German dermatologist P. G. Unna first noted the use of trichloroacetic acid (TCA) in chemical peels as early as 1882,9 and it has been used in peeling for many years since. Previously, TCA peel depth was thought to be related to peel strength, and to a great degree that may be true. Superficial wounding has been quantitated as 10 to 30%, whereas above 50% has the potential to result in deep chemical peeling. TCA at 35 to 50% is considered by some as medium-depth peeling.10 In any event, there are many variables that impact the various concentrations of TCA upon penetration and thus the level of peeling. Although higher concentrations would certainly peel deeper and in some cases obtain a better result, in some conditions scarring can occur when used above 45%.11,12 As such, lesser concentrations in combination or as a singular agent are popular options.
TCA is both versatile and chemically stable.13 It can be utilized in varied concentrations. Further, it does not have the systemic toxicity associated with increasing concentrations, such as seen with phenol peeling.14
Combination or multiagent peel therapy has also gained widespread use in medium-depth peeling, not only due to the ability to control frosting (keratin protein denaturation) but also because of the established safety margin.15 Many of these protocols essentially break down the superficial layers to allow better penetration of TCA.
Common protocols currently employed to enhance medium peeling include 35% TCA alone or in combinations, such as TCA with Jessner’s Solution or 70% glycolic acid with TCA. However, there are other options that will allow enhanced penetration of TCA at a lower, safer concentration, thus promoting improved results.
The sequential use of reduced concentrations of TCA (15, 20, and 25%) can provide enhanced results with greater improvement than those typically obtained with lesser concentrations. The technique can reduce fine rhytids, photodamage, and dyschromias, with outcomes approaching those obtained with medium-depth concentrations as well as some fractionated laser treatments. This involves four principles: (1) proper prepeel skin care preparation, (2) good pretreatment skin degreasing, (3) peel application technique that achieves the necessary frosting, and (4) sequential peels over a period of several months.16
Proper prepeel daily skin preparation involves the use of an exfoliation cream that results in slight flaking of skin. A 5% or greater glycolic acid product is our preference. Retinoic acid is added in many cases to start the exfoliation process and is continued if necessary to obtain the desired skin preparation. Retinoic acid is discontinued 2 days prior to the peel. This process augments the skin’s reparative ability and aids penetration of the peel components.
Just before the peel, the skin is thoroughly washed and then degreased with acetone. Removal of all oils while gently abrading the skin surface also enhances peel penetration.
During the peel application, the skin is carefully observed. The peel is reapplied until proper frosting is obtained; the planned frosting level is dependent upon the skin type and goals. The frosting level is an indication of the peel depth.
The aggressive prepeeling skin care program, immediate prepeel oil removal, and proper frosting level enhance the impact of the weaker TCA concentrations, while avoiding the unpredictability of using higher concentrations. Resuming a daily skin care program once postpeel erythema has subsided in addition to repeated peels can continue to enhance results.
Although higher concentrations of TCA have been used safely, it is the authors’ opinion that this protocol using lower concentrations can accomplish equivalent benefits, with a more tolerable peel process, and easier and quicker healing.16
26.2 Patient Selection
Fine rhytids, actinic skin changes, mild-to-moderate photoaging, and superficial dyschromias may be improved with medium peeling. The ideal patient is one with fair skin and a Fitzpatrick skin type of I, II, or III. The risk for postprocedural pigmentation abnormalities is higher in individuals with darker skin.
Some patients may present with a history of postinflammatory hyperpigmentation. We exercise caution in peeling these patients and, if peeled, plan to treat any postprocedural pigmentary changes. Patients who are taking hormonal medications have a greater tendency to demonstrate postpeel pigment alterations.4 We inform these patients that pigment changes may occur, thereby requiring additional treatment after the peeling process.
Superficial acne scarring may occasionally be improved; however, other treatments may be more effective for this condition.
A careful patient history should focus on any skin disorders such as various forms of dermatitis, rosacea, acne, or herpes simplex, so that these conditions may be managed.
A history of radiation exposure, immunosuppression, autoimmune disease, and collagen-vascular disease could potentially compromise the healing process. Isotretinoin (Accutane, Roche, Basel, Switzerland) may also reduce skin-healing capacity. We recommend that patients wait 12 months from the end of isotretinoin therapy before undergoing peeling.
Some patients report that they have sensitive skin. These patients can either undergo a patch test in a small, inconspicuous location before the decision is made to go forward with a full-face, medium-depth peel, or they may be started with a 15% TCA peel.
As with all cosmetic procedures, the physician should understand the patient’s desire and communicate realistic expectations. Patients should also comprehend the importance of their roles in the pretreatment and posttreatment skin care regimen. As always, standardized photographic documentation may help record most conditions. However, some photographic details can be difficult to capture due to the limits of lighting, exposure, and camera capabilities.
26.3 Prepeel Preparation
During the initial consultation and after the patient is determined to be an appropriate candidate, the procedure, postprocedural care, alternatives, risks, complications, limitations, and likely further treatment are discussed. No promises of perfection are made. The patient must understand that deeper wrinkles are likely to remain. It is also pointed out that postprocedural erythema, edema, and facial crusting are expected and that multiple peels are often required.
Photographs are obtained with a 100-mm macro-lens. Anteroposterior (AP), oblique, and side full-face views are obtained at 1.5 m. Close-up views are also obtained at 0.6 and/or 0.8 m that include an AP view of the forehead, periorbital, and perioral regions. Oblique right and left cheek views are obtained at 0.8 m. Care must be taken to set exposure and flash settings so that skin irregularities are not obscured in the photograph.
Preprocedural and postprocedural information and instructions are given both orally and in printed form. It is essential that the patient and the patient’s family comprehend the expected early discoloration and possible swelling. Patients should also understand their roles in the outcome by properly preparing the skin and adhering to the daily skin care program. They should be realistic and recognize that a series of peels is usually needed to obtain the best result.
We do not normally prescribe antiviral medications unless the patient reports a history of fever blisters. If so, antiviral medication may be started the day prior to the peel and taken for 7 to 14 days after the peel. Valacyclovir or famciclovir may be prescribed at 500 mg/d. If an outbreak occurs, the dose is increased.
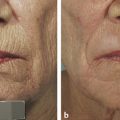
The authors’ pretreatment program requires a minimum of 2 weeks of aggressive skin preparation with exfoliation, hydration, and protection. Excellent improvements can be seen with this regimen alone (▶ Fig. 26.1 and ▶ Fig. 26.2). Sunscreens and a strong glycolic acid-based exfoliator are used. Glycolic acid is an alpha hydroxy acid derived from sugarcane that initiates keratinocyte dyscohesion and increases type I collagen and hyaluronic acid deposition in the skin.17 The tightening properties of collagen and the hydrophilic properties of hyaluronic acid give the skin a fuller and less wrinkled appearance.16 Tretinoin is added in many cases of thick, oily, or resistant skin. Tretinoin (e g., Retin A, Ortho Dermatologics, Los Angeles, California) not only thins the stratum corneum in thick-skinned individuals but also helps prepare the skin for chemical peels by activating dermal fibroblasts and stimulating increased collagen deposition.16 If the patient cannot tolerate the tretinoin, we use the glycolic cream twice per day as single-modality preparation. The cream application is usually stopped 2 days before the procedure. Hydroquinone is added to the pretreatment regimen, when faced with pigmentation considerations such as spotty hypopigmentation and melasma. Hydroquinone blocks the production of melanin precursors and, consequently, epidermal neopigmentation during the healing phase by inhibiting the enzyme tyrosinase.18 Hydroquinone 4% cream may be recommended for those patients with Fitzpatrick skin type III or higher, or for those patients with pigmentary dyschromias.16

Fig. 26.1 Prior to the initiation of skin care regimen. (Courtesy of The Langsdon Clinic, Germantown, Tennessee.)
Related posts:
 Combining Different Lasers in the Same Session for Optimal Outcomes in Treating Aging Skin
Combining Different Lasers in the Same Session for Optimal Outcomes in Treating Aging Skin
 Treatment of Acne Rosacea
Treatment of Acne Rosacea
 Laser Hair Removal
Laser Hair Removal
 The Future of Rejuvenation Techniques for Aging Facial Skin
The Future of Rejuvenation Techniques for Aging Facial Skin
 Private: Lasers, Peels, and Abrasion Techniques for Latino Skin
Private: Lasers, Peels, and Abrasion Techniques for Latino Skin
 Private: Laser-Assisted Lower Lid Blepharoplasty
Private: Laser-Assisted Lower Lid Blepharoplasty



