Abstract
Atrophies of the skin are caused by a diminution or loss of collagen and/or elastic fibers. These disorders range from common conditions, such as striae distensiae, to those conditions associated with very rare syndromes (e.g. Conradi–Hünermann–Happle syndrome, Rombo syndrome). In addition, the areas of atrophy can range from quite large, as in mid-dermal elastolysis, to punctate, as in follicular atrophoderma. The involvement can also vary from subtle to obvious. In most disorders, the underlying pathogenesis remains to be discovered.
Keywords
anetoderma, atrophoderma, atrophoderma of Pasini and Pierini, idiopathic atrophoderma of Pasini and Pierini, mid-dermal elastolysis, piezogenic papules, piezogenic pedal papules, striae, follicular atrophoderma, atrophia maculosa varioliformis cutis, atrophoderma vermiculatum
Atrophies of the skin that are due to a diminution or loss of collagen and/or elastic fibers are discussed in this chapter. The areas of involvement can be quite large, as in mid-dermal elastolysis, or punctate, as in follicular atrophoderma. In most disorders, the underlying pathogenesis remains to be discovered.
Mid-Dermal Elastolysis
- ▪
Uncommon disorder with areas of fine wrinkling
- ▪
Usually affects Caucasian middle-aged women
- ▪
Selective loss of elastic tissue in the mid dermis
Introduction
Mid-dermal elastolysis is a rare acquired disorder of elastic tissue. Clinically, it is usually characterized by diffuse fine wrinkling, most often located on the trunk, neck, and arms. Histologically, a clear band of elastolysis is present in the mid dermis.
History
In 1977, Shelley and Wood reported the first case of “wrinkles due to idiopathic loss of mid-dermal elastic tissue”. Their patient, a 42-year-old woman, had circumscribed areas of fine wrinkles that gave her an inappropriately aged appearance .
Epidemiology
To date, ~100 cases have been reported in the literature. The vast majority of patients are Caucasian women between the ages of 30 and 50 years .
Pathogenesis
The cause of the acquired elastic tissue degeneration in mid-dermal elastolysis is still unclear. Exposure to UV light is thought to be a major contributing factor in the degeneration of elastic fibers (as in annular elastolytic giant cell granuloma). There are reports of mid-dermal elastolysis developing after significant UV exposure, including natural sunlight, UVA (tanning salon), and narrowband UVB phototherapy .
Other possible mechanisms include defects in the synthesis of elastic fibers, autoimmunity against elastic fibers, and damage to elastic fibers via the release of elastase by inflammatory cells or fibroblasts. Of note, it has been observed in the setting of immune reconstitution inflammatory syndrome (IRIS). An imbalance between matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs) may also be playing a role, in addition to CD34 + dendritic fibroblasts . Recently, a decrease in lysyl oxidase-like 2 (LOXL2) expression, potentially affecting elastin renewal, was observed in this condition .
Clinical features
In mid-dermal elastolysis, patients can have well-circumscribed to large diffuse areas of fine wrinkling ( Fig. 99.1 ), usually in a symmetric distribution (type I). The wrinkles themselves tend to follow cleavage lines. Discrete perifollicular papules are seen in some patients (type II), with the site of the central hair follicle being indented. Occasionally, erythematous patches, telangiectasias, and reticulated erythema may be present (type III) . Although in the majority of patients there is no history of a prior inflammatory dermatosis, some patients do report previous mild to moderate erythema and, rarely, the elastolysis is preceded by urticarial lesions or granuloma annulare.

Sites of predilection are the trunk, lateral neck, and upper extremities. Once the patches of wrinkling have appeared, they usually remain stationary. They are asymptomatic and give the skin a prematurely aged appearance. The affected areas usually have normal pigmentation and no associated scaling, induration, or herniation. There is neither associated systemic involvement nor a family history of similar lesions.
While diagnosis is usually confirmed via histologic examination of involved skin, non-invasive imaging techniques such as optical coherence microscopy or high-frequency ultrasound may also prove helpful .
Pathology
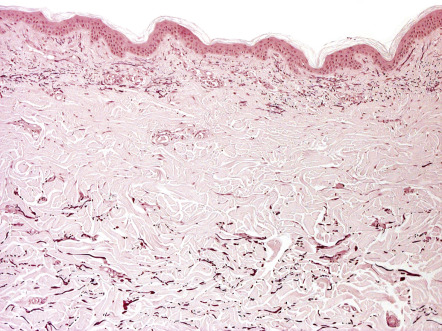
The epidermis is normal in appearance and, occasionally, a mild perivascular infiltrate is noted in the dermis. Elastic tissue stains, such as Verhoeff–van Gieson or Weigert’s stain, reveal a selective loss of elastic fibers in the mid dermis ( Fig. 99.2 ). There is preservation of normal elastic tissue in the superficial papillary dermis above, in the reticular dermis below, and along adjacent hair follicles. The preservation of elastic tissue around the hair follicles explains the perifollicular papules observed in some patients.
By electron microscopy, phagocytosis of normal as well as degenerated elastic fiber tissue by macrophages has been described . Elastophagocytosis by macrophages is also occasionally observed by routine histology.
Differential diagnosis
Mid-dermal elastolysis must be differentiated from the other disorders of elastic tissue such as anetoderma, pseudoxanthoma elasticum (PXE), PXE-like papillary dermal elastolysis, elastoderma and cutis laxa, especially the acquired form ( Table 99.1 ).
| DISORDERS OF ELASTIC TISSUE | |||
|---|---|---|---|
| Condition | Clinical findings | Site of predilection | Pathology |
| Anetoderma | Multiple circumscribed areas of flaccid skin; lesions are often elevated (protruding), but can be macular or depressed | Usually on trunk | Focal or complete loss of elastic tissue in the papillary and/or reticular dermis |
| Cutis laxa (see Ch. 97 ) | Loose, sagging skin folds resulting in prematurely aged appearance. Hereditary or acquired. Internal organ involvement, e.g. pulmonary, in hereditary form and generalized acquired form | Eyelids, cheeks, neck, shoulder girdle and abdomen; distal digits in acquired acral form | Diminished and fragmented elastic fibers usually throughout the dermis |
| Mid-dermal elastolysis | Diffuse areas of fine wrinkling (type I), perifollicular papules (type II), and/or reticulated erythema (type III) in middle-aged women | Trunk, arms, and lateral neck | Selective loss of elastic fibers within the mid dermis in a band-like pattern |
| Pseudoxanthoma elasticum (PXE; see Ch. 97 ) | Yellowish coalescing skin papules, “cobblestoning”, and redundant folds in flexural sites; associated ocular and cardiovascular involvement | Lateral neck, axillae, and groin; scars | Clumped and calcified elastic fibers in the mid dermis |
| PXE-like papillary dermal elastolysis | Multiple, 2–3 mm, yellow or skin-colored papules that can coalesce into cobblestoned plaques | Neck, flexor forearms, axillae, lower abdomen, inframammary folds | Decreased elastic tissue in the papillary dermis (band-like pattern); clumping and fragmentation of elastic fibers; no calcification of elastic fibers |
Clinically, anetoderma is characterized by soft macules and papules that herniate upon palpation, as opposed to diffuse wrinkling. Histologically, elastolysis can occur in the papillary and/or mid-reticular dermis in anetoderma (see below). Patients with generalized cutis laxa have loose, redundant skin, hanging in folds, and histologic examination shows elastolysis that frequently involves the entire dermis. Acquired cutis laxa, both generalized and acral, can be a manifestation of an underlying paraproteinemia, with binding of immunoglobulins to elastic fibers (see Table 97.7 ). In addition, there is a form of postinflammatory elastolysis and cutis laxa that was originally described in young girls of African descent; an inflammatory phase consisting of indurated plaques or urticaria, malaise and fever precedes the development of diffuse wrinkling, atrophy, and severe disfigurement. Insect bites may be the trigger for the initial inflammatory lesions .
Less often, mid-dermal elastolysis is confused with solar elastosis or the perifollicular elastolysis that is usually seen on the trunk in association with acne vulgaris. Solar elastosis differs clinically by its onset in an older age group, restriction to only sun-exposed areas, yellow color, and coarser wrinkling and differs histologically by hyperplasia of abnormal elastic fibers and basophilic degeneration of the collagen in the papillary dermis. Perifollicular elastolysis leads to a selective and almost complete loss of the elastic fibers that surround hair follicles, compared with preservation of elastic fibers around follicles in mid-dermal elastolysis.
Treatment
Currently, there is no effective treatment for mid-dermal elastolysis. Sunscreens, colchicine, chloroquine, vitamin E, and topical agents (retinoic acid, corticosteroids) have been tried without success .
Anetoderma
▪ Macular atrophy ▪ Anetoderma maculosa ▪ Anetoderma maculosa cutis ▪ Atrophia maculosa cutis
- ▪
Circumscribed 1–2 cm areas of flaccid skin, which may be elevated, macular, or depressed
- ▪
Primary anetoderma has classically been divided into inflammatory and non-inflammatory
- ▪
Secondary anetoderma is associated with infectious and inflammatory cutaneous disorders as well as tumors and autoimmune disorders (e.g. antiphospholipid antibody syndrome)
- ▪
Focal dermal defect of elastic tissue
Introduction
The term “anetoderma” is derived from anetos , the Greek word for slack, and derma for skin. Anetoderma is an elastolytic disorder characterized by localized areas of flaccid skin, which may be depressed, macular or papular; the latter can reflect herniation of the subcutaneous tissue. Anetoderma may be idiopathic or associated with an inflammatory disorder of the skin.
History
The first case of primary inflammatory anetoderma was reported by Jadassohn in 1892. The patient was a 23-year-old woman with depressed pink-to-red lesions on her elbows that were noted to have an atrophic, wrinkled appearance . A year previously, Schweninger and Buzzi described a 29-year-old woman with multiple sac-like tumors that demonstrated herniation upon palpation; the lesions were located on the trunk and upper extremities but lacked inflammation .
Epidemiology
Several hundred cases of anetoderma have been reported in the world literature since the original report. Primary anetoderma favors young adults between 15 and 25 years of age and occurs more frequently in women than men. The epidemiology of secondary anetoderma reflects that of the underlying etiologies (see Table 99.3 ).
Pathogenesis
The pathogenesis of anetoderma is not known. These lesions could be considered unusual scars, since scars also have decreased elastic tissue. The loss of dermal elastin may reflect an impaired turnover of elastin, caused by either increased destruction or decreased synthesis of elastic fibers. There are a number of proposed explanations for the focal elastin destruction, e.g. the release of elastase from inflammatory cells, the release of cytokines such as interleukin-6, an increased production of progelatinases A and B , and the phagocytosis of elastic fibers by macrophages. In addition, immunologic mechanisms may play a role in anetoderma and may explain the reported associated findings of antiphospholipid antibodies, antinuclear antibodies, false-positive serologic testing for syphilis or Borrelia spp., and positive direct immunofluorescence (see below).
In primary anetoderma, there is no underlying associated disorder and lesions arise within clinically normal skin. It can be classified into two major forms: those with preceding inflammatory lesions (the Jadassohn–Pellizzari type) and those without preceding inflammatory lesions (the Schweninger–Buzzi type) ( Table 99.2 ). This clinical classification is primarily of historical interest, since the two types of lesions can coexist in the same patient and their histopathology is often the same (i.e. inflammation has been observed in both types of lesions); the presence or absence of clinical inflammation at the onset of the disease is not related to prognosis .
| CLASSIFICATION OF ANETODERMA | |
|---|---|
| Primary anetoderma |
|
| Secondary anetoderma |
|
| Familial anetoderma |
|
| Anetoderma of prematurity |
|
Secondary anetoderma can arise in the setting of a primary inflammatory dermatosis, skin infection or cutaneous tumor, as well as in patients with systemic disorders (e.g. autoimmune). Over the past decade, an association with antiphospholipid antibody syndrome has been highlighted. Although the vast majority of cases are sporadic, familial anetoderma has been described and is usually not associated with pre-existing lesions .
Clinical features
The characteristic lesions are flaccid, circumscribed areas of slack skin that are a reflection of a marked reduction or absence of dermal elastic fibers; they can appear as depressions, wrinkling, or sac-like protrusions ( Fig. 99.3 ). These atrophic lesions vary in number from a few to hundreds, and they typically measure 1–2 cm in diameter and are skin-colored to blue–white in color. The skin surface can be normal in appearance or wrinkled, and a central depression may be seen. Coalescence of smaller lesions can give rise to larger herniations.
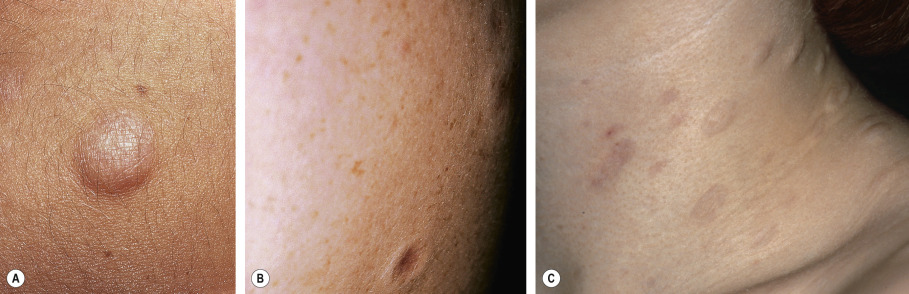
The examining finger sinks into a distinct pit with sharp borders as if into a hernia ring. The bulge reappears when the pressure from the finger is released. This clinical finding is referred to as the “buttonhole” sign and is similar to that observed in neurofibromas.
Predilection sites for these asymptomatic lesions are the chest, back, neck, and upper extremities. Primary anetoderma usually develops in young adults, and new lesions often continue to form for many years as the older lesions fail to resolve.
Secondary anetoderma implies that the characteristic atrophic lesion has appeared in the same site as a previous specific skin lesion. Some authors also consider lesions associated with an underlying disease (e.g. HIV infection, antiphospholipid antibody syndrome, autoimmune thyroiditis) as secondary anetoderma; however, in this instance, the atrophic areas do not necessarily develop within areas of known inflammation. Evaluation for the presence of antiphospholipid antibodies should be performed before patients with idiopathic anetoderma are labeled as having primary anetoderma . The range of heterogeneous conditions associated with secondary anetoderma are outlined in Table 99.3 . With the exception of distribution (and perhaps size), the clinical features are the same as those of primary anetoderma.
| SECONDARY ANETODERMA – ASSOCIATED CONDITIONS | |
|---|---|
| Infectious |
|
| Drugs |
|
| Inflammatory |
|
| Autoimmune |
|
| Tumors and depositions |
|
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


