Fig. 7.1
(Slide 2 in PPT) – before and after “sit-down position” after combined procedure – abdominoplasty, liposuction of the back and flanks, implant exchange, and capsulotomies. Arrows from top to bottom, outline the supraumbilical midline sulcus, a small “mysterious” umbilicus, the length of the lower abdominal scar are determined by the location and length of the most lateral skinfold, infraumbilical short vertical scar from previous umbilical location is strategically placed below the top bikini line

Fig. 7.2
(Slide 3 in PPT) – before and after combined procedure – abdominoplasty with repair of large rectus diastasis, liposuction of the back and flanks, and breast augmentation. Arrows from top to bottom outline, improvement of rectus lateral margin after diastasis repair; well-healed scar with excellent placement below the bikini line
Ousterhout demonstrated the feasibility of combining abdominoplasty and high-volume suction lipectomy in the obese patient [27], and Dillerud showed that neither obesity nor liposuction increased flap necrosis in abdominoplasty [28]. It is widely held, however, that obesity is an independent risk factor for local wound healing complications and systemic morbidity [29–31].
7.4.1 Surgical Planning
Among our abdominoplasty patients, the most frequent request is for suction-assisted lipectomy (SAL) of adjacent areas including flanks, back, hips, and thighs.
In our practices, respectively, we routinely adjoin liposuction of the back and flank areas to our abdominoplasties. Starting in the prone position, the back and flank adiposities are addressed first prior to undertaking the anterior trunk. Circumferential reduction of excess adiposity produces a total torso transformation and improves the visual aesthetic from every angle. Liposuction of the back and flanks further assists in creating a defined waist where traditional abdominoplasty can blunt the waistline. Residual adiposity in the flanks and back can distract from an overall harmonious result from an abdominoplasty; when one area becomes smaller and tighter, it can call attention to other problem areas that were previously less noticeable.
Marking is done preoperatively while patient is standing. In all patients, we prefer abdominoplasty scar placed below the top bikini line. If umbilical scar cannot be removed completely, a short vertical scar is preferred instead of placing horizontal abdominoplasty scar in a higher level.
Things to Remember
We prefer abdominoplasty scar placed below the top bikini line. If umbilical scar cannot be removed completely, a short vertical scar is preferred instead of placing horizontal abdominoplasty scar in a higher level.
7.4.2 Anesthesia
General anesthesia should always be used in body contouring procedures. Excellent control of the airway is critical since the patient is moved and turned many times during the procedure. Initially, patient is transferred from the stretcher to the surgical table by turning from supine to prone position to achieve the liposuction of the back area and later back to a supine position to continue with the abdominoplasty procedure. Compression boots (SCD’s) are in place prior to induction, continued in the recovery room, and during the overnight stay. All patients are kept warmed with the use of a warm blanket and warm fluids. Hypothermia, a common problem in prolonged body contouring procedures with significant body exposure, can be completely avoided/prevented if appropriate preventative measures are taken at all times.
7.4.3 Patient Positioning
Once the patient is intubated and the endotracheal tube is secured, the patient is carefully placed in a prone position with padding under the arms, breast, and hips. The table is flexed and reversed Trendelenburg position is applied to avoid head down for prolonged periods and significant facial swelling. At this point, the tumescent solution is injected through one or two small incisions on the back. The superior midline incision is placed at the level of the brassiere, and the inferior midline incision at the top portion of the infra-gluteal fold. This process is followed by prepping and draping of the surgical area. After adequate time to allow the tumescent solution to work, the liposuction is completed in all of the pre-marked areas, using the power-assisted liposuction system. If fat injection is anticipated, fat collection is done during this part of the procedure (Fig. 7.3).

Fig. 7.3
(Slide 3 in PPT) – initial patient prone position ready for tumescent infiltration – surgical table flexed with padded hips, breasts, knees, and arms. Heating blanket is used below knees and above upper back immediately after patient is prepped
7.4.4 Patient Turning
Patient turning is a critical part of modern abdominoplasty surgery. It is done by a well-trained team in a safe and quick manner by protecting the airway, intravenous lines, and all patient extremities. We use a draw sheet and four team members to perform this part of the procedure. An effective and safe turning should be done in less than 15 s by protecting the patient, the airway, intravenous lines, and all other important accessories of the operation.
7.4.5 Surgical Technique
Once turning is completed, the abdominal markings are double-checked and only then injected with vasoconstriction solution. Patient is re-prepped and redraped. Team members scrub again and change gowns/gloves. Prior to making the first cut, symmetry is verified.
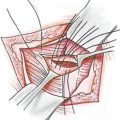
Anatomical details of importance in modern and safe abdominoplasty as emphasized by Saldanha [23, 24] include preservation of the Scarpa’s fascia in the abdominal flap for increased blood supply to the dermis and skin. Also, by performing a selective tunnel undermining (instead of total undermining) over the rectus diastasis only preserving the lateral rectus muscle perforators, 80 % of the blood supply to the abdominal wall is protected. Thus, reducing complications when compared to traditional abdominoplasty and also combined bariatric surgery.
After liposuction is completed, abdominoplasty is carried out. Adding liposuction to abdominoplasty flap (lipoabdominoplasty) when necessary increases the pliability of the abdominoplasty flap and makes postoperative result better. Liposuction of the abdominal flap first also makes the elevation of the abdominal flap easier. Additionally, vasoconstrictor agents in liposuction solution spare the perforator vessels. The main concern with concurrent liposuction of the abdomen with abdominoplasty is ischemia and necrosis of the flap. The area most at risk for this complication is a triangular area beginning at the umbilicus and extending to the suprapubic region. When the perforator vessels are spared, we did not expect such a complication. And we did not observe such a complication in our cases, either.
During the dissection, a narrow undermining of the midline by preserving the lateral rectus muscle perforators is critical as described in the inverse abdominoplasty technique section. The supraumbilical tunnel is undermined all the way up to the xiphoid process, preserving the lateral neurovascular bundles that support the abdominal flap. Once the entire supraumbilical flap and the inferior flap are free, the pull-down approach is used to estimate where the inferior flap or the lower resection can be made end bloc and without much tension, and the rectus fascia plication is performed.
Things to Remember
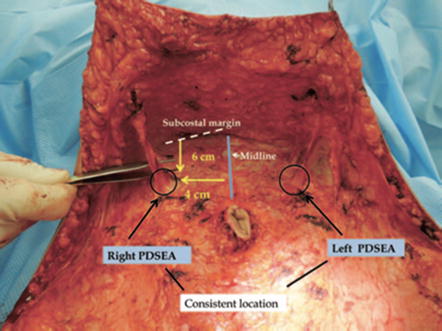
The perforator vessels are located consistently in a 2-cm radius located 4 cm from the midline and 6 cm from the subcostal margin [33].
Lipoabdominoplasty (described in 2001): Liposuction of the abdomen combined to rectus muscle plication through selective and safe undermining of the abdominal flap in the supraumbilical area by preserving the lateral rectus muscle perforators, thus increasing blood supply to the abdominal flap and its survival, decreasing the incidence of seroma and other complications of traditional abdominoplasty.
7.4.6 Pain Control, Drains
Before closing the lower abdominal wound, drains are placed, and injections of Exparel® (bupivacaine liposome injectable suspension) to the fascia are done. The drains are extended to the lower back and brought out through the suprapubic area. They drain the liposuctioned areas and lower abdomen, therefore decreasing the amount of swelling and bruising in the lower back. During the early postoperative period, we recommend the drains to be on low suction during recovery room and overnight admission.
If one elects to use Exparel®, the injections should follow manufacturers’ recommendations and cover the rectus aponeurosis, external oblique aponeurosis (if the extended technique was used), and around the incision sites. Since senior author (RS) has been using Exparel® exclusively in all abdominoplasty cases and observed that patients have absolutely no abdominal pain and only some discomfort easily treatable with nonsteroidal anti-inflammatory drugs like ibuprofen, he has completely stopped the pain pumps usage.
Things to Remember
Postoperative pain control allows early ambulation, thereby decreases the theoretical potential of thrombophilia.
7.4.7 Optimizing Outcomes
Promoting safe surgical practice and prevention of catastrophic events are the surest ways to optimize outcomes. Prior to the operating room, there should be a vigilant investigation of both personal and family history of thrombotic events. Our guidelines in clinical practice are as follows (Table 7.1):
Table 7.1
Our guidelines in clinical practice of combined abdominoplasty procedures (abdominoplasty + liposuction, abdominoplasty + aesthetic breast surgery, etc.)
Hematologic and/or appropriate specialist consultation for patient or family history of coagulopathy including miscarriages, early myocardial infarction, prior thromboembolic events |
Cancelation of immediate preoperative trips via airplane or car |
A baseline preoperative duplex scan with even a minor clinical suspicion |
Oral contraceptives and hormones stopped at least a month prior to surgery |
Sequential compression devices prior to induction of anesthesia, in recovery room, and during overnight stay |
Adequate temperature management to avoid hypothermia |
Low-molecular-weight heparins (Lovenox) starting at 8–10 h after completion of surgical procedure and to continue 3–5 days until fully ambulatory |
Aggressive early ambulation by recovery room and overnight stay nurse personnel |
Patient and family to be educated about the importance of ambulation in the immediate postoperative period so it continues at home after discharge from the surgical facility |
An outstanding postoperative appearance does not guarantee that an outcome is satisfactory to the parties involved. A postoperative period that is free of major clinical complications and delayed healing can significantly enhance both patient and surgeon satisfaction.
7.4.8 Postoperative Care
All patients should be placed in a semi-compressive dressing after abdominoplasty and other ancillary procedures. Initial dressing with foam dressing such as Reston over liposuctioned areas and abdominal binders is appropriate. In our practice, patients are instructed to purchase compressive garments that encompass the abdomen and hips and wear the garments continuously for 6 weeks after surgery. Both medical grade and commercially available compressive garments are appropriate as long as they are worn with consistency. Surgical edema often persists for several months, and inconsistent use of garments can exacerbate the unflattering appearance.
Scar massage, lymphatic massage, and topical therapies such as silicone sheets are frequently used among our patients with the understanding that the therapeutic outcomes are highly variable. Frequent and regular postoperative visits are essential in impeding wound problems before they flare out of proportion.
Postsurgery weight control is regularly discussed with our patients so that the surgical results are maintained. This is especially crucial in the postoperative period when the patient may be more sedentary than usual, and activity restrictions prevent them from strenuous exercise.
Patients are kept in the surgery center overnight for safe postoperative management (pain control, fluid management, and deep vein thrombosis (DVT)/pulmonary embolism (PE) prevention) when abdominoplasty is combined with other body contouring procedures or patient’s health conditions warrant closer observation and care. The compression girdle is recommended for the first 4–6 weeks. Patients are then allowed to resume regular exercises. Their weight is checked and documented in the chart during all office visits.
7.4.9 Complications
In the past, abdominoplasty has been implicated in higher incidence of complications when performed in a combined procedure. In the 2001, ASAPS Lipoplasty Survey performed between 1998 and 2000; data from 159 procedures was collected [32]. ASAPS members reported on 94,159 lipoplasty procedures. In all, 66 % of the procedures were suction-assisted lipectomy (SAL = lipoplasty = liposuction) alone, 20 % were lipoplasty without abdominoplasty but with one or more additional procedures, and 14 % of the SAL was combined with abdominoplasty. At result, they reported that the addition of abdominoplasty to suction-assisted lipectomy increased the likelihood of postoperative complications by a factor of 14. After this study was carried out, lipoabdominoplasty concept has become popular which was based on the preservation of the perforator vessels, and thereby increasing the safety of the lipoabdominoplasty procedure and decreasing the complications accordingly [23, 24, 33]. Additionally, with implementation of safe clinical practices such as preoperative screening, effective pain control, early ambulation, and multiple methods of anticoagulation; complications including thromboembolic events observed after liposuction-abdominoplasty combination decreased at the last decades.
The development of deep vein thrombosis and pulmonary embolism poses a small but significant risk for surgical patients and may result in death or debilitating consequences. The risk of deep venous thrombosis (DVT) and pulmonary embolism (PE) in liposuction-abdominoplasty combination is likely multifactorial: prolonged operative time, increased pelvic vein compression due to rectus muscle diastasis repair which theoretically increases intra-abdominal pressure, and prolonged recovery period with relative immobility.
Muscle plication and abdominal binders that can compress the abdominal cavity may also interfere with respiratory mechanics. Changes in pulmonary compliance can occur after abdominal plication and may be predictive of respiratory complications. Rectus plication causing intraabdominal hypertension decreases venous return, results in venous stasis, and thus increased deep venous thrombosis risk occurs. A study conducted on 12 abdominoplasty patients confirmed the effect of rectus plication on increasing intraabdominal pressure but also implicated bed position, binder placement, and general anesthetic as risk factors [34]. Combination with the liposuction can worsen the vicious circle by increasing the immobility and edema. On the other hand, in other studies minimal changes in intraabdominal pressures and minimal to negligible changes in intrathoracic pressures were reported after abdominoplasty with muscle plication. It is important to note that pulmonary function assessed with pulmonary function tests and peak airway pressures may be insufficient measures of acute respiratory changes that could lead to postoperative pulmonary morbidity. Additionally, strength of plication is also important.
Over a 2-year period, 175 patients underwent lipoabdominoplasties in the senior author’s (RS) practice. One hundred forty-one patients (80 %) underwent combination procedures (Table 7.2).
Table 7.2
Combined surgeries of 175 lipoabdominoplasty patients
Combined surgeries of lipoabdominoplasty patients | 175 patients |
|---|---|
Only lipoabdominoplasty | 34 (20 %) |
Combined with SAL back/extremities | 79 (46 %) |
Combined with breast surgery | 31 (17 %) |
Combined with other surgeries | 31 (17 %) |
The complications of combined procedures were comparable to rates after lipoabdominoplasty alone and superior to rates associated with traditional abdominoplasty in the author’s practice. Three patients required hospitalization after a combined procedure: two admissions were for postsurgical complications and one patient for inadvertent narcotic overdose while at home. There was a single incidence of pulmonary embolism that recovered well with intravenous heparin therapy and hospitalization. This particular patient received both mechanical and chemical prophylaxes. It was discovered afterwards that the patient had driven 10 h the day prior to surgery (Table 7.3).
Table 7.3
Complications among 175 patients who underwent lipoabdominoplasty alone or in combination
Complications among 175 patients who underwent lipoabdominoplasty alone or in combination | |
|---|---|
Seroma | 5 (2.85 %) |
Pulmonary embolism | 1 (0.5 %) |
Dehiscence | 1 (0.5 %) |
Narcotic overdose | 1 (0.5 %) |
The Authors’ Comment
By better preserving the nerves and vasculature to the anterior abdominal wall, modern abdominoplasty likely reduces much of the most common and aggravating complications of traditional abdominoplasty, including seromas and lower skin flap necrosis. When perforator vessels are spared, abdominoplasty can be safely combined with liposuction (liposuction of abdominal flap) with no increase in complication rates. This procedure can potentially be safely combined with other aesthetic procedures to produce a more dramatic transformation.
7.5 Abdominoplasty Combined with Aesthetic Breast Surgery
Among abdominoplasty patients, the second most frequent request is for aesthetic breast surgery. In this section, we address the issues surgeons facing in abdominoplasty – aesthetic breast surgery combination and the findings in the literature and our experience (RS and DO).
Among the weight loss and multiparous patients, the ptotic, involuted breasts can similarly detract from achieving a harmonious result. The huge popularity of the so-called mommy makeovers stems from the high incidence of simultaneous deformities of the breasts and the abdomen. Augmentation, mastopexy, and augmentation-mastopexy are the most common cosmetic breast operations combined with abdominoplasty to rejuvenate and restore felicitous dimensions to the breasts. When combined with lipoabdominoplasty and suction-assisted lipectomy of the lower torso, breast aesthetic surgery can facilitate a more complete transformation (Figs. 7.4 and 7.5) (Table 7.4).