Class V: The presence of substantial visceral fat accumulation prevents any successful result even if extensive muscular tightening would be performed. Such patients are contraindicated for any abdominal surgery may it be liposuction or abdominoplasty and are directed to dieticians or bariatric surgery centers (Table 4.2).
Table 4.2
Classification of abdominoplasty candidates
Class
Visceral fat
Skin elasticity
Musculofascial tonus
Treatment
Class I
−+
Good
Good
Liposuction
Class II
−+
Good
Moderate
Endoscopic abdominoplasty
Class III
−+
Average
Moderate
Mini abdominoplasty
Class IV
−+
Poor
a
Inverse abdominoplasty
Class V
++
a
a
No surgery
Class I: On the contrary to visceral fat accumulation, subcutaneous fat accumulation can be solved with liposuction only if the skin elasticity is good without any stretch marks/striae and good abdominal wall integrity.
Class II: If skin quality is good but existing wall laxity is prominent, an endoscopic abdominoplasty together with or without liposuction or mini abdominoplasty might be chosen.
Class III: Medium level skin laxity, particularly with short upper abdomen, and the resulting lack of enough postsurgical skin cover may necessitate a combination of mini abdominoplasty with or without floating umbilicus and upper abdominal plication. It is to be noted that performing mini abdominoplasty without abdominal plication is a sure way to patient dissatisfaction. This is valid particularly for an incomplete plication covering only the lower part of the abdomen. In such cases, the tightening of the lower abdomen will result in bulging of the upper abdomen.
Class IV: If both wall integrity and skin elasticity are poor, a full inverse abdominoplasty should be considered.
As a summary, the typical patient for standard abdominoplasty has excessive, loose, sagging, abdominal skin, lax abdominal fascial wall, and/or diastasis recti with minimum visceral fat accumulation [9].
Things to Remember:
Three parameters: the visceral fat accumulation, the skin quality, and the abdominal wall laxity help us to decide about the necessary procedure.
The presence of substantial visceral fat accumulation prevents any successful result even if extensive muscular tightening would be performed.
Moderate visceral fat accumulation cannot be treated without abdominal wall plication.
Subcutaneous fat accumulation with a good skin quality and elasticity can be solved only with liposuction.
Medium level skin laxity, particularly with short upper abdomen, may necessitate a combination of mini abdominoplasty and upper abdominal plication.
Performing mini abdominoplasty without abdominal plication or with incomplete plication for the lower abdomen will result in even worse outcomes with rebound bulging of the upper belly.
4.3 Anatomy of a Beautiful Belly
Even a cursory perusal of the imagery depicting the ideal stomach in the popular culture – advertising, films, television, non-medical literature and so on – is required to appreciate that there is a dominant perception of what the abdomen, especially the female abdomen, should look like: flat and tight without overly obvious fat deposits. Women frequently desire to have an “hourglass” or “coke bottle” shape formed by the relative thinness of waist and abdomen relative to the fuller bustline and hips. Men often search for a “V-shape” with a waist area smaller than the shoulders and without full hips, and ones aspiring to an implied athleticism may seek a “six pack,” in which the individual muscles of the frontal abdomen stand out in relief.
Although this last effect is perhaps best achieved through long exercise, medical science does have its methods. Aside from our brief nod to common beauty standards, medical and scholarly literature and experience confirm that most people seeking the help of medical professionals for problems related to self-image in this area of the body much prefer to conform to these exact same cultural beauty norms; abdominal aesthetic intervention usually tries to replicate this archetypal shape in order to be considered successful. So the question for doctors is: How are these precise curves sculpted?
Abdominoplasty, liposuction, and other related procedures have been extensively researched and highly effective techniques have been developed. A surgeon looking to perform these operations has an abundance of resources to turn to for aid. However, one fact that can never change is that successful abdominal aesthetic intervention requires a detailed, three-dimensional familiarity with the anatomy of the body’s midsection.
There are distinct abdominal surface landmarks, dependent upon subdermal features, which define the shape of an attractive abdomen. Much of abdominoplasty involves resituating these visible lines and masses relative to one another.
The abdomen (less formally called the belly, stomach, tummy) constitutes the part of the body between the thorax (chest) and pelvis. Midway across horizontally, a slight furrow extends from the ensiform cartilage (also known as the xiphoid process) above to the pubic symphysis, constituting the linea alba in the abdominal wall. It is so called because it is made mostly of connective tissue (linea alba being Latin for “white line”). Since it is made up mostly of collagen and contains no primary blood vessels or nerves, it is a favored path for incisions. At about its vertical midpoint lies the bellybutton, better known as the umbilicus or navel.
On either side of the “white line,” broad recti muscles (sometimes, and not unambiguously correctly, known simply as the abs) stand out in muscular people. The outline of these muscles is interrupted by three or more transverse depressions indicating the linea transversae, or sometimes the tendinous intersections. These allow us forward flexion, as when we bend over to pick something up or do sit-up exercises. There is usually one near the ensiform cartilage, one at the umbilicus, and one between. Occasionally, in people with very low body fat, a fourth is visible below the umbilicus. It is the combination of the linea alba and the linea transversae which form the abdominal “six-pack” sought after by many fitness junkies and male models.
The linea semilunaris (also semilunar line or Spigelian line) is a curved tendinous line found on either side of the rectus abdominis muscle. Each corresponds with the lateral border of the rectus abdominis, extends from the cartilage of the ninth rib to the pubic tubercle.
The upper lateral limit of the abdomen is the costal margin (at or near the subcostal plane) formed by the cartilages of the false ribs [8–10] joining one another. The lower lateral limit is the anterior crest of the ilium, which runs from the anterior superior spine of the ilium to the spine of the pubis. These lower limits are marked by visible grooves [10]. These lines are demarking the grooves and eminences of the abdominal area. The hourglass appearance is the result of the concavity of the core muscles, the external oblique, the internal oblique, and the transverse abdominis between the thorax and the hips.
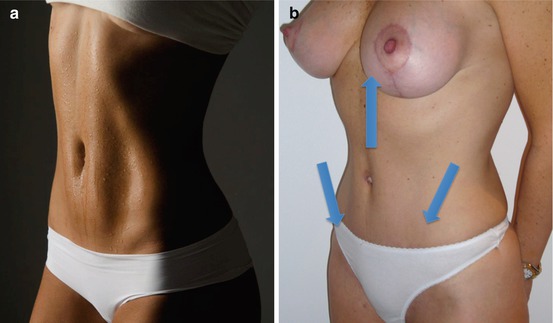
Ideally, there is a median tissue prominence marking the rectus muscles between the costal margin and the pubis, which is vertically divided by linea alba. This prominence has two grooves on both sides, which are delineated by the linea semilunaris (Fig. 4.1a).
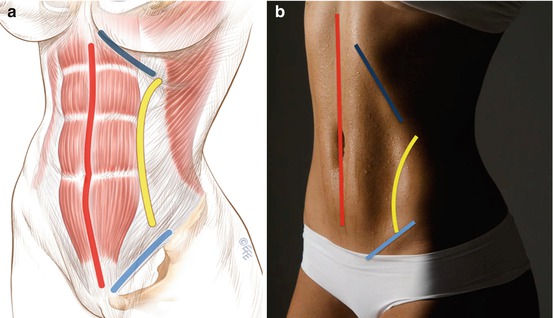
Fig. 4.1
(a, b) (left) Anatomy of the human abdomen and a modern example of a human female abdomen with superficial landmarks: linea alba, linea semilunaris, Poupart’s ligament, costal margin
4.4 Manipulating the Forces Effecting the Abdominal Shape
In order to mimic this ideal anatomy and to create a beautiful abdominoplasty result, we should fulfill the following basic aesthetic goals:
Get Clinical Tree app for offline access

- 1.
Coke bottle shape with bilateral grooves: We have to re-create the coke bottle shape by enforcing the concavity of the core muscles of the abdomen. The bilateral hollowing, following the linea semilunaris, which corresponds to the lateral border of the rectus abdominis, extending from the cartilage of the ninth rib to the pubic tubercle, is to be shaped (Fig. 4.2).