Breast Reconstruction: A Review and Rationale for Patient Selection
Maurice Y. Nahabedian, M.D.
Washington, D.C.
From the Department of Plastic Surgery, Georgetown University Hospital.
Received for publication January 15, 2008; accepted August 22, 2008.
Copyright © 2009 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e31818b8c23
Disclosures: Dr. Nahabedian serves on the speakers’ bureau for LifeCell Corporation (Branchburg, N.J.) and lectures on the use of AlloDerm for breast reconstruction. He is not a consultant. The author has no financial interest to declare in relation to the content of this article.
Summary: The importance of good patient selection is becoming increasingly appreciated as a predictor of good outcomes following mastectomy and reconstruction. There are many variables that should be considered when making these decisions. Patient variables include breast characteristics, age, body habitus, comorbidities, and expectations. Oncological variables include tumor size, cancer stage, and perioperative radiation. This article is structured to review the variables that are relevant when deciding upon a particular reconstructive option for a particular patient. (Plast. Reconstr. Surg. 124: 55, 2009.)
The importance of patient selection as a determinate of good outcomes in plastic surgery is well accepted. Its importance is becoming increasingly recognized in the patient with breast cancer who is interested in reconstruction. Although reconstructive in nature, the aesthetic importance of breast reconstruction following mastectomy cannot be underestimated. Achieving a highly desirable outcome can be difficult in many women. There are numerous variables that must be considered when selecting the appropriate operation. Patient-related factors include breast size, volume, and contour, as well as body weight and habitus. Oncological factors include tumor size, cancer stage, and previous or future radiation therapy, as well as whether the reconstruction is immediate or delayed. Psychological factors include an assessment of expectations, both realistic and unrealistic, as well as preconceived notions of the reconstructive option desired. Surgeon factors include the technical ability to perform the various reconstructive operations in a predictable and reproducible manner. These variables all contribute to the complexity of the reconstructive process.
It is the intent of this article to review a single surgeon’s approach to patient selection. The specific details of the article are based on personal experience dating from July of 2005 to June of 2007; however, the principles and concepts are based on having personally performed breast reconstruction in more than 1000 women over the past 10 years. The goal is to provide a framework for optimizing patient evaluation with the ultimate selection of the reconstructive option that will optimize outcomes.
Patients
Between July of 2005 and June of 2007, a total of 236 women had primary breast reconstruction following mastectomy. The reconstruction was unilateral in 161 women and bilateral 75 women, totaling 311 breasts. The reconstruction was completed with prosthetic devices in 61 women (25.8 percent) and autologous tissue in 175 women (74.2 percent). Of those women with prosthetic devices, the reconstruction was unilateral in 39 women (63.9 percent) and bilateral in 22 women (36.1 percent), totaling 83 breasts. Of those women who had autologous tissue repair, the reconstruction was unilateral in 122 women (69.7 percent) and bilateral in 53 women (30.3 percent), totaling 228 breasts. The specific type of autologous reconstruction included the muscle-sparing free transverse rectus abdominis musculocutaneous (TRAM) flap in 26 women (34 flaps), the deep inferior epigastric perforator (DIEP) flap in 128 women (172 flaps), superior gluteal artery perforator flap in eight women (11 flaps), and the latissimus dorsi flap in 11 women.
Principles of Patient Selection
Patient selection begins with a thorough evaluation of the history and physical examination, progresses to a review of the reconstructive options, and ends with an understanding of patient expectations and surgeon recommendations. Women are educated and counseled to understand the differences between the various reconstructive options. Some women are interested in a short operation with a rapid recovery, whereas others are less interested in the duration of the procedure or the recovery but more interested in a procedure that will last forever. Some women are interested in autologous reconstruction because they do not want prosthetic materials in their body. It is incumbent upon the plastic surgeon to understand what the patient desires and to review the appropriate options to facilitate the decision-making process.
In a typical consultation, a pertinent history and physical examination are performed. Important details include body weight, patient height, body mass index, and bra size. The importance of symmetry following the first operation or following subsequent operations is determined. In general, most women who seek autologous reconstruction are candidates using the abdomen, the gluteal region, or the posterior thorax. Prosthetic reconstruction is generally used for women who desire a quick recovery with minimal downtime or for women with insufficient donor sites. Many women are curious about the safety of silicone gel implants based on the previous moratorium that limited their use.1 It is explained that there is significant scientific evidence that supports the safety and efficacy of these devices and that the results following breast reconstruction with silicone gel implantation are usually superior to that of saline implants.
Another important component of the consultation includes a review of schematic illustrations as well as preoperative and postoperative photographs. Typically, the patient is shown a poor result, a good result, and an excellent result. Results are shown at the various stages of the reconstruction (e.g., fresh incision, red scar, breast mound with a nipple, nipple without a tattoo, and so on). Both prosthetic and autologous outcomes and morbidities are demonstrated showing photographs. The morbidities include flap failure, abdominal bulge, delayed healing, rippling and wrinkling, and prosthetic removal. My practice is not to raise one’s expectations or to sell a particular operation but rather to convey a realistic picture of what to expect.
Patient Selection Based on Cancer Stage
The foundation for safe and effective breast reconstruction is to appreciate not only the aesthetic desires of the patient but also her oncological concerns. Several studies have demonstrated that breast reconstruction following mastectomy will not promote cancer growth or interfere with surveillance.2,3 It is therefore generally accepted that immediate breast reconstruction can be safely performed in women with early-stage breast cancer. In women with advanced breast cancer, however, delayed breast reconstruction is usually recommended.
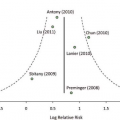
Occasionally, some women with locally advanced breast cancer will request immediate breast reconstruction. A motivating factor has been to maintain quality of life and femininity. The important question that needs to be raised is whether or not these women should undergo immediate breast reconstruction based on their oncological risks. It is well established that immediate breast reconstruction does not delay the initiation of adjuvant treatments, such as chemotherapy or radiation therapy. However, are the aesthetic and oncological outcomes affected by these adjuvant treatments? In women with locally advanced breast cancer, postoperative radiation therapy is almost always a certainty. Review of the literature demonstrates mixed results when analyzing the effects of radiation on the aesthetic quality of the reconstruction.4–8 With prosthetic devices, there is an increased risk of capsular contracture, infection, and premature removal.4,5 With autologous tissue, there is an increased risk of fat necrosis, distortion, and shrinkage, although no change is also a possibility.6,7 With regard to oncological safety, some studies have concluded that immediate breast reconstruction in the setting of locally advanced breast cancer is safe and effective7,8; however, this has not been my personal observation. In a review of 146 women who had breast cancer, mastectomy, and breast reconstruction either before or after radiation therapy, there was noted to be a higher local recurrence rate when the reconstruction preceded the radiation (27 percent) compared with when the radiation preceded the reconstruction (14.9 percent).9 Local recurrence in the setting of autologous reconstruction was 38 percent when radiation followed immediate breast reconstruction and 14 percent when radiation preceded breast reconstruction
(p = 0.0146). The recurrence rate associated with implant reconstruction was 10 percent when radiation followed immediate breast reconstruction and 19 percent when radiation preceded breast reconstruction (p = 0.0424).
(p = 0.0146). The recurrence rate associated with implant reconstruction was 10 percent when radiation followed immediate breast reconstruction and 19 percent when radiation preceded breast reconstruction (p = 0.0424).
Autologous Versus Prosthetic
Traditional dogma has dictated that women with small breast volumes are better candidates for reconstruction using prosthetic devices and that women with large breast volumes are better candidates for reconstruction using autologous tissue. Current concepts in breast reconstruction imply that type of reconstruction selected is not as dependent on breast volume alone as previously thought. The reality is that prosthetic or autologous reconstruction can safely be performed in women with a variety of breast sizes and shapes (Table 1).
With the advancements in breast reconstruction, it is not uncommon to reconstruct women with cup sizes ranging from A to D with either a flap or prosthetic device. As previously discussed, an important aspect is the recognition of what a woman’s goals and expectations are following the reconstruction. When evaluating women for autologous breast reconstruction, several factors are noted. The abdomen has been the donor site of choice for most women. In general, the most important physical finding is a sufficient quantity of skin and fat to reconstruct the desired breast volume. Most women have experienced previous childbirth and have an excess of abdominal skin and fat.10 Although a woman may be slender with a paucity of abdominal fat, she may still be a candidate if the reconstructive requirements are low. In women who are overweight or obese, an abdominal flap in the form of a free TRAM or DIEP flap can still be performed; however, the flap must be tailored to sustain its perfusion requirement and to minimize the incidence of fat necrosis.11–13 The abdomen is usually not considered when there are midline scars that will preclude incorporating the contralateral zones when additional tissue is deemed necessary or there is minimal to no excess fat in the region.
Table 1. Indications for Autologous and Prosthetic Breast Reconstruction | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
Should the abdomen not be a suitable donor site, then the gluteal region is considered. The superior artery gluteal perforator flap is ideal for women who desire autologous reconstruction, refuse prosthetic reconstruction, and prefer a perforator flap.14 Most women will have sufficient donor fat in this area and will be candidates. An important caveat about this operation is the appearance of the donor site. It has been observed that some will have significant scalloping of the buttock and/or gluteal asymmetry. This has been a major source of dissatisfaction in some women. In general, I have found that petite women of shorter stature are more prone to these aesthetic issues, whereas taller and slender women are less prone.
When considering women for prosthetic reconstruction, it is important to assess the potential for symmetry. Secondary procedures are more common following prosthetic reconstruction and may involve the ipsilateral or contralateral breast.15 As a means of minimizing these secondary procedures, ideal candidates for prosthetic reconstruction include those with small to moderate breast volume and with minimal to no ptosis. This is especially true in the unilateral setting in which obtaining symmetry is generally more difficult. In the setting of bilateral reconstruction, the specific characteristics of the breast are less important because the two reconstructed breasts will be very similar. Poor candidates for prosthetic reconstruction are those who have had previous radiation following mastectomy or following breast conservation therapy. Complications such as infection, capsular contracture, distortion, pain, and premature removal are more common in this setting.4,5
Related posts:
 Radiation Therapy and Breast Reconstruction: A Critical Review of the Literature
Radiation Therapy and Breast Reconstruction: A Critical Review of the Literature
 The Oncologic Outcome and Immediate Surgical Complications of Lipofilling in Breast Cancer Patients: A Multicenter Study—Milan-Paris-Lyon Experience of 646 Lipofilling Procedures
The Oncologic Outcome and Immediate Surgical Complications of Lipofilling in Breast Cancer Patients: A Multicenter Study—Milan-Paris-Lyon Experience of 646 Lipofilling Procedures
 A Meta-Analysis of Human Acellular Dermis and Submuscular Tissue Expander Breast Reconstruction
A Meta-Analysis of Human Acellular Dermis and Submuscular Tissue Expander Breast Reconstruction
 Techniques of mastectomy: tips and pitfalls
Techniques of mastectomy: tips and pitfalls
 Mastectomy and Immediate Expander Reconstruction for Local Breast Recurrence After Previous Quadrantectomy and Radiation
Mastectomy and Immediate Expander Reconstruction for Local Breast Recurrence After Previous Quadrantectomy and Radiation
 Patient Selection
Patient Selection
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


