Age
Test
12–40a
CBC (complete blood count)
40–60
CBC, EKG
60↑
CBC, EKG, BUN, CXR, glucose
Certain risk factors such as undiagnosed hypertension, cardiac arrhythmia, or bronchial asthma can be detected with preoperative physical examination. Risk assessment in terms of intubation by considering the head and neck structure of the patient is essential. Preoperative assessment of the patient by an anesthetist is an appropriate and necessary approach for both planning the anesthesia to be applied to the patient and minimizing the perioperative risks.
Many authors agree on common points in morbidity and mortality: performing more than one procedure at a time, prolonged surgeries, significant blood loss, and wide invasive surgeries have increased perioperative complication risks. In order to minimize the risk of cardiopulmonary complications and optimize tissue perfusion in liposuctions, the aspired amount must be less than 5 % of the body weight and 30 % of the body surface, as a rule [17].
The most common method in preoperative risk evaluation is the ASA (American Society of Anesthesiologists) classification. Table 2.2 demonstrates the ASA classification which was extended and accepted in 2014 [18].
ASA PS classification | Definition | Examples include but not limited to |
|---|---|---|
ASA I | A normal healthy patient | Healthy, non-smoking, no or minimal alcohol use |
ASA II | A patient with mild systemic disease | Mild diseases only without substantive functional limitations. Examples include (but not limited to) current smoker, social alcohol drinker, pregnancy, obesity (30< BMI <40), well-controlled DM/HTN, mild lung disease |
ASA III | A patient with severe systemic disease | Substantive functional limitations; one or more moderate to severe diseases. Examples include (but not limited to) poorly controlled DM or HTN, COPD, morbid obesity (BMI ≥40), active hepatitis, alcohol dependence or abuse, implanted pacemaker, moderate reduction of ejection fraction, ESRD undergoing regularly scheduled dialysis, premature infant PCA <60 weeks, history (>3 months) of MI, TIA, or CAD/stents |
ASA IV | A patient with severe systemic disease that is a constant threat to life | Examples include (but not limited to) recent (<3 months) MI, CVA, TIA, or CAD/stents; ongoing cardiac ischemia or severe valve dysfunction; severe reduction of ejection fraction; sepsis; DIC; ARD; or ESRD not undergoing regularly scheduled dialysis |
ASA V | A moribund patient who is not expected to survive without the operation | Examples include (but not limited to) ruptured abdominal/thoracic aneurysm, massive trauma, intracranial bleed with mass effect, ischemic bowel in the face of significant cardiac pathology, or multiple organ/system dysfunction |
ASA VI | A declared brain-dead patient whose organs are being removed for donor purposes | |
Things to Remember: Box 2.5
Risk Factors
Undiagnosed hypertension
Cardiac arrhythmia
Bronchial asthma
More than one procedure at a time
Prolonged surgeries
Significant blood loss
Wide surface-invasive surgeries
Things to Remember: Box 2.6
Preoperative evaluation forms provide very essential information.
ASA classification must be performed.
Things to Remember: Box 2.7
The amount aspired in liposuctions which is less than 5 % of body weight and less than 30 % of body surface as a rule reduces complications.
Cardiac diseases are associated with serious complications leading to perioperative mortality. One should be particularly careful in assessment of asymptomatic patients with risk factors such as obesity, diabetes, hypertension, hyperlipidemia, cigarette use, or serious cardiac diseases in the family. While planning anesthesia for patients with significant cardiac diseases, it is preferable to perform the surgical procedure under hospital conditions rather than office conditions. For any effective surgery to be performed after a myocardial infarction (MI), the surgery must be planned for at least 6 months later [19]. Hemodynamic stability must be ensured in order to prevent perioperative ischemic attacks.
Obesity is associated with risk factors such as hypertension, coronary arterial disease, hyperlipidemia, diabetes, obstructive sleep apnea (OSA), and degenerative disc disease. Perioperative pulmonary emboli risk is considerably high in morbid obesity. Obesity attended by any one of these risk factors increases the complication risk in anesthesia [20]. In the obesity assessment of the patient, body mass index (BMI kg/m2) and waist-hip ratio are used. If the waist circumference is longer than 102 cm for male patients and longer than 89 cm for female patients, they are accepted as high risk in terms of obesity-related diseases. Patients with BMI values over 30 are evaluated as obese, and patients with BMI values over 35 are evaluated as morbidly obese [21]. Hypertension is very common in these patients and must be under control during operation. If there are symptoms or findings pertaining to heart failure or coronary artery disease in morbidly obese patients, it is appropriate to apply advanced tests (such as echocardiography, dobutamine stress test, etc.) to evaluate myocardial damage. In patients having undergone bariatric surgery before abdominoplasty, an additional careful assessment must be performed in terms of nutrition and vitamin deficiencies [1].
Things to Remember: Box 2.8
BMI >30→obese
BMI >35→morbid obese
Attention for additional diseases
Things to Remember: Box 2.9
For male patients
If WC (waist circumference) >102 cm
For female patients
If WC >89 cm, then they are in high-risk category which means they might have an obesity-related disease.
Hypertension is accepted by many authors as a disease that must be stabilized before an operation. Perioperative cardiovascular complications such as ischemia can be addressed, and thus morbidity and mortality can be reduced [22]. In patients undergoing hypertension treatment, drugs must be used until the morning of the operation day due to rebound hypertension risk. An exception to this case is angiotensin-converting enzyme (ACE) inhibitors. Since this group of drugs may lead to hypotension during anesthesia induction, they must be ceased before operation [23].
Diabetes Mellitus is a case increasing surgical mortality particularly when it is not regulated. It can increase the tendency toward many end-organ diseases such as cardiovascular, renal, or different wound healing [24]. Keeping in mind that silent myocardial ischemia incidence is high in diabetic patients, necessary care must be provided in preoperative assessment [25]. In type 1 or type 2 diabetic patients, the purpose is firstly to prevent hypoglycemia in perioperative treatment. For this purpose, blood sugar follow-ups must be performed carefully beginning from the morning of the operation day until the patient is discharged, and interventions must be performed with appropriate procedures when necessary.
Pulmonary diseases cover conditions that can affect pulmonary functions during operation and are widely encountered. The most frequent conditions include upper respiratory tract infections, chronic bronchitis, chronic obstructive pulmonary disease, bronchial asthma, and a cigarette habit. In cases of upper respiratory tract diseases, operations must be postponed until symptoms such as coughing, fever, expectorating, and shaking fully dissipate, particularly in patients for whom general anesthesia is considered. In a prospective study, it was demonstrated that postoperative pulmonary complication risk increases by approximately sixfold in smoking patients. It was detected that reducing smoking within 1 month before the surgery is not associated with any decrease in postoperative pulmonary complication risk [26]. Management of asthma patients with success can be achieved by determining whether they are in attack or not via a careful anamnesis and physical examination and by an appropriate intervention. If the asthma is under control, it does not constitute any additional risk in terms of perioperative complications. In contrast, in cases of inadequately controlled asthma, perioperative complication risk is almost always present [27]. Therefore, treatment of asthma patients must be continued until the surgery, and patients must be educated regarding postoperative airway exercises.
Things to Remember: Box 2.10
If a patient had a myocardial infarction, any elective surgery must be planned for at least 6 months after that.
Things to Remember: Box 2.11
Hypertension, diabetes, and asthma must be regulated preoperatively.
Treatments must be continued until surgical day (except for ACE inhibitors).
Obstructive Sleep Apnea (OSA) can be defined as a sleep disorder where respiration stops for five times or more within an hour of sleep, during more than 10 s despite respiratory efforts, and characterized by 4 % or more decrease in arterial saturation [28]. Many drugs from sedative, hypnotic, or narcotic-analgesic group which are used during anesthesia increase airway obstruction risk and lead to respiratory depression particularly in patients with OSA. In patients with severe OSA whose apnea-hypopnea index is higher than 30 in an hour, the desaturation possibility of the patient during anesthesia induction is evaluated as very high [29]. Patients with OSA generally use home-type CPAP (continuous positive airway pressure) masks to reduce symptoms. If the CPAP required for the patient is more than 10 cm H2O, ventilation with mask can much possibly be difficult [30].
2.4 Anesthesia Methods in Abdominoplasty
Anesthetic approaches can be reviewed under two categories as general anesthesia and regional anesthesia. Apart from these, sedative and nonsedative local anesthesia can also be applied in minor invasive surgeries over small areas.
2.4.1 General Anesthesia
General anesthesia is a particularly appropriate choice for those patients whose narcotic and sedative drug toleration is high, who suffer from extreme anxiety, and who will undergo major surgeries. The purpose of general anesthesia is to achieve a soft induction, to provide a complete and smooth wake-up, and to minimize side effects such as nausea, vomiting, and throat pain. Isoflurane, sevoflurane, and desflurane are the newest inhalation anesthetic agents. They have rapidly become popular since they are safe, protective, and easy to use.
Since the airway reflexes are blocked in general anesthesia, airway control is the most critical issue to which attention must be paid. The purpose of airway management is to maintain an open airway, to provide adequate ventilation, and to prevent aspiration of the stomach content. In obese patients, total pulmonary capacity, expiratory reserve volume (ERV), and functional residual capacity (FRC) decrease depending on the BMI increase. Thus, tendency toward arterial hypoxemia has increased due to ventilation-perfusion inconsistency and right-left shunt [31]. This is clearer in the supine position, and one must be careful since hypoxemia and desaturation may develop rapidly in anesthesia induction.
Things to Remember: Box 2.12
Obese patient ventilation is difficult under general anesthesia, and desaturation develops rapidly.
Attention for aspiration of stomach content.
2.4.2 Regional Anesthesia
Regional anesthesia may be applied in different ways: complete regional anesthesia without any additional anesthesia, regional anesthesia applied together with a mild sedation, and regional interventions applied to achieve postoperative pain control in procedures performed under general anesthesia.
In patients who will undergo abdominal wall surgery, dermatome area from T4 to L1 must be blocked. This region can be anesthetized through epidural or spinal anesthesia. While this method may provide the required anesthesia in the surgical area on its own, it can also be used together with general anesthesia or sedation. Surgical anesthesia is achieved within 5–15 min with spinal anesthesia. Applying the local anesthetic agent directly to cerebrospinal fluid (CSF) ensures rapid start for effect. There is certain recently reported information regarding abdominoplasty surgery performed by using spinal anesthesia under office conditions [32]. Spinal anesthesia can be performed through single-entry technique, or an intrathecal catheter can be placed when the surgery is estimated to last a long time.
In epidural anesthesia, a catheter is placed in the epidural cavity before the dura. The local anesthetic applied from the catheter is diffused from the dura and affects nerve roots. This is an ideal method for both intraoperative anesthesia and continuance of postoperative surgical area analgesia. During the last decade, the use of the combined epidural-spinal technique has been gradually increasing [33]. While surgical anesthesia is rapidly obtained with this method, the availability to intervene to extend the block allows us to adjust the regional block depth. There are certain limitations for patients undergoing spinal, epidural, or combined spinal-epidural anesthesia for abdominoplasty operation. While an effective intraoperative anesthesia is achieved through caudal spreading of local anesthetic, the sensory-motor block formed in lower extremities prevents early mobilization and increases urinary retention. Local anesthetic spreading toward the cranium may lead to paralysis in accessory respiratory muscles including the diaphragm and pressure in respiration. Local anesthetic spreading upward may block spinal cardiac accelerator fibers and thus decrease cardiac output and result in hypotension. Besides, since there is a mobilization restriction in patients undergoing abdominal wall surgery, anticoagulant treatment need must be kept in mind as a protective measure against thromboembolism [1–33]. As a result, regional anesthesia may not be appropriate for every patient undergoing abdominal wall surgery.
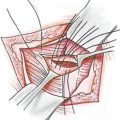
2.4.3 Planar Blocks: Transverse Abdominis Plane (TAP) Block
TAP block is a regional anesthesia technique providing analgesia on the frontal abdominal wall up to the parietal peritoneum including the muscles and skin. Compared to modern techniques it is not used much in practice, despite its high-success rate and relatively low-complication risk [34]. Subumbilical anesthesia of the abdominal frontal wall is achieved by applying local anesthetic in a high volume (20 ml) with a special needle together with ultrasound between the internal oblique muscle on lumbar Petit triangle and transverse abdominis muscle. When the oblique subcostal TAP block is added, the whole abdominal frontal wall is anesthetized [1–34].
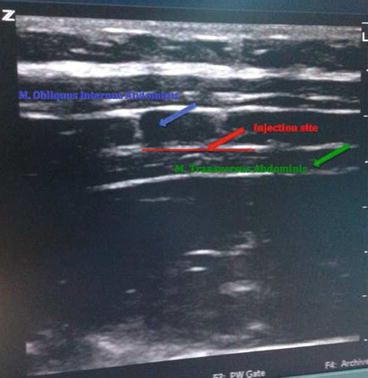
Postoperative pain treatment is worrisome for both surgeons and patients. In order to achieve a painless postoperative period, many methods such as local anesthetic infiltrations, epidural analgesia, peripheral nerve disorders, and intravenous patient-controlled analgesia (iv-PCA) are used. TAP block takes its place as a safe and effective method that can be applied easily under ultrasound guidance to reduce postoperative pain in lower abdominal region [35]. It is more important for patients with high risks such as obstructive sleep apnea since it reduces the need for postoperative narcotic drugs [35, 36]. In the labeled pictures below, some examples of ultrasound-guided TAP block are shown (Pictures 2.1, 2.2, and 2.3).


Picture 2.1
Ultrasound-guided TAP block (From the right lumbar Petit triangle)
Picture 2.2
Ultrasound-guided TAP block (From the left lumbar Petit triangle)
Picture 2.3
Ultrasound vision at TAP block
Things to Remember: Box 2.13
TAP block is very effective in postoperative analgesia.
It reduces narcotic needs and provides advantages to OSA patients.
2.4.4 Local Anesthesia
There are many local anesthetics used for infiltrative anesthesia. Safeness and effectiveness of the local anesthetic is the most important point for cosmetic plastic surgeons. The use of local anesthetic not only provides adequate anesthesia after an operation and during procedures applied but also minimizes blood loss and supports postoperative analgesia [37].
The basic pharmacologic effects of all local anesthetics are realized over sodium channels. Sodium entrance into neuron is blocked, and thus axon depolarization is ceased, and the local anesthetic effect begins. In addition to local anesthetic effect, it restricts inflammatory response by reducing the release of inflammatory cytokines from neutrophils, neutrophil adhesion to endothelium, free oxygen radical formation, and edema [38].
Local anesthetics are divided into the two main groups of ester and amid depending on their chemical structures and their characteristics that are demonstrated in Fig. 2.1. Information on the effective time and dose range of the amide group local anesthetics, used widely in infiltration anesthesia, is summarized in Table 2.3.
Fig. 2.1
Classification of local anesthetics
Table 2.3
Characteristics of certain local anesthetics used frequently in infiltration anesthesia
Without epinephrine | With epinephrine | ||||||||
|---|---|---|---|---|---|---|---|---|---|
Agent | Concentration (%) | Duration of action (min) | mg/kg total | Total ml | Maximum dose | Duration of action (min) | mg/kg total | Total ml | Maximum dose |
Lidocaine | 1 | 30–60
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

| |||||||