Auricular Reconstruction for Microtia and Post-traumatic Deformities
Charles H. Thorne
DEFINITION
Microtia literally means small ear but is used to refer to a spectrum of auricular anomalies (FIG 1) that are almost always associated with aural atresia (absence of the external auditory canal).
From a practical point of view, any congenital deformity of the auricle that requires insertion of a complete or nearcomplete cartilage or synthetic framework is an example of microtia.
As discussed below, the principles for reconstruction of other auricular deformities such as post-traumatic deformities are similar.
ANATOMY
As depicted in FIG 1, the anomalies that constitute microtia vary from almost complete anotia to cases that demonstrate an almost normal lower 2/3 of the auricle. Microtia has been classified in various ways, but the most useful is the classification of Nagata: lobular microtia, small concha microtia, and large concha microtia. Complete anotia is almost never seen.
Patients with microtia almost always have absence of the external auditory canal (aural atresia) with complete bony separation of the auricular remnant and the middle ear structures (FIG 2).
The middle ear is underdeveloped and also presents variable abnormalities. If an apparent external auditory canal is present, it is almost always blind or stenotic. Patients with microtia, therefore, almost always have total conductive hearing loss on the affected side.
Microtia is more common on the right side; 90% of cases are unilateral, and those patients usually have normal hearing in the contralateral ear.
In the 10% with bilateral involvement of microtia and aural atresia, the patients are functionally deaf and require bone conductive hearing aids on an urgent basis in order to develop speech.
There are several anatomic differences between microtia and post-traumatic deformities:
The skin quality in post-traumatic cases may present problems because of scarring around the remnant.
Post-traumatic auricular remnants almost always contain a canal and a tragus, making reconstruction of near-normal auricle more likely.
Post-traumatic remnants may be distorted by scar but are almost always in the correct position, as opposed to microtic remnants that are often malpositioned.
PATHOGENESIS
The auricle and the middle ear develop together from the first and second branchial arches, explaining the concomitant anomalies of those two structures.
The inner ear is almost always normal in microtia patients because it arises separately in embryonic development and is not a branchial arch derivative.
Microtia is the second most common congenital deformity affecting the head and neck (after cleft lip and palate) and is more common in patients of Southeast Asian descent.
PATIENT HISTORY AND PHYSICAL FINDINGS
Microtia and aural atresia fall within the larger spectrum of craniofacial microsomia or first and second branchial arch syndrome. Craniofacial microsomia can present with either unilateral (ie, hemifacial microsomia) or bilateral involvement.

FIG 1 • Variable presentation of microtia. The term microtia refers to a wide variety of presentations. A. Small conchal-type microtia. B. Lobular-type microtia. C. Almost complete anotia. D. Atypical microtia with hemifacial microsomia.
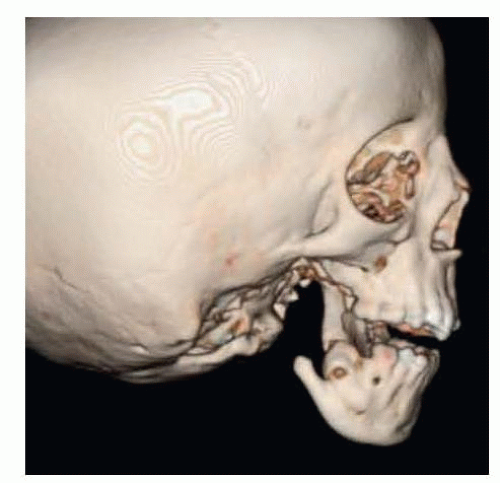
FIG 2 • Aural atresia. Microtia is almost always accompanied by aural atresia. Note the absence of an external auditory canal and, in this case, an extremely hypoplastic mandibular ramus.
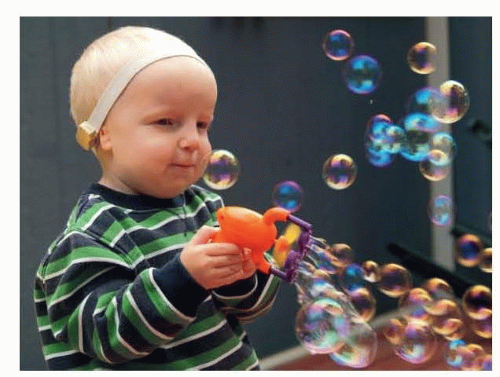
FIG 3 • BAHA soft band. Infants with unilateral microtia benefit from the BAHA soft band, which will provide binaural hearing. Patients with bilateral aural atresia must have a bone conduction aid in order to hear and to develop normal speech.
Most patients with microtia have symmetrical or nearly symmetrical faces, but radiographs usually show some asymmetry of the ipsilateral mandibular condyle indicating that microtia is part of the craniofacial microsomia spectrum.
A minority have more obvious underdevelopment of the tissues of the face including mandible, soft tissue, facial nerve, and auricle.
SURGICAL MANAGEMENT
The autogenous method of auricular reconstruction is the technique with which this author is most familiar.1,2,3 If the reader is interested in a technique using synthetic frameworks, the publications of John Reinisch are recommended.4
The ideal age to perform reconstruction of a missing auricle is age 10 years.
At this age, the contralateral ear has reached adult size, and the rib cartilages are large enough to create an adult size ear framework. In a patient who is small for his/her age, delaying surgery until the patient is approximately the size of an average 10-year-old is recommended.
Prior to age 10, the focus of patient management is on the hearing.
As mentioned, a patient with unilateral microtia has a total conductive hearing loss on the affected side but normal hearing in the unaffected ear. These patients can hear normally in quiet environments, but the lack of binaural input causes difficulty with localizing sound and in discriminating sounds in noisy environments. For example, a unilateral patient will have difficulty playing football when his/her name is yelled. The patient may have trouble immediately determining the direction of the sound and may look in the incorrect direction initially. In addition, in a room with multiple voices, it is more difficult for a microtia patient to screen out the background noise to focus on a conversation. These patients benefit from a bone conduction hearing aid (FIG 3).
Patients with bilateral microtia, on the other hand, absolutely require conduction aids because they are functionally deaf and will not develop normal speech without appropriate aids.
Hearing can be restored either surgically or by use of a bone-anchored hearing aid (BAHA).
Reconstruction of the external auditory canal and ossicles can be surgically performed in approximately half the cases of aural atresia. In the other 50% of cases, the anatomy is too deranged for surgical repair.
BAHAs are so effective, however, and less prone to complications when compared to canalplasty, that they are more commonly employed than surgical reconstruction of the canal (FIG 4).
Preoperative Planning
When planning the auricular reconstruction, a tracing of the contralateral ear is made (FIG 5) that can be sterilized for intraoperative use. From that tracing, the surgeon then makes a drawing of the framework that would be required to produce that size auricle.
Because the skin has a certain thickness (approximately 2 mm), the framework must be at least 4 mm shorter than the desired auricle (or shorter depending on how deep in the native lobule the framework will be placed).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








