Canthopexy
Adam R. Sweeney
Christopher B. Chambers
DEFINITION
Canthopexy is a resuspension of the canthus to the bony orbit used to treat eyelid laxity, ectropion, or misalignment.
A common surgery in adult facial rejuvenation, canthopexy is an indispensable tool for treating children with eyelid positioning defects or deformities.
ANATOMY
The canthal tendons maintain the shape of the palpebral fissure and also maintain lid apposition to the globe, important for proper corneal lubrication and tear drainage.
The medial canthus has origins at the anterior and posterior lacrimal crests that fuse temporal to the lacrimal sac, enveloping the lacrimal sac. The medial canthus then divides into upper and lower segments that attach to the tarsus of the upper and lower lid.
The medial canthus is involved in the lacrimal pump mechanism and intimately associated with the lacrimal sac.
The lateral canthal tendon originates at the lateral orbital tubercle 4 to 5 mm posterior to the lateral orbital rim. This provides a posterior vector opposing the lid to the globe. The lateral canthal tendon then splits into superior and inferior segments that attach to the tarsal plates (FIG 1).
The lateral canthal tendon inserts approximately 2 mm higher than does the medial canthal tendon. This creates a superior tilt to the palpebral fissure moving laterally.
The orbital septum overlies the lateral canthus as it approaches the orbital rim and acts as a “superficial lateral canthus,” which can be used for suspension in mild cosmetic defects.1
PATHOGENESIS
Common conditions that may cause eyelid laxity or malposition including congenital facial clefting (ie, Tessier 2 to 12 clefts), amniotic band syndrome, congenital eyelid malposition, or deformities resulting from other etiologies including trauma and cancer resection or from craniofacial manipulation (iatrogenic)
NATURAL HISTORY
Eyelid laxity is both a cosmetic and a functional problem.
Uncorrected, lower lid laxity may cause exposure keratopathy, epiphora, or problems with the lacrimal pump mechanism.
PATIENT HISTORY AND PHYSICAL FINDINGS
Lower eyelid laxity
Canthal dystopia
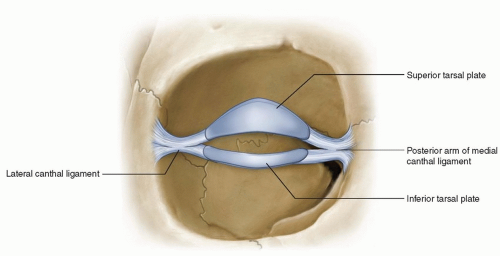
FIG 1 • Anatomy of the medial and lateral canthal tendons.
Poor eyelid snap back test: This test refers to evaluating the time for the eyelid to return to normal position after pulling the lower lid down and away from the globe. It is graded from 0 (brisk snap back) to IV (severe laxity).
Eyelid distraction—5 mm of eyelid distraction often considered excessively lax.
Dry eye including exposure keratopathy or punctate epithelial erosions
Punctual stenosis from keratinization of the lid margin in medial ectropion2
IMAGING
CT imaging of the face is appropriate in the evaluation of congenital craniofacial abnormalities. In the setting of orbital trauma, CT imaging is useful to assess for nasoorbital-ethmoid fractures.
NONOPERATIVE MANAGEMENT
In patients not bothered by the cosmetic defect, scheduled application of lubricant artificial tears may provide the necessary corneal protection to defer or prevent surgery in mild cases.
Careful attention must be made to prevent deprivation amblyopia by constant application of ointments, taping the eyelid shut, or patching of the eye.
SURGICAL MANAGEMENT
If the cosmetic defect is bothersome or the patient is symptomatic, canthopexy, canthoplasty, or both may be performed to correct the eyelid abnormality.
Preoperative Planning
General anesthesia is recommended for pediatric cases.
Preoperative photos should be reviewed assessing the degree of malpositioning and marking of the face at the desired canthi position to create the proper slight superolateral contour of the eyelid with appropriate eyelid tightening achieved.
Positioning
Patients should be positioned supine in an operating bed with adjustable head positioning. The contralateral eyelid may be temporarily taped shut or lubricated rather than covered to serve as a reference point during surgery.
Approach
Medial, lateral, or a combination of approaches may be performed depending on the location of the lid abnormality or the desired results.
TECHNIQUES
▪ Lateral Canthopexy
The lateral canthopexy procedure tightens the canthal tendon with sutured reconstruction of the canthal tendon. This effectively tightens the eyelid.
Place 2 drops of topical tetracaine on the conjunctival surface.
Inject 1 to 2 cc 2% lidocaine with 1:100 000 epinephrine subcutaneously above and below the lateral canthus.
Using a no. 15 blade, make a 1-cm horizontal subciliary incision at the lateral canthal angle (TECH FIG 1A).
Retract the skin with skin hooks and bluntly dissect down to the periosteum using blunt-tipped scissors.
Undermine and dissect in this plane to the lateral canthal tendon under the orbital septum (TECH FIG 1B).
The lateral canthal tendon is identified by tension and the ability to “strum” if manipulated by closed blunttipped scissors. Grasping the lateral canthal tendon, vertically transect the lateral canthal tendon at its lateral insertion taking care to avoid the levator aponeurosis (TECH FIG 1C).
Pass a double-armed 4-0 Vicryl suture on a P-2 needle (Ethicon, Somerville, NJ) entering anteriorly through the lateral canthus at its transected superior and inferior attachment points (TECH FIG 1D).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree