Class
Visceral fat
Skin elasticity
Musculofascial tonus
Treatment
Class I
−+
Good
Good
Liposuction
Class II
−+
Good
Moderate
Endoscopic abdominoplasty
Class III
−+
Average
Moderate
Mini-abdominoplasty
Class IV
−+
Poor
*
Inverse abdominoplasty
Class V
++
*
*
No surgery
If the mentioned skin problems affect majorly the infraumbilical area, a reverse mini-abdominoplasty and a full-length abdominal wall plication with or without floating umbilicus might be enough to get an excellent result. Similarly, if the skin quality is generally good but the existing wall laxity is considerable, again, a mini-abdominoplasty together with or without liposuction shall be chosen [7]. Another indication for an inverse mini-abdominoplasty is a case when the downward traction asserted to the abdominal skin demonstrates an absence of sufficient laxity to bridge the gap of a full abdominoplasty. Whether a mini-abdominoplasty with floating umbilius or not is to be performed, depends on the vertical location of the umbilicus. If the umbilicus is proximal to the mid-level of the ksiphoid-pubis height, a floating umbilicus is indicated. If the umbilicus is between 1/2 and distal 1/3 of the vertical abdominal height, relocating the umbilicus further down should not be performed since it would distort the abdominal harmony [8] (Fig. 6.1).

Fig. 6.1
If the umbilicus is vertically above the mid-level of the ksiphoid-pubis height a floating umbilicus is indicated. If the umbilicus is distally between 1/2 and 1/3 of ksiphoid-pubis height, a mini-abdominoplasty without a floating umbilicus is preferable, since moving the umbilicus further distally would distort the harmony of the abdomen. Usually a full abdominoplasty is performed if the umbilicus is distal to 2/3 of the abdominal height
It should be noted that performing mini-abdominoplasty without a full abdominal plication is a sure way to patient dissatisfaction. This is also valid for an incomplete plication covering only the lower part of the abdomen. In such a case, the tightening of the lower abdomen might even result in bulging of the upper abdomen.
The presence of substantial visceral fat accumulation prevents any successful result even if extensive muscular tightening would be performed. Such patients are contraindicated for any abdominal surgery, may it be liposuction or abdominoplasty, and are directed to dieticians or bariatric surgery centers.
Contraindications to mini-abdominoplasty are excessive skin and soft tissue in the upper abdomen, generalized laxity or soft-tissue excess of the entire abdominal wall, and patients presenting after massive weight loss.
Even though the candidates for mini-abdominoplasty are usually younger, healthier, and fitter than patients requiring more extensive procedures, any personal or family history of deep vein thrombosis (DVT) and/or pulmonary embolism (PE) is very important, and standard precautions should be taken due to the fact that like all forms of abdominoplasty this procedure also includes myofascial plication [9]. General precautions like cessation of smoking are important in all types of abdominoplasty procedures and should begin several weeks before and continue after the procedure [10–12].
Things to Remember
Even though the candidates for mini-abdominoplasty are usually younger, healthier, and fitter, standard precautions should be taken due to the fact that, like all forms of abdominoplasty, this procedure also includes myofascial plication.
The presence of substantial visceral fat accumulation prevents any successful result even if extensive muscular tightening would be performed. Such patients are contraindicated for any abdominal surgery.
6.3 Surgical Technique
6.3.1 Marking
Initially, preoperative photographs are taken in anterior, bent, right and left oblique, and right and left lateral views. Patients are marked in a standing position to delineate the areas for liposuction and skin incisions, wearing their preferred undergarments to confine the incision within the boundaries of her clothing.
Marking starts with a midline drawing from the xyphoid to the umbilicus and to the anterior vulvar commissure with the patient standing, which will serve also as a reference line to facilitate symmetry and to better appreciate any excess of tissue on either sides. Two paramedian vertical lines are also drawn 5–6 cm off the midline symmetrically.
Holding the skin excess in the lower abdomen, a curvilinear incision is marked in the natural inferior skinfold, extending in length slightly beyond the lateral skinfolds with the patient in a lateral hip-flexed position. A seagull shape superior line is designed around 7–8 cm inferior to the umbilicus. This superior horizontal line is drawn gently upward, peaking up around 5–6 cm away on both sides from the midline at the paramedian lines, and then curves downward toward the lateral endings of the inferior incision line. The amount of skin to be removed is double-checked by the surgeon grasping the skin and confirming that the upper and lower incisions meet (Fig. 6.2).

Fig. 6.2
A seagull shape is designed around 7–8 cm inferior to the umbilicus. This superior horizontal line is drawn gently upward, peaking up around 5–6 cm away on both sides, and then curving toward the lateral endings of the inferior incision line
Simultaneously, the marking for the concurrent liposuction is drawn to address all areas of excess adiposity. This might include the entire abdomen, flanks, and mons pubis area. In inverse mini-abdominoplasty, the liposuction might be an important element in substantial majority of cases.
The definitive markings for the real amount of tissue resection are done on the operating table. The patients are dressed with thromboembolic deterrent stockings before they are called to the OR.
6.3.2 Positioning and Planning
Unless indicated otherwise, the surgery is usually performed under general anesthesia. In the OR, the operating table is checked to insure that it can be flexed prior to induction of anesthesia. The patient is placed in a supine position with silicone pillows under the knees to prevent nerve compressions during the surgery.
Afterward, the symmetry of the body and the arms is verified; a rolled towel of 5–10 cm in diameter is positioned behind the back of the patient at the level of the scapulae in order to decrease the unnatural backward leaning of the thorax, and the arms are loosely secured by wrapping them with gauze. A Foley catheter is inserted, sequential pneumatic compression devices are placed, and if indicated, anticoagulants are used.
To guarantee symmetry a 2-0 silk suture is placed in the midline at the level of the xyphoid. Vertical parallel lines to the midline at 5, 10, and 15 cm are drawn, and a symmetrical upper incision line with a seagull shape is obtained at the crossing of the vertical lines using the silk suture. The same drawing is performed for the planned lower incision.
If any liposuction is planned, it is performed immediately in the beginning of the abdominal procedure. The mini-abdominoplasty is done once the suction is completed (Fig. 6.3).

Fig. 6.3
To achieve symmetry a 2-0 silk suture is placed in the midline. Vertical parallel lines at 5, 10, and 15 cm are drawn, and a symmetrical upper incision line with a seagull shape is obtained at the crossing of the vertical lines using the silk suture. Afterward, the inferior incision line is drawn
Points to Remember
The operating table is checked to ensure that it can be flexed prior to induction of anesthesia.
A rolled towel is placed under the back at the level of each scapula bones to mimic natural standing position.
Vertical parallel lines at 5, 10, and 15 cm are drawn, and a symmetrical upper incision line with a seagull shape is obtained at the crossing of the vertical lines using the silk suture. The same drawing is performed for the lower planned incision.
6.3.3 Incision and Upper Flap Elevation
First, the upper incision is made. A slightly beveled incision through the cutis is made through the superior seagull shape marking, while pulling the skin only downward in order to achieve proper cutting angle (Fig. 6.4).
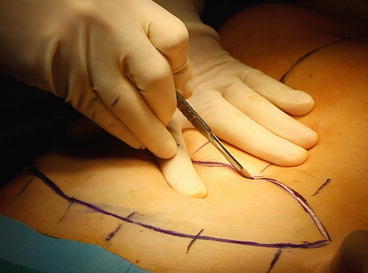
Fig. 6.4
A slightly beveled incision through the cutis is made through the superior seagull shape marking to achieve proper cutting angle, which will be beneficial for scar healing due to better suture line elevation
Then, the blade bevels more to lie at 30° to the surface of the flap so the Scarpa’s fascia portion of the flap is about 1 cm shorter than the skin portion. This maneuver will ensure the scar-edge elevation and an appropriate skin closure with good scar healing at the end of the surgery. The bilateral upward curves of the incision are designed to create a relative paramedian skin gap and median skin excess.
The supra and sub-scarpal fat is transversed until the surgeon reaches the abdominal wall. The large vessels are suture-ligated, and the rest of the dissection is done by electrocautery or harmonic scalpel, leaving the fine areolar tissue and their lymphatics over the fascia.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


