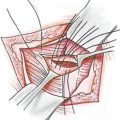
Fig. 3.1
View of the abdomen of a massive-weight-loss patient in diver’s position after belt lipectomy. Vertical skin excess has been removed; however, horizontal skin excess still persists. A fleur-de-lys procedure was performed afterwards
The amount of vertical skin excess also determines the length of the incision. Lateral skin excess can be removed by high lateral tension abdominoplasty [23]. However, if the skin excess is circumferential, especially in massive-weight-loss patients, a belt lipectomy procedure should be considered [24].
3.3.2 Subcutaneous Fat
The amount and location of the subcutaneous fat should be examined carefully. In lipoabdominoplasty procedures, liposuction is a part of the operation. Wide liposuction allows easy mobilization of the abdominal skin without undermining, and contrary to the common belief, it is a safe procedure in terms of blood circulation [25]. The areas to be suctioned should be determined and marked preoperatively. In body sculpting procedures, whole abdomen, pubic area, flanks, back, and trochanteric areas are suctioned prior to abdominoplasty. Also fat injections to the gluteal area and supratrochanteric depressions should be considered, if necessary. Ultrasonic techniques, such as VASER, are getting more popular in abdominal shaping. Hi-def liposuction with VASER allows surgeon to create anatomical details such as six-pack abs [26]. Precise liposhaping should be considered only in patients with ideal weight and sporting regularly.
Patients with good skin quality and skin excess can be treated with liposuction alone. Hi-def procedures can also be considered in selected patients. However, it should always be kept in mind that excessive liposuction, even in young patients with tight skin, may result in irregularities especially in the hypogastric area and skin accumulation just over the umbilicus (Fig. 3.2).

Fig. 3.2
It should be remembered that even in young, nulliparous patients with good skin quality, excessive liposuction might result in skin irregularities
3.3.3 Intra-abdominal Fat
Visceral fat accumulation occurs with age and is more likely to be found in men. Women also accumulate this type of fat as they approach menopause. Alcohol consumption also increases visceral fat accumulation. These patients usually have a distended abdomen with a little subcutaneous fat. The presence of substantial visceral fat accumulation prevents any successful result even if extensive muscular tightening would be performed (Fig. 3.3). It should be kept in mind that patients with excessive intraperitoneal fat cannot be treated by any abdominal contour procedure [27]. Such patients are contraindicated for any abdominal surgery may it be liposuction or abdominoplasty. These patients are directed to dieticians or bariatric surgery centers. It should also be remembered that patients with that body type are under more risk of cardiac problems [28].

Fig. 3.3
Patient with significant intra-abdominal fat accumulation and lumbar lordosis. Although a full abdominoplasty was performed, there is no improvement except for adding an ugly scar
3.3.4 Abdominal Wall
Musculofascial laxity is common in patients with multiple pregnancies or after massive weight loss. In majority of male patients, abdominal wall laxity is not present and there is no need for myofascial tightening [29]. Abdominal wall laxity is best determined while the patient is wanted to do crunches in supine position. Ventral and periumbilical hernias can also be examined in the same way. A thick subcutaneous fat layer may obscure the hernia, and careful examination should be performed [20, 21]. In patients with visceral fattening, even in presence of abdominal wall laxity, operation should be postponed after weight loss.
As indicated previously in the chapter, myofascial tightening may cause respiratory disturbances and should be done either conservatively or cancelled in patients with respiratory problems [27].
3.3.5 Position of the Umbilicus
Patients with high-seated umbilicus do not have enough excess skin to allow traditional abdominoplasty without a high transverse or vertical midline scar. If there is no skin excess above the umbilicus, a mini-abdominoplasty procedure combined with liposuction could be good solution. If there is skin excess above the umbilicus with myofascial laxity, floating umbilicus technique with low placement of a full transverse abdominal scar, abdominal flap undermining, more inferior umbilical repositioning, flank liposuction, and plication of diastasis recti from xiphoid to pubis should be considered [30]. If the skin excess is not present, endoscopic myofascial repair and inferior repositioning of the umbilicus may be a better solution [31] (Fig. 3.4)
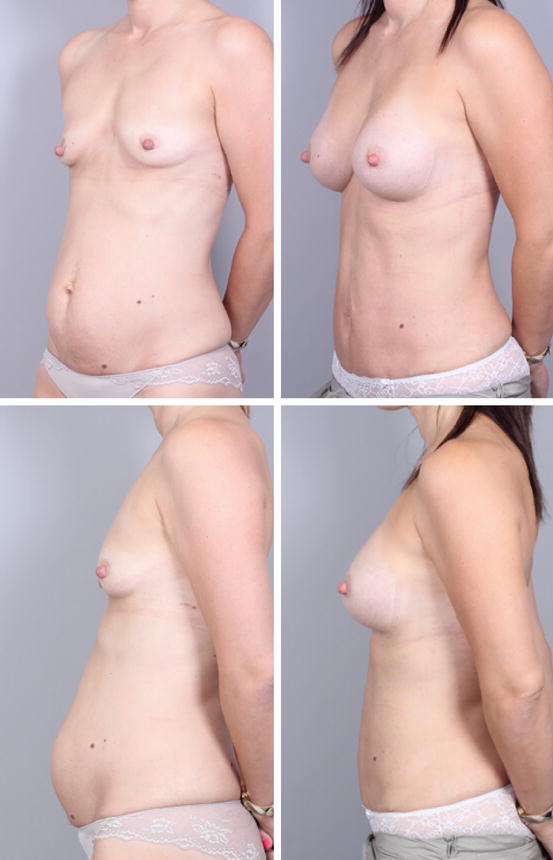
Fig. 3.4
Floating umbilicus procedure with myofascial repair, inferior repositioning of the umbilicus, skin resection from the lower abdomen, combined with breast augmentation (14 months postoperatively)
3.4 Technique Selection
There is a wide spectrum of surgical techniques varying from liposuction to belt lipectomy, depending on the abdominal deformity and tissue characteristics [32]. Surgical strategies are summarized as an algorithm for the technique selection is presented in Table 3.1:
Table 3.1
Technique selection
Patient and tissue characteristics | Technique |
|---|---|
Young, nulliparous patient Good skin quality No skin excess No abdominal wall laxity | Liposuction only |
Good to moderate skin quality High-seated umbilicus No skin excess above the umbilicus Moderate skin excess below the umbilicus No abdominal wall laxity | Mini-abdominoplasty Skin resection from the lower abdomen Liposuction (±) |
Good to moderate skin quality No skin excess Abdominal wall laxity (+) | Endoscopic abdominoplasty Myofascial repair No skin excision Liposuction (±) |
Good to moderate skin quality Minimal skin excess above the umbilicus Moderate skin excess below the umbilicus High-seated umbilicus Abdominal wall laxity (+) | Floating umbilicus technique Inferior repositioning of umbilicus Skin resection from the lower abdomen Liposuction (±) |
Moderate to bad skin quality Skin excess both above and below the umbilicus Abdominal wall laxity (+) | Full abdominoplasty∕lipoabdominoplasty Myofascial repair Liposuction (±) |
Bad skin quality Skin excess both above and below the umbilicus Skin excess laterally Abdominal wall laxity (+) | High lateral tension abdominoplasty Myofascial repair Liposuction (±) |
Massive-weight-loss patient Bad skin quality Skin excess both above and below the umbilicus Circumferential skin excess Abdominal wall laxity (+) | Belt lipectomy Myofascial repair Liposuction (±) |
Massive-weight-loss patient Bad skin quality Skin excess both above and below the umbilicus Circumferential skin excess Horizontal skin excess Abdominal wall laxity (+) | Belt lipectomy Fleur-de-lys-type skin resection Myofascial repair Liposuction (±) |
Excessive intra-abdominal fat accumulation
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|