Case 11 Ear Reconstruction

11.1 Description
Fungating and ulcerative mass involving the upper two-thirds of the left ear, including the helix, scapha, and antihelix
Surrounding edema, induration, and discoloration of the skin
Lesion has high suspicion for malignancy
11.2 Work-Up
11.2.1 History
Length of time the lesion has been present
Associated symptoms: pain, itching, bleeding, and hyperkeratosis
History of sun exposure
Personal and family history of skin cancer
11.2.2 Physical Examination
Thorough examination of the ear, including size and shape of lesion
Characterize findings associated with skin lesion (if present): Size, color, shape of lesion, skin irregularity, and hyperkeratosis
Depth of lesion and likelihood for cartilaginous or full-thickness involvement.
Lymph node examination
Full body integument examination
11.2.3 Diagnostic Studies
If patient presents initially without resection, a biopsy should be performed at the time of evaluation to establish a diagnosis.
Full-thickness incisional versus excisional biopsies may be performed. Avoid shave biopsies.
When the likelihood of cancer is high, as in this case, take multiple biopsies along the periphery.
11.3 Patient Counseling
Attempts at reconstruction may result in ear deformities, including a smaller or less projecting ear
The poor blood supply of the auricular cartilage puts these cases at higher risk of infection, particularly chondritis
Patients must be made aware that with large malignant lesions, amputation may be a possibility
11.4 Treatment
For skin malignancies, consider Mohs surgery, if available (see Table 7.1)
Allows examination of complete surgical margins, resulting in highest cure rates
Board examiner may require that you excise it yourself
Excision (see Chapter 7 for margins required for different types of malignancies)
Reconstruction
Should be delayed until negative margins are confirmed on final pathology
Fresh frozen pathologic evaluation cannot ensure negative margins
Local wound care, Integra, or temporizing skin graft in interim
Antibiotic coverage
Sulfamylon (topical) and fluoroquinolones (systemic) have excellent cartilaginous penetration
11.4.1 Reconstructive Ladder
Primary closure +/– Tanzer’s excision patterns (Fig. 11-1)
Wedge resection: Defect <1.5cm
Skin grafts may be used for superficial defects
Usually harvested from contralateral posterior auricular ear
Skin graft cannot be placed on raw cartilage without overlying perichondrium
Exposed raw cartilage must be covered by flap or debrided
Helical rim advancement (Fig. 11-2)
Useful for defects of helical rim
Chondrocutaneous flaps are advanced into the defect
Antia-Buch flap (Fig. 11-3)
Useful for upper 1/3 helical defects
The base of the helix is advanced in V-Y fashion and coupled with helical rim advancement from below
May result in decrease in height of ear
Posterior auricular flap: Large flap of skin from behind the ear can be advanced to cover the posterior ear
Typically used in a staged fashion for initial coverage followed by additional release and further reconstruction, possibly with skin graft
Tubed pedicle flap from postauricular skin
Useful to reconstruct longer sections of missing helical rim
Must be divided in second stage
Banner flap: Skin flap based on anterosuperior auriculocephalic sulcus
Combine with contralateral auricular cartilage graft for larger (>2cm) defects
Chondrocutaneous transposition flaps: Often require grafting of donor site
Converse flap: Contralateral auricular cartilage graft tunneled under skin flap from mastoid, requires second stage (3 weeks) for division and inset
Orticochea procedure: Based laterally on helix
Davis flap: Based anteriorly on crus helicis, from conchal bowl
Temporoparietal fascia (TPF) flap
Thin flap of TPF may be harvested from scalp based on superficial temporal artery
Large flap (10×12 cm) may be elevated for complete coverage of the ear, if necessary
Total ear reconstruction (see Chapter 20)
Autologous rib cartilage framework covered with posterior auricular skin or TPF flap and skin graft
Medpor construct covered with TPF flap and skin graft
Complete amputation/avulsion: Replantation if viable blood supply is available (e.g., superficial temporal or posterior auricular artery)
External auditory canal
Maintenance of patency more important than choice of coverage
May use skin graft over vascularized bed
Requires use of stent or splint for 6 months
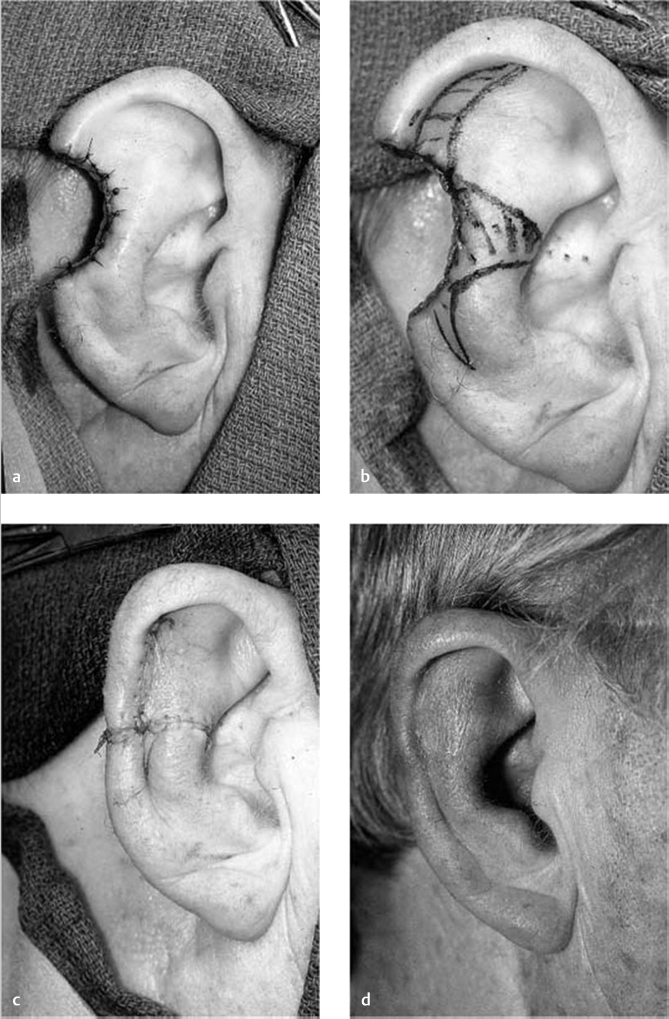
Fig. 11.1 (a-d) Wedge resection and primary closure with excision of accessory triangles. (Source: Unit Defects. In: Day T, Farrior E, Frodel J et al., ed. Facial Plastic Surgery. The Essential Guide. Thieme; 2005.) 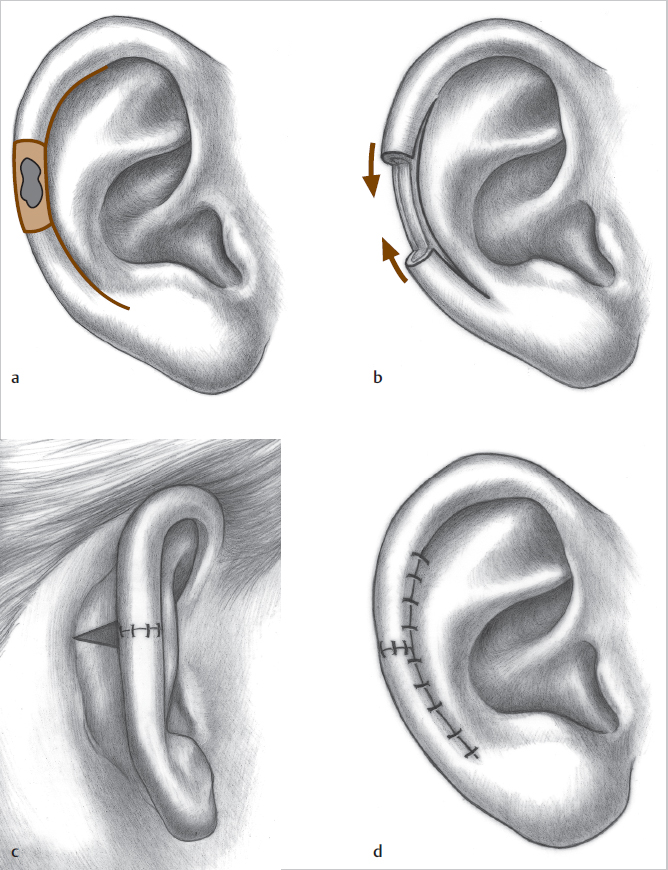
Fig. 11.2 (a-d) Helical rim advancement. Incision is made in the scapha and a chondrocutaneous flap is advanced into the defect in the helical rim. (Source: Ears. In: Sherris D, Larrabee Jr W, ed. Principles of Facial Reconstruction. A Subunit Approach to Cutaneous Repair. 2nd Edition. Thieme; 2009.) 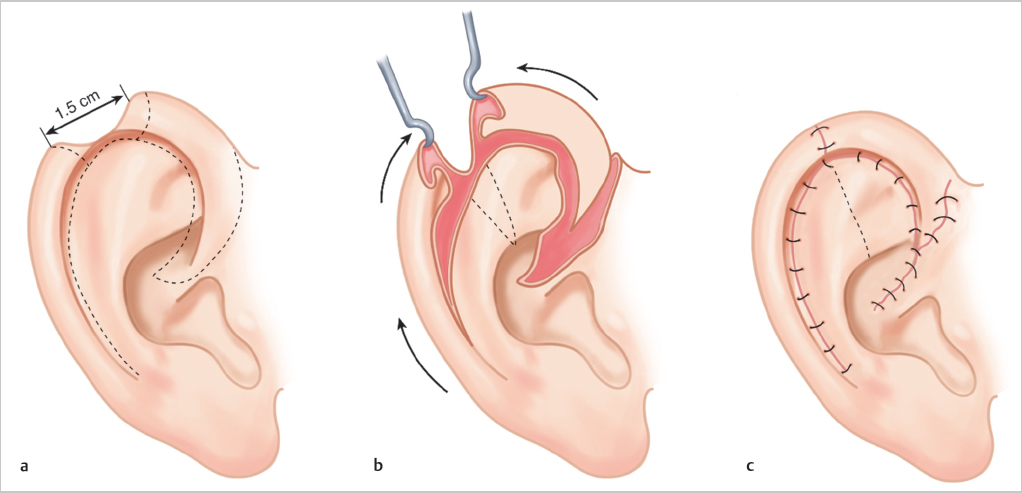
Fig. 11.3 (a,b) Antia-Buch flap. The base of the helix is advanced posteriorly in a V-Y fashion.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


