Box and U-Shaped Osteotomies
Sunil Tholpady
Robert J. Havlik
Barry L. Eppley
DEFINITION
Orbital dystopia is used to describe a vertical or horizontal displacement of the entire orbit and its contents.
The most common dystopia encountered is orbital hypertelorism.
ANATOMY
Hypertelorism is an abnormal interorbital distance and should not be confused with telecanthus, which is lateral displacement of the medial canthi without normal bony architecture (FIG 1).
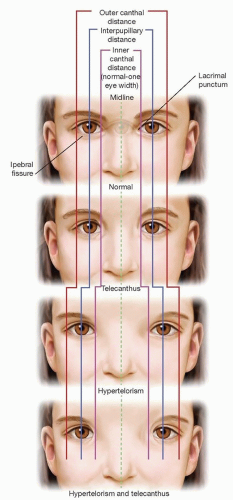
FIG 1 • Differences between telecanthus and hypertelorism.
Ethmoid sinuses are often overexpanded with excess medial soft and hard tissue.
Severe hypertelorism can be associated with inferior displacement of the cribriform plate.
The interorbital distance (dacryon to dacryon) is used to diagnose and classify hypertelorism. (The intercanthal distance is 4 to 6 mm greater than the interorbital distance due to soft tissue.)
Normal is 25 mm in women and 28 mm in men.
First degree: 30 to 34 mm
Second degree: 34 to 40 mm
Third degree: greater than 40 mm1
PATHOGENESIS
Orbital dystopias are a heterogeneous group of disorders that usually arise as a consequence of congenital or traumatic conditions:
Craniofrontonasal dysplasia
Apert or Crouzon syndrome
Encephaloceles or craniofacial clefts
Frontal sinus mucocele
Neurofibromatosis
Fibrous dysplasia
Craniofacial trauma
Orbital positioning will at best be maintained and may worsen with time and growth.
Traumatic dystopias can occur at any age.
PATIENT HISTORY AND PHYSICAL FINDINGS
Symmetric hypertelorism with wide set brows
Vertical malposition of the orbit
Epicanthal folds
Wide nasal dorsum
Amblyopia or strabismus
Inferolaterally positioned zygomas
High-arched palate
IMAGING
Neurosurgical consultation is appropriate for intracranial exposure.
Ophthalmologic consultation for amblyopia, strabismus, or extraocular dysfunction and postoperative visual changes
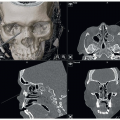
Three-dimensional computed tomographic reconstruction of the face and skull is necessary.
Three-dimensional printed models may be useful for visualizing and teaching surgery.
SURGICAL MANAGEMENT
Most surgical corrections of hypertelorism in the pediatric population are performed between the ages of 4 and 8.
Psychosocially, this is a period of development during early school years.
The cranium has had a period of explosive growth, and the interzygomatic distance is nearly adult-sized by age 6.
The sinuses have not yet pneumatized.
Most stable results are obtained in adults, and there may be a need for revision when the procedure is performed in the pediatric population.
There are no absolute contraindications, but patients with a high-arched palate, narrowed midface, inferolaterally displaced orbits, or very severe cases may benefit from a facial bipartition procedure to correct these concerns.
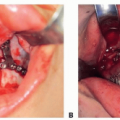
Box osteotomies can be used to correct both horizontal and vertical dystopias. An intracranial approach is preferable with significant (greater than 40 mm deformity), as this provides access to the central ethmoidosphenoidal area. Orbits are sectioned in a 360-degree fashion (FIG 2A).2
Preoperative Planning
Medical models of the skull abnormalities enable preoperative knowledge of osteotomy positions and predicted movements (FIG 3).
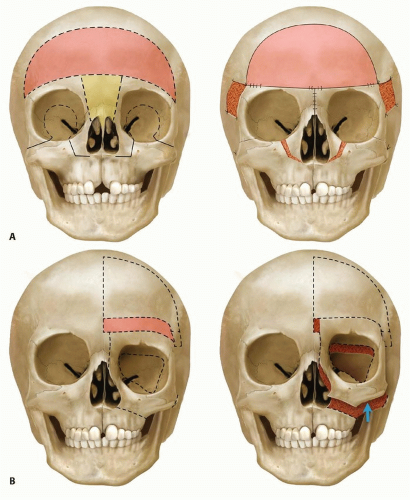 FIG 2 • Medical modeling with proposed osteotomies and final result. A. Demonstrates box osteotomies and (B) demonstrates U-shaped osteotomies.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|