Fig. 3.1
Typical erythematous crusted and excoriated plaques with lichenification in two children with atopic dermatitis

Fig. 3.2
Typical erythematous crusted and excoriated plaques with lichenification in two children with atopic dermatitis

Fig. 3.3
Hyperlinear palms are a common finding in patients with AD (Photo courtesy of Alfons Krol, MD)
Table 3.1
American Academy of Dermatology Criteria for AD
Essential features: |
Pruritus |
Eczema (acute, subacute, chronic) |
Typical morphology and age-specific patternsa |
Chronic or relapsing history |
Important features—seen in most cases, adding support to the diagnosis: |
Early age of onset |
Atopy |
Personal and/or family history |
Immunoglobulin E reactivity |
Xerosis |
Associated features—these clinical associations help to suggest the diagnosis of atopic dermatitis but are too nonspecific to be used for diagnosing AD in isolation: |
Atypical vascular responses (e.g., facial pallor, white dermatographism, delayed blanch response) |
Keratosis pilaris/pityriasis alba/hyperlinear palms/ichthyosis, ocular/periorbital changes |
Other regional findings (e.g., perioral changes/periauricular lesions), perifollicular accentuation/lichenification/prurigo lesions |
Exclusionary conditions—it should be noted that a diagnosis of atopic dermatitis depends on excluding conditions, such as: |
Scabies |
Seborrheic dermatitis |
Contact dermatitis (irritant or allergic) |
Iichthyoses |
Cutaneous T-cell lymphoma |
Psoriasis |
Photosensitivity dermatoses |
Immune deficiency diseases |
Erythroderma of other causes |
Management Strategies
Management begins with disease education, followed by the creation of an individualized treatment plan using a sequential approach, primarily based on disease severity. Key educational points to deliver during the initial encounter with a patient and family include information on pathogenesis, the role of food allergy, topical steroid risks and benefits, prognosis, proper skin care, and avoidance of triggers (Table 3.2). Families should be asked about the presence of immediate hypersensitivity symptoms to foods such as lip swelling, urticaria, abdominal pain, or vomiting within 2 h after food consumption. If these are not present, there are few data to support the idea that foods contribute to the eczematous lesions, and food avoidance should not be routinely recommended [9].
Table 3.2
Key educational points to be delivered in first visit
The cause of the disease | The cause of AD may be thought of as a disease driven by genetic and environmentally derived alterations in both the skin barrier and immune regulation |
The prognosis and disease course | Parents should be informed that AD is a chronic disease that needs continued management. Early aggressive control of the inflammation will improve a patient’s itch and quality of life |
Role of food allergy | Patients with atopic dermatitis are more likely to have immediate reactions to foods like egg, milk, and peanut. However, in the absence of immediate hypersensitivity symptoms, there are no convincing data that altering a child’s diet will improve the eczema |
Avoiding triggers and exacerbating factors | Avoid common triggers to reduce itch such as contact with wool, a warm environment, harsh soaps, or lotions with fragrance |
Steroid phobia and steroid side effects | A thorough explanation of the risks and benefits of topical steroids should take place with a discussion on how those risks may be mitigated |
Patient support and education | Written instructions and information regarding patient support organizations such as the National Eczema Association (nationaleczema.org) are important resources for patients |
Skin care | Gentle skin care should be encouraged with the use of mild cleansers and the daily use of emollients (moisturizers) |
Treatment Overview
Management can be roughly thought of in two parts—a Clearance Phase where inflammation becomes controlled rapidly and a Maintenance Phase, where therapy choices should consider long-term safety. If flares occur during maintenance therapy, an abbreviated Clearance Phase protocol may be needed.
Clearance Phase
Very mild disease may be managed with emollients alone. For mild to moderate disease, topical steroids should be prescribed in adequate quantities and potency to achieve near clearance of the disease within 1–3 weeks. Topical steroids may be applied once or twice daily, with data showing little clinical difference between the two frequencies [10]. Ointment preparations are generally preferred over creams and lotions because of their enhanced efficacy and reduced possibility of causing stinging or contact dermatitis. One small study found that daily bathing followed immediately by topical steroid ointments (“soak and seal”) led to 95 % of patients with moderate to severe disease achieving mild disease or better after 1–2 weeks of treatment [11]. Another study found 3 days of a medium-potency topical steroid was just as effective as 2 weeks of low-strength steroid [12]. Clinically relevant hypothalamic-pituitary-adrenal axis suppression typically occurs only in the setting of inappropriate use (i.e., prolonged duration with daily application). The short-term use of daily topical steroids has proven to be safe, but topical steroid therapy should not be used daily for long-term control [13, 14]. Topical calcineurin inhibitors may be used as first-line treatment in areas of the body prone to steroid side effects such as the face, but are not often tolerated when skin is flaring due to burning and stinging (Table 3.3).
Maintenance Phase
After achieving disease control in the Clearance Phase with topical steroids, the Maintenance Phase begins. The Maintenance Phase involves reducing topical steroid use to twice-weekly application to newly active or residual lesions. This reduction in steroid frequency prevents potential side effects such as skin atrophy, telangiectasias, and striae. Topical calcineurin inhibitors may be added at this stage if twice-weekly application of topical steroids is not adequate to maintain disease control [13]. Daily use of topical steroids to the same areas of skin for longer than 4–6 weeks should be avoided. For patients with severe disease that frequently relapses, intermittent topical steroid (two times per week) or calcineurin inhibitors (three times per week) may be used on normal–appearing skin at sites that frequently flare, so-called “proactive therapy,” to reduce the probability of relapse [15, 16].
Rescue of Flares
If a patient experiences a disease flare, the cause of the flare, such as a bacterial infection of the skin, should be identified and treated. Other common causes of flares include upper respiratory viral infections, change in season, and non-adherence to the prescribed skin care or maintenance regimen. A shortened version of the Clearance Phase may then be instituted, such as 3–7 days of daily topical steroid.
Adjunctive Interventions
Twice-weekly dilute sodium hypochlorite baths (1/4 to ½ cup of household bleach to a full standard tub) may improve the severity of AD when added to routine therapy; their use may be especially helpful in patients with moderate-to-severe disease who experience frequent bacterial infections [17]. Some controlled studies also support oral vitamin D3 supplementation [18]. While oral antihistamines may be useful for treating allergic comorbidities, or may be needed as a short-term sleep aid, there are little data supporting their effectiveness in treating the itch or inflammation of atopic dermatitis [19]. Some data support the use of acupressure as an adjunctive treatment for itch [20]. Narrowband ultraviolet B phototherapy may be added if topical therapy does not achieve satisfactory results [21]. Topical calcineurin inhibitors should be discontinued during phototherapy, given the theoretical photocarcinogenesis potential of these two interventions used concomitantly.
Refractory Disease
Patients with moderate or severe disease that fail to respond adequately to intensive topical therapy are candidates for systemic therapy. The diagnosis in patients failing intensive topical therapy should be reconsidered, with consideration given to scabies infection, skin infection, contact dermatitis, cutaneous T-cell lymphoma, or other dermatosis. Oral immunosuppressive/immunomodulatory medications are the current mainstay of treatment for this subset of patients, with cyclosporine being the treatment of choice for acute disease control given its rapid onset of action and well-documented efficacy. Cyclosporine is normally started at a dose of 3–6 mg/kg/day, with higher initial doses likely leading to more rapid clinical response [21]. Once disease control is obtained with cyclosporine, patients may be transitioned to safer longer-term options such as phototherapy, methotrexate, azathioprine, or mycophenolate mofetil (Tables 3.4, 3.5).
Specific Investigations Recommended
No routine investigations are required. The diagnosis is primarily clinical and based on the presence of the criteria listed in Table 3.1. If symptoms of immediate hypersensitivity are present, referral to an allergist for allergy testing may be needed to confirm the history. Referral to an allergist may also be useful for supervised oral food challenges if children are on overly restrictive diets based on the results of allergy testing. Biopsy, immunologic evaluation, KOH preparation, or genetic testing may rarely be needed if an alternative diagnosis is suspected, or in cases of severe refractory disease.
Topical corticosteroids remain the mainstay of acute therapy in AD in evidence-based guidelines supported by extensive literature review. Evidence-based guidelines also strongly support topical calcineurin inhibitors as a proven option for long-term control. A systematic review of “proactive” therapy (i.e., intermittently treating normal-appearing skin that frequently flares to prevent flares) reported that both topical steroids and topical tacrolimus trials showed efficacy, with twice-weekly topical steroids possibly being slightly superior to tacrolimus.
Huang et al. published the first controlled trial showing the effectiveness of twice-weekly sodium hypochlorite, or dilute bleach baths, in reducing AD severity in 2009; prior to this, only anecdotal evidence was available. A randomized trial of oral calciferol (1,000 IU/day) showed improved disease severity at 1 month over placebo in children aged 2–17 years. Strong evidence is also available supporting various light modalities in AD, with narrowband UVB representing the treatment of choice.
Multiple studies document the efficacy and safety of cyclosporine in pediatric and adult patients with atopic dermatitis, with a systematic review of controlled trials revealing cyclosporine consistently improves AD severity by greater than 30–50 %. Methotrexate in controlled trials also has been found to be safe and effective in both the pediatric and adult population; one study in adults reported comparable efficacy of both methotrexate and azathioprine, but with fewer side effects, especially hematological abnormalities, in the methotrexate group. Mycophenolate mofetil has also been shown effective and safe in adult and pediatric patients; however, response can often be delayed. A randomized, controlled study in which adult patients were cleared with 6 weeks of 5 mg/kg cyclosporine, then randomized to maintenance therapy with either 3 mg/kg cyclosporine or mycophenolate sodium, showed equivalent responses; however several patients in the MMF group received oral steroid rescue, while none in the CsA group needed rescue during the treatment phase. In an adult randomized controlled trial, almost half of patients treated with interferon gamma achieved more than 50 % clearance.
Pityriasis Alba
Clinical Features of the Disorder
Pityriasis alba (PA) is characterized by ill-defined, oval, hypopigmented to pink macules, small patches or very thin plaques with fine overlying scale (Fig. 3.4). The hypopigmented lesions are typically not preceded by obvious signs of inflammation. Multiple lesions are normally present and distributed most often over the cheeks, forehead, perioral skin, and proximal arms. Less commonly, involvement of the trunk and legs can be seen (Fig. 3.5) [30–32].


Fig. 3.4
Pityriasis alba characterized by round hypopigmented macules of the cheeks (Photo courtesy of Sabra Leitenberger, MD)
Fig. 3.5
Pityriasis alba involving the arms and legs of a young girl with atopic dermatitis (Photo courtesy of Alfons Krol, MD)
PA is frequently associated with atopic dermatitis, and in these patients likely represents a form of post-inflammatory hypopigmentation. PA has been described in an endemic form associated with poor hygiene, parental income, and more siblings [33, 34]. The role of exposure to sunlight is controversial, as it has been reported to both improve PA as well as exacerbate it. A portion of the change seen with sunlight could be due to increasing pigment of skin surrounding the PA lesions. This condition is more readily apparent in children of darker skin types. The lesions are most often asymptomatic, although mild itching may be present. Histologically, PA shows spongiotic dermatitis and, less often, hyperkeratosis and acanthosis [35].
Management Strategies
Treatment can be frustrating, and in some cases may not be necessary, as lesions often resolve spontaneously over months to years. Very few controlled studies have been performed evaluating the treatment of PA. The most often recommended treatments include gentle skin care with mild cleansers, emollients, and sunscreen (Table 3.6). The efficacy of these recommendations has not been thoroughly evaluated, but they likely counteract possible causative factors. The gentle skin care combats any role xerosis and inflammation may be playing, and the sunscreen is helpful in that it lessens the contrast between involved and uninvolved skin and may help prevent new lesions. In cases with suspected dermatitis, low-potency topical corticosteroids (such as hydrocortisone 1 % or 2.5 %) and calcineurin inhibitors may be of benefit. Calcineurin inhibitors have been the most studied treatments, suggesting the role of subclinical inflammation in the etiology of PA.
Specific Investigations Recommended
PA in most cases is diagnosed clinically. Biopsy may be necessary to rule out hypopigmented mycosis fungoides if the lesions are extensive with significant involvement off of the face [36]. Testing for a loss of sensitivity to light touch, pinprick, or temperature can be useful in patients in which leprosy is suspected [37].
Biopsy if hypopigmented MF is suspected |
Skin scraping for KOH to exclude dermatophyte infection or tinea versicolor |
Testing for loss of sensitivity if patient is at risk for leprosy |
In a review of 67 cases seen at the Mayo Clinic, bland lubricants such as white petrolatum were equivalent in effectiveness when compared to 5 % ammoniated mercury in petrolatum, 2 % crude coal tar in petrolatum, Whitfield’s ointment, and Myconef ointment. A randomized, controlled study of tacrolimus 0.1 % ointment versus placebo showed improvement over the 9-week study period in hypopigmentation, pruritus, and scaling, with significantly greater improvement in pruritus and hypopigmentation in the tacrolimus group at all three time points. A similar study randomizing to three groups—tacrolimus 0.1 % ointment, calcipotriol 0.0003 % ointment, and petrolatum ointment for 8 weeks—showed improvement in all groups, but the improvement in the tacrolimus and calcipotriol groups was superior to petrolatum. A study using pimecrolimus 1 % cream also showed efficacy in pediatric and adult subjects, with clearance of scaling for most patients by week 3 and evening of pigmentation by week 12.
A study of 12 patients (skin types III–V) reported complete clearance of PA lesions with twice-weekly for 12 weeks with Excimer. Another study reported clearance or marked improvement in five of six patients treated with 4 weeks of oral methoxsalen, followed by exposure to midday summer sun or exposure to UVA cabinet.
Contact Dermatitis
Clinical Features of the Disorder
Contact with various exogenous compounds can induce an eczematous dermatitis either by delayed type IV hypersensitivity (allergic contact dermatitis), or through direct injury to skin cells (irritant contact dermatitis).
Allergic contact dermatitis (ACD) is becoming increasingly recognized as a cause of dermatitis in children and may be under-recognized, as children are not often patch tested [2, 3, 44]. ACD is classically characterized in its acute form by well-demarcated erythematous edematous and often vesicular plaques that are quite pruritic (Fig. 3.6) Chronic ACD appears as lichenified scaling plaques and can be more difficult to distinguish from irritant contact dermatitis (ICD) and atopic dermatitis (AD) (Fig. 3.7). The distribution of ACD depends on the contactant, and can be major clue to the diagnosis and likely causative agent. Geometric angular streaks raise the possibility of exposure to plants, usually of the toxicodendron family. Involvement of the eyelids, face, and anterior neck is typical for airborne allergens such as fragrances or sesquiterpene lactones. Pruritic eczematous dermatitis of the plantar and dorsal feet should raise suspicion of an ACD to a component of shoes. ACD should also be considered in patients with AD that have a sudden worsening of their disease or that is difficult to treat, especially when the flare involves areas of the body not typically involved in AD. Any asymmetric dermatitis or eruption limited to one area of the body (i.e., feet, eyelids, buttocks) should also raise suspicion for contact dermatitis. Patch testing is the standard for establishing the diagnosis of ACD and should be done when the history and clinical exam supports a diagnosis of ACD. Positive reactions must be interpreted in the clinical context to identify those that are truly relevant to the patient. The most common allergens causing ACD in children are shown in Table 3.8, below.


Fig. 3.6
Young boy with ACD to p-Phenylenediamine in a temporary tattoo (Photo courtesy of Patricia Norris, MD)
Fig. 3.7
ICD or ACD from household cleaners used on toilet seats between uses. So-called “toilet seat” dermatitis (Photo courtesy of Julianne Mann, MD)
Table 3.8
Most common allergens causing allergic contact dermatitis in children
Allergen | Most common source |
|---|---|
Nickel | Jewelry |
Cobalt | Jewelry |
Neomycin sulfate | Topical antibiotics |
Balsam of Peru | Fragrance in perfumes and toiletries; flavoring in food and drink |
Lanolin | Pharmaceutical preparations, cosmetics, and toiletries |
Fragrance mix | Cosmetics, toiletries |
Bacitracin | Topical antibiotics |
Formaldehyde | Cosmetics, toiletries, and skin- and health-care products |
Quaternium-15 | Cosmetics, toiletries, and skin- and health-care products |
p-Phenylenediamine | Hair dyes, temporary tattoos |
Management Strategies
The principal goal in treating contact dermatitis is removal and avoidance of the causative agent. For irritant contact dermatitis, the offending agent is often obvious such as soap and water for hand dermatitis. See Chap. 2 for a discussion of diaper dermatitis, another form of irritant contact dermatitis. Identification of the causative agent in allergic contact dermatitis is not always straightforward and depends on correct identification of the contactant, with a careful comprehensive history and patch testing. Parents and patients must be thoroughly educated about the compounds responsible for their ACD. Handouts describing common products containing the suspected contactant as well as suggesting alternative products that do not contain them can be helpful in educating parents and patients. For acute ACD, or in cases when avoidance alone does not lead to improvement, topical steroids can be helpful. Topical calcineurin inhibitors are often useful for treating the face or intertriginous areas [45]. In severe acute ACD, systemic therapy with oral corticosteroids or other immunosuppressants may be necessary (Table 3.9). Many authors recommend systemic treatment for acute severe ACD (such as seen with rhus dermatitis) covering greater than 10 % of the skin surface. A common regimen involves prednisone, 1 or 2 mg/kg/d, as a single morning dose for 7–10 days, with the dose tapered over an additional 7–10 days. Premature cessation may result in rebound dermatitis. Barrier creams and specialized soaps also exist for occasions when exposure cannot always be avoided, such as when outdoors in areas with poison oak/ivy. If the causative allergen can be successfully identified and avoided, long-term treatment is usually not necessary. As is the case with many pediatric conditions, research specifically evaluating the treatment of contact dermatitis in children is lacking.
Specific Investigations Recommended [46–49]
For diagnosis |
Patch testing |
Multiple studies have been performed using patch testing in symptomatic children and adolescents. Most showed one or more positive patch test reaction in 62–83 % of patients (one study was only 25.1 % of those tested), of which 55–77 % were considered to be relevant. The most common sensitizers were metals, fragrances, and hair dyes.
Patch testing and removal of contactant | Expert opinion |
Topical corticosteroids | A* |
Avoidance of irritants | C* |
Emollients (lipid rich moisturizers) | A* |
Barrier creams (dimethicone or perfluoropolyethers) | B* |
A thorough systematic review of 49 studies (pulled from 413 initial articles) of adult patients was performed with multiple evidence-based findings. Barrier creams containing dimethicone or perfluoropolyethers, cotton liners, and softened fabrics were able to prevent irritant CD. Lipid-rich moisturizers both prevent and treat irritant CD. Topical skin protectant and quaternium 18 bentonite (organoclay) can prevent rhus dermatitis. Diethylenetriamine pentaacetic acid (chelator) cream prevents nickel, chrome, and copper dermatitis. Potent or moderately potent steroids (fluticasone propionate 0.05 %, clobetasone butyrate 0.05 %, and clobetasol propionate 0.05 %) effectively treat allergic CD.
Multiple studies report statistically significant improvement in adult patients with ACD with tacrolimus 0.1 % ointment when compared with petrolatum or vehicle alone. In studies comparing tacrolimus 0.1 % ointment and mometasone ointment, both showed efficacy. Tacrolimus 0.1 % ointment in the treatment of eyelid ACD led to improvement in erythema, edema, scaling, and lichenification at 30 days of treatment, though fissuring did not improve. In a study of adult patients with nickel-induced ACD, pimecrolimus 0.6 % cream was comparable to betamethasone-17-valerate 0.1 % cream and was more effective than the vehicle.
Several authors recommend oral prednisone in cases of widespread and/or severe reactions. Dosing recommendations include 1 mg/kg/day for 10–14 days (>10 % body surface area) up to >3 weeks (severe reactions, such as from poison ivy exposure).
Studies show treatment with UVB or PUVA can lead to improvement in ACD, though amount and duration of improvement varied. One study of ten patients treated with UVB led to complete resolution of hand ACD; however, treatment duration was lengthy at 5 months) and maintenance therapy was required. Two studies compared UVB and PUVA. One using left–right comparison of the two modalities showed no significant different between the two, though side effects were seen more often in the PUVA group. The other study showed significant improvement but not clearance in UVB-treated patients, whereas all patients treated with PUVA has clearance of their dermatitis, but over half experienced relapse within 3 months.
Juvenile Plantar Dermatosis
Clinical Features of the Disorder
Juvenile plantar dermatosis (JPD) is characterized by shiny erythema and superficial scaling primarily involving the weight-bearing surfaces of the forefoot, toes (especially great toes), and the heel (Fig. 3.8). In more extensive cases, painful fissures may develop. JPD presents in school-age children and early adolescents and typically resolves by age 12–16. Pruritus is variably present. The etiology is unclear but it is often associated with a personal or family history of atopy. There may also be a relationship with excessive sweating and occlusive footwear [2, 3].
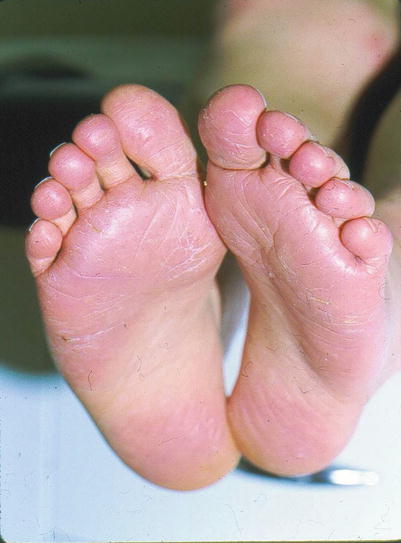
Fig. 3.8
Shiny erythema and superficial scaling on the weight-bearing surfaces of the forefoot (Photo courtesy of Alfons Krol, MD)
Management Strategies
Interventions are aimed at preventing maceration and irritation from repeated moistening and drying of the plantar skin. This is accomplished by wearing breathable footwear, cotton socks, and application of barrier emollients such as white petrolatum. Changing out damp socks with a fresh dry pair after applying white petrolatum to the affected skin can be a useful strategy. In more severe cases with significant pruritus and fissures, mid- to high-potency topical steroids may be helpful (Table 3.12). Topical tacrolimus 0.1 % used in combination with emollients has also been reported to be helpful (Table 3.13). In patients with significant hyperhidrosis, aluminum chloride can be helpful.
Specific Investigations Recommended [59]
For diagnosis |
Skin scraping for KOH to exclude dermatophyte infection |
Biopsy rarely necessary but can be useful if psoriasis is suspected |
Patch testing if ACD is suspected |
The diagnosis is primarily clinical. Potassium hydroxide preparation can be useful to evaluate for tinea pedis, although the absence of interdigital involvement supports a diagnosis of juvenile plantar dermatosis. Patch testing is helpful in cases where allergic contact dermatitis (ACD) is suspected. ACD involving the feet typically is more pruritic than JPD and often involves the dorsal aspects of the feet. Palmoplantar psoriasis can involve the soles but tends to be more sharply demarcated, have thicker scale, and typically extends beyond the weight-bearing surfaces.
Corticosteroids | D |
Emollients
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





