Photoaging
In order to understand how to treat facial aging, one needs to understand how the skin ages. Skin changes occur as a result of genetic factors (intrinsic aging) and environmental factors (extrinsic aging). Ultraviolet (UV) light has the most significant impact on photoaging, but smoking, medications, and poor nutrition can also influence the skin.
Chronically sun-exposed skin will demonstrate a typical appearance referred to as solar elastosis or dermatoheliosis. When evaluated microscopically, histologically fragmented and disorganized elastic fibers are found in the upper dermis, and collagen degradation is identified. Cellular atypia with varying-sized cells are also present. Clinically aged skin demonstrates both fine and coarse wrinkles as a result of collagen loss. Dryness, rough texture, and sallow complexion are seen on sun-exposed skin, likely due to disorganized collagen and uneven thickness of the skin resulting in poor light reflection off the skin surface. Dyschromias and increased melanogenesis also occur, leading to uneven pigmentation of the skin. Functional abnormalities of the skin occur as well. These include easy dispensability of the skin, uneven tanning due to areas of hypopigmentation, and skin that is easily traumatized with resultant skin sloughing and ecchymosis.
Ideal cosmeceutical products, therefore, are those that increase the amount and quality of collagen in the skin, increase the hydration of the skin, and improve skin texture with the least amount of side effects.
34.3 Retinoids
Retinoids are a diverse class of vitamin A products. Vitamin A is a necessary dietary nutrient involved in bone development, vision, reproduction, and mucosal and epithelial integrity. It is a fat-soluble vitamin found in liver, milk, and eggs. Deficiency of vitamin A manifests as night blindness, exophthalmia, total blindness, hyperkeratosis of the skin, and increased propensity for infections. Retinoids are likely the most studied products in topical antiaging therapy, with more than 12 double-blinded, randomized controlled studies available (▶ Fig. 34.1).

Fig. 34.1 Mybody A-Team. (Courtesy of Mybody Skin Care, Phoenix, Arizona.)
Tretinoin was first used as a topical preparation on the skin in 1983, followed by Kligman’s research on the topic a few years later.2 Retinoic acid is the active form of vitamin A and long believed to exert the most significant effects. New research suggests retinol demonstrates some chemical effects without being converted to retinoid acid.3 Retinoic acid is available by prescription, whereas all other products are available over the counter.
There are three primary forms of vitamin A: retinol, retinal, and retinoic acid. Retinol is the alcohol form of vitamin A and is involved in differentiation and maintenance of the epithelium. Retinal, the aldehyde form, is involved in vision. Retinoic acid, in the form of all transretinoic acid, is the form responsible for all other biological activities within the body.
Retinoids are absorbed through the skin and primarily converted to retinoic acid in the skin. This retinoic acid is carried by albumin to the cell to be absorbed into the cell and then into the nuclear membrane. Specific nuclear retinoic acid binding proteins, once activated, stimulate gene expression of type I procollagen and type VII procollagen. The result is increased collagen production by augmenting the expression of these procollagen building blocks.
UV exposure is known to increase a family of enzymes known as matrix metalloproteinase (MMP). These enzymes lead to connective tissue damage by degrading collagen and decreasing collagen synthesis. Another way retinoids increase the amount of collagen is by blocking this UV-induced activation of collagen-degrading enzymes to limit the amount of collagen degradation.
Retinoids are very potent products that exert their effects at low concentrations. Duell et al performed a study to assess the skin absorption of the various forms of retinoids. They found a minimum concentration of 0.025% was required for retinol to have an effect.4 Levels below this did not induce cellular changes but, interestingly, higher levels did not show significantly more benefit. Retinoic acid was found to be more potent and exert its cellular activity in one half the time of retinol.
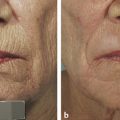
Multiple studies have demonstrated that topical tretinoin improves the skin at both the dermal and epidermal level.4,5 The epidermis shows a decrease in epidermal thickness, reduction of corneocyte adhesion, and decreased melanin production. Changes in the dermis include increased collagen production, decreased collagenase, and decreased glycosaminoglycans. These events result in the clinically demonstrable improvement of fine lines and coarse wrinkles, improvement of skin roughness, reduction of sallow coloring, and reduction of pigmentation in the skin.6 Histological evidence of biopsy specimens also shows increased collagen and elastin deposition.
There are multiple strengths of retinoic acid available: 0.02, 0.025, 0.04, 0.05, and 0.10% are the most commonly prescribed formulations. To evaluate the optimal dosage, a double-blinded, placebo-controlled study was performed researching 0.025% tretinoin versus 0.10% tretinoin versus placebo. A similar statistically significant clinical improvement was seen with both tretinoin dosages compared to placebo. However, there was a greater incidence of adverse effects and skin irritation with the higher dosage.7 Therefore, there is no rationale for use of the topical tretinoin dosages above 0.025%.
Retinoid products are known to have many local adverse effects referred to as retinoid dermatitis. These side effects include erythema, pruritus, desquamation, and an exaggerated photosensitivity at the beginning of treatment. These sequelae generally begin a few days after starting treatment, peak in the first few weeks, and then wane as tolerance develops. Patients are encouraged to push through these first few weeks if possible; however, these side effects can be diminished by stopping the product for a few days or by changing to alternate-day applications.8 Avoiding astringents and any other harsh chemicals will also help decrease the associated irritation to the skin. Retinoids will also cause significant dryness to the skin initially. Utilizing a moisturizer or emollients helps with patient tolerance. Any additional moisturizers should be applied at least 30 minutes after the retinoid acid application to allow the greatest absorption of the drug.
There are numerous adverse effects of retinoids to be aware of when recommending these agents to your patients. First, is the most serious concern of teratogenicity. Oral retinoids have been shown to cause limb and craniofacial abnormalities when the fetus is exposed in utero. Cardiovascular and neural abnormalities have also been reported. No cases of fetal harm have been documented with topically applied retinoids. Specifically, Jick et al retrospectively studied a large number of patients exposed to topical tretinoin during pregnancy and no fetal harm was identified.9 Despite this evidence, given the severity of the potential adverse effects, most dermatologists and plastic surgeons will recommend against tretinoin usage during pregnancy.
Studies in mice have shown increased photocarcinogenicity, but this has not been shown in human studies. Following usage of topical tretinoin, the protective epithelial layer of the skin is diminished, and thus the skin is more susceptible to UV-induced damage. Judicious use of sunscreen is essential for any patient using topical retinoids. Despite these associated adverse effects, retinoids remain the best available and the best-studied topical products with demonstrated effectiveness in the treatment of photoaging.
34.4 Vitamin C
Vitamin C is another well-studied topical vitamin. Vitamin C is an essential water-soluble vitamin. Deficiency of vitamin C leads to scurvy, due to the inability of cross-linking of the procollagen molecules. Because of vitamin C’s necessity for collagen production, it was a natural hypothesis that topically applied vitamin C may improve the collagen degradation that occurs with photoaging (▶ Fig. 34.2).

Fig. 34.2 Physician’s Choice of Arizona Inc. (PCA) Vitamin C products. (Courtesy of Physician’s Choice of Arizona, Scottsdale, Arizona.)
Related posts:
 Combining Different Lasers in the Same Session for Optimal Outcomes in Treating Aging Skin
Combining Different Lasers in the Same Session for Optimal Outcomes in Treating Aging Skin
 Treatment of Acne Rosacea
Treatment of Acne Rosacea
 Laser Solutions for Scar Management
Laser Solutions for Scar Management
 Enhanced Medium-Depth Chemical Peels
Enhanced Medium-Depth Chemical Peels
 Private: Lasers, Peels, and Abrasion Techniques for Latino Skin
Private: Lasers, Peels, and Abrasion Techniques for Latino Skin
 Private: Laser-Assisted Lower Lid Blepharoplasty
Private: Laser-Assisted Lower Lid Blepharoplasty



