Arthroscopic Management of Discoid Lateral Meniscus in the Pediatric Knee
Benton E. Heyworth
Operative Indications
Symptomatic lateral discoid meniscus
Symptoms may include lateral-sided knee pain or mechanical symptoms (clicking, clunking, snapping, popping, locking) which adversely affect a child’s gait (ie, limping), activities of daily life, sports, or participation in recreational activities (eg, free play, playground activities, gym class)
Lateral discoid meniscus tear
Even in the setting of minimal or no symptoms, the presence of a true tear within a discoid meniscus should warrant consideration of proactive surgical treatment, so as to remove the tear, “stabilize” the free edges of the meniscus, and prevent the tear from propagating or worsening. Progression of a small tear to a large, complex, or degenerative tear may preclude meniscal preservation and lead to the need for subtotal or total meniscectomy, after which an accelerated rate of arthritis may be predicted at a young age1,2,3,4
Radiologic assessment of a tear within a discoid meniscus can be more complex than that in a normal meniscus. Therefore, a higher resolution, higher quality (eg, 3 T magnet) magnetic resonance imaging (MRI) study may be helpful
One or more different tear patterns may be seen, including radial, vertical, horizontal, or complex/degenerative tears, as well as meniscocapsular separation or instability. Intermediate or high signal abnormality in the middle of a complete or near-complete discoid meniscus is not necessarily a horizontal cleavage tear, particularly if there is no extension of the signal abnormality to the central free edge or to the superior or inferior meniscal surface
If intrasubstance signal abnormality is detected in the absence of significant symptoms, and the shared decision-making process with a patient’s family results in a decision for nonoperative treatment, close observation or monitoring should be pursued, in the form of annual clinical checks and consideration of serial MRI studies
If there is worsening of the radiologic appearance, or if symptoms worsen, surgical treatment may allow for a more successful overall meniscal preservation strategy, though this has not been clearly established in the literature
While more prospective research is needed on the controversial topic of timing of discoid meniscus surgery, the author believes that a “wait and see” approach—in which surgery is deferred until symptoms become severe or functionally limiting or more definitive tear patterns are identified—may represent a suboptimal strategy, from a long-term joint preservation perspective
Equipment
Basic knee arthroscopy setup
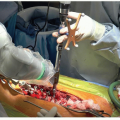
Arthroscopic basket punches (complete array of baskets needed, including 45° curved, 90° side-biters, back-biters) (Figure 35.1)

Figure 35-1 ▪ Photograph of the array of arthroscopic basket punch instruments that may be needed for a discoid meniscus, including straight baskets, 45° curved baskets, 90° “side-biters,” and 180° “back-biters.”
Arthroscopic shavers—both straight and curved shavers may be helpful, with the latter particularly helpful for accessing undersurface of anterior horn from the inferomedial portal
Arthroscopic long-handled, thin meniscal scalpel (aka, “banana blade”) may be particularly helpful in performing partial debridement of the anterior horn, which may have excessive tissue or a bulky appearance, not easily accessed with arthroscopic baskets
Meniscal repair instrumentation—complete array of instruments needed, including:
all-inside meniscal repair sutures/implants for posterior horn,
zone-specific inside-out meniscal repair cannulas, for passing of needle-based meniscal repair sutures, and
spinal needle and/or “micro” suture passing instrumentation for outside-in passage of 2.0 PDS sutures through anterior horn using “Mulberry knot” technique or double suture passage technique
Basic open instrumentation kit (eg, “ortho basic” or “foot kit”)—these instruments are used to create small anterolateral or posterolateral incision to facilitate suture retrieval and extracapsular, capsular-based suture tying, if inside-out or outside-in meniscal repair sutures were utilized
Positioning
Standard supine positioning
A lateral knee post is used on a standard operating room (OR) table to ensure adequate valgus stress for visualization of the medial compartment during the diagnostic arthroscopy portion of the procedure
Most of the surgery is performed with the knee in the figure-4 position (see Figure 35.2), in which the knee is flexed to 60° to 100° of flexion and the hip is externally rotated
Opening of the lateral compartment, to minimize the chance of iatrogenic injury to the lateral femoral condyle or tibial cartilage surfaces, is best achieved by placing the lateral aspect of the foot of the operative side on the anterior surface of the mid-tibia of the sterilely draped contralateral extremity, which allows the surgical technician or assistant to hold the foot in place (short arrow) in an optimal position (Figure 35.2)
Additional gapping of the lateral compartment can be achieved by simultaneously applying a downward force on the medial aspect of the knee
These two steps (securing the foot, varusizing the knee) may be performed selectively, only when sharp instruments are passed through the lateral compartment, so as to free the hands of the assistants for instrument passage and other functions
 Figure 35-2 ▪ Photograph illustrating the use of a spinal needle (long white arrow) with the right knee in the figure-4 position for optimization of the location and vector of the medial working portal for access to the lateral compartment and involved area of a discoid meniscus. During key portions of the procedure, when additional varus force is needed to open the lateral compartment, an assistant may hold the foot in place (short black arrow) on top of the anterior aspect of the sterilely draped contralateral leg in the mid-tibia region. |
Surgical Approach
Portals
Establish a standard inferolateral portal just lateral to the lateral border of the patellar tendon and just proximal to the anterior horn of the lateral meniscus. For optimal viewing of the entire lateral compartment, the medial working portal should be established with the knee in the figure-4 position using a spinal needle under direct arthroscopic visualization (see Figure 35.2, long arrow)
The optimal position for the medial portal to allow instrumentation access to the entire lateral compartment is usually 1 cm proximal and 1 cm medial (long arrow) to the typical inferomedial portal position (Figure 35.3)
Alternatively, a standard inferomedial portal (see Figure 35.3, short arrow) can be established, with plans for creation of a secondary accessory portion in this proximal, medial position, if needed, later in the procedure

Figure 35-3 ▪ Photograph of skin markings on anterior aspect of a right knee, prior to discoid meniscus surgery. The optimal medial working portal (long arrow) for access to the lateral compartment, and all parts of a discoid meniscus, particularly the anterior horn, is usually more medial and more proximal/superior than the standard inferomedial working portal (short arrow).
Finally, because the medial portal is often utilized as the viewing portal for portions of the procedure, consideration may be given toward creation of a secondary, accessory lateral portal that is 1 cm proximal to the typical inferomedial portal position. Specifically, this higher portal position may facilitate more atraumatic trimming of the anterior horn discoid meniscus tissue, particularly if this step is performed with arthroscopic, long-handled, thin meniscal knife (or “banana blade,” which is often used for precision trimming of excessive anterior horn tissue)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree