Key points
- •
To understand the distinct anatomy of the upper and lower lids.
- •
To understand how this anatomy impacts function and physiology in the eyelids.
- •
To understand age-related changes of the lower lid and midface.
Aesthetic surface anatomy and the aging eyelid
American sculptor Hiram Powers once articulated that the ‘eyes are the window to the soul’. The ocular and periorbital regions represent not only one of the most perceptible and impressionable areas of human anatomy, but one of the most intricate. Subtle differences or abnormalities in surface anatomy may have perceptible implications in human interaction. For example, a patient who suffers from ptosis may give the impression that they are sleepy or disinterested whereas a patient with proptosis may present an aura of surprise or irritability. A critical understanding of the anatomy of the lids as well as anticipating how manipulation of deeper structures impacts surface aesthetics is the key to correcting pre-operative deformity and creating a youthful appearing eye.
The topographic anatomy of the eyelids and periorbital region is illustrated in Figure 1.1 . The hallmark of a youthful eyelid is a smooth contour extending from the brow to the upper lid and from the lower lid to the cheek and midface. In a balanced, youthful face, the eyebrow is lower medially and higher laterally. In females, the highest portion of the arch is usually at the junction of the medial and lateral thirds of the brow. The lid–cheek junction lies over the infraorbital rim and is usually 5–12 mm below the lower lid margin. The palpebral fissure is the opening between the eyelid margins. The standard opening is 28–30 mm horizontally and 9–10 mm vertically when the lids are open.
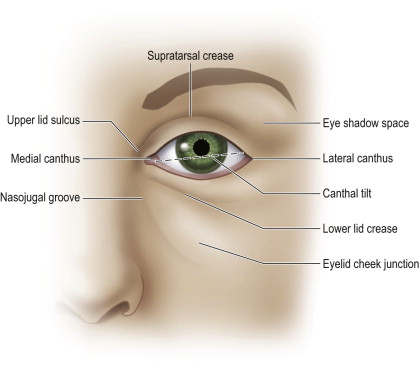
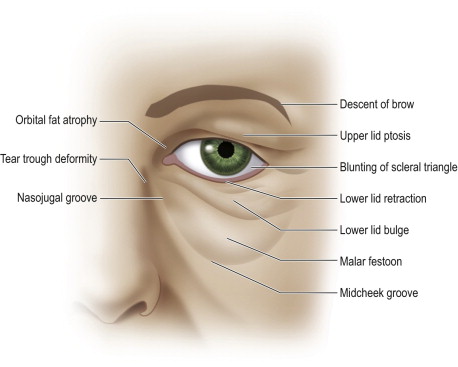
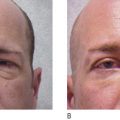
The commissures are the junction points where the upper and lower eyelids meet medially and laterally, whereas the medial and lateral canthi are the angles formed by the eyelids at these commissures. The lateral canthal angle is generally positioned approximately 2 mm superior to the medial canthal angle, giving the eyelid a slightly upward and lateral canthal tilt. In primary gaze, the upper eyelid margin is positioned approximately 1.5 mm inferior to the superior limbus of the cornea. The lower eyelid margin is found at or just above the inferior limbus. The upper eyelid margin forms a smooth arch with the highest point positioned between the medial limbus and the pupil. With age, there is a gradual lateral shift of this point as the tarsal plate migrates laterally. Several age-related changes to the eyelids and periorbital region are illustrated in Figure 1.2 .
The supratarsal crease of the upper eyelid is a fixed landmark that is formed by the dermal insertion of the levator aponeurosis after it passes through the orbicularis muscle. A smooth, slightly convex contour between the supratarsal crease and the mid to lateral brow defines a youthful and attractive eye shadow space. With aging, brow descent, orbital fat atrophy and skin/muscle excess can contribute to a tired, hollow appearance. In patients undergoing blepharoplasty or levator surgery, the lid crease must be reformed by suturing the eyelid skin and pretarsal orbicularis to the levator aponeurosis. Failure to do this maneuver may result in late-onset ptosis.
With aging, there is a downward slant from the medial to lateral canthus. The eye may appear hollow, with definitive demarcation from the brow to the upper lid and the lower lid to the cheek and midface. In most individuals, the palpebral fissure becomes smaller and rounder with age. The lid–cheek junction lies well below the infraorbital rim, 15–18 mm from the lid margin. Medial septal attachments and fat herniation can create unsightly nasojugal grooves and contribute to a tired appearance.
The anterior lamella
Skin and orbicularis oculi
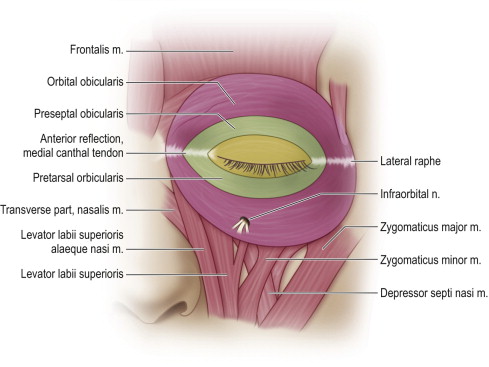
The skin of the eyelids is exceptionally thin and contains minimal subcutaneous fat. Deep in the dermis lies the orbicularis oculi muscle which is divided into three major divisions including the pretarsal, preseptal, and orbital divisions. These divisions are illustrated in Figure 1.3 . The superficial and deep components of the orbicularis in the medial canthal region function to assist tear transport through a lacrimal pump to the lacrimal sac. The orbital orbicularis is the largest division of the orbicularis muscle and functions to protect the globe with forced eyelid closure as well as medial brow depression. The pretarsal fibers have dense attachments to the upper and lower lid tarsal plates.
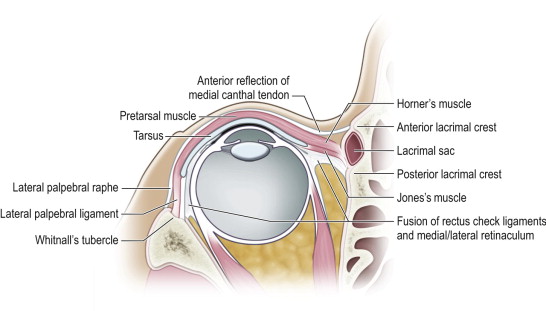
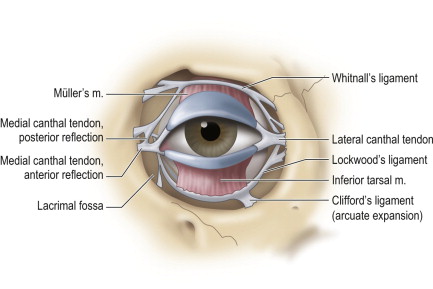
The medial and lateral muscular attachments of the orbicularis are important for normal closure of the palpebral fissure. The medial orbicularis surrounding the medial canthus is the location of the dominant blood supply and innervation and contributes to the major contractile forces used for involuntary blinking, lacrimal pump, and eye protection. Medially, the deep head of the pretarsal muscle, known as Horner’s muscle, originates at the posterior lacrimal crest of the lacrimal bone. The superficial head of the pretarsal muscle originates from the anterior reflection of the medial canthal tendon. Laterally, both the superior and inferior pretarsal orbicularis insert into the zygomatic bone at Whitnall’s tubercle. The medial and lateral attachments at the canthal level are illustrated in Figure 1.4 .
The preseptal orbicularis also has a superficial and deep component. The deep muscle, Jones’s muscle, originates from the lacrimal sac fascia. The superficial preseptal muscle originates from the anterior reflection of the medial canthal tendon. Both preseptal muscles insert onto the lateral palpebral raphe, which creates the superficial component of the lateral canthus. With each blink, contraction of Jones’s muscle creates negative pressure in the tear sac thereby draining the canalicular system.
In the lower lid, the orbital orbicularis originates from the maxilla. In the upper lid, the orbital orbicularis originates from the frontal bone converging on the superficial component of the medial canthal tendon. The lateral insertion of the orbital orbicularis creates the anterior raphe along the lateral orbital rim. ( Figure 1.3 ). The lateral aspect of the orbicularis represents a fixed anchor point to the bony rim which functions as a stable fulcrum for the eyelids. This allows the forces of medial contraction to change lid position.
Motor innervation
The motor innervation to the orbicularis oculi muscle is diffuse and is illustrated in Figure 1.5 . There are several contributions from multiple branches of the facial nerve, including the frontal, zygomatic, and buccal branches. The major nerve supply enters the medial aspect through the buccal branch of the orbicularis along with an additional supply laterally from the frontal and zygomatic branches. The frontal branch also provides innervation to the upper lid pretarsal and preseptal orbicularis. If the frontal branch is injured, patients will clinically develop a weakened blink.
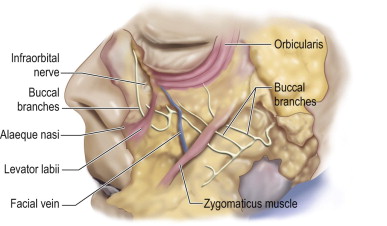
The anatomy associated with the buccal branch and its course to the orbicularis is very complex. Cadaveric studies have revealed a diffuse sensitium of nerves innervating the orbicularis oculi muscle both superficial to the origin of the zygomaticus major supplying the lateral orbicularis as well as deep continuing to supply the medial orbicularis. The medial section of orbicularis in this region has dense innervations and contributes significantly to voluntary and involuntary lid closure. This is clinically evident by impaired upper eyelid closure following an isolated medial lower lid incision over the nasolacrimal crest following dacrocystorhinostomy or Mohs surgery despite the absence of an upper lid incision.
The posterior lamella
Tarsoligamentous sling
Whereas the skin and muscle make up the anterior lamella, the tarsoligamentous sling is a network of fibrous support structures that creates the posterior lamella. An illustration of these structures is found in Figure 1.6 . The tarsal plates are fibrous plates of connective tissue that maintains the support for the upper and lower eyelids. The upper lid tarsal plate is approximately 30 mm horizontally and 10 mm vertically. Attachments to the upper lid tarsal plate include the pretarsal orbicularis and levator aponeurosis on the anterior surface, Müller’s muscle on the superior border, and conjunctiva on the posterior surface. The lower lid tarsal plate is approximately 28 mm horizontally and 4 mm in vertical dimension. Attachments to the lower lid tarsal plate include pretarsal orbicularis, capsulopalpebral fascia, and conjunctiva.
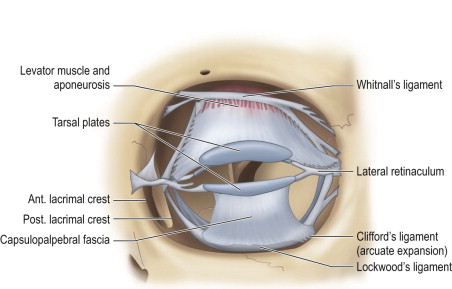
Whitnall’s ligament is a superior support structure partially formed by the fascia of levator palpebrae superioris. Laterally, it splits the lacrimal gland and attaches to its pseudocapsule while still maintaining attachments to the frontal bone of the lacrimal sac fossa. Medially, it inserts a stronger attachment at the trochlea of the superior oblique. Whitnall’s ligament acts as a pulley to convert the posterior vector of pull from the levator palpebrae superioris, originating from the lesser wing of the sphenoid, to a superior vector in order to elevate the eyelid. This vector shift prevents the upper lid from pulling away from the globe during opening.
Lockwood’s ligament is an analogous structure in the lower lid which functions as a hammock to prevent descension of the globe. It stabilizes the lower lid on down gaze while the lower lid retractors cause lid depression, essentially increasing the inferior visual field during down gaze. Lockwood’s ligament arises from the medial and lateral retinaculum and fuses with the capsulopalpebral fascia inserting on the inferior tarsal border. The arcuate expansion of Lockwood’s ligament, Clifford’s ligament, inserts into the inferolateral orbital rim and fuses with the interpad septum between the central and lateral fat compartments of the lower eyelid. The arcuate extension is often kept during blepharoplasty to maintain some septal support.
The tarsal plates of the upper and lower eyelid are attached to the orbital rim by the medial and lateral canthal tendons and retinacular support structures. The canthal ligaments are the fibrous extensions of the tarsal plate, while the canthal tendons represent the true insertion of the deep heads of the orbicularis oculi muscle to the bone, thereby constituting a true tendon.
The medial canthus is a complex structure that forms the medial fixation point for the medial commissure. The medial canthus consists of an anterior and posterior reflection of the medial canthal tendon as well as the medial retinaculum ( Figure 1.4 , Figure 1.7 ). The anterior reflection of the medial canthal tendon inserts on the anterior nasolacrimal crest formed by the frontal process of the maxilla. The posterior reflection of the medial canthal tendon is deep to the lacrimal sac and inserts on the posterior lacrimal crest of the lacrimal bone. The medial retinaculum is a complex structure formed by the deep head of the pretarsal orbicularis, the orbital septum, the medial extent of Lockwood’s ligament, the medial horn of the levator aponeurosis, the medial rectus check ligaments, and Whitnall’s ligament. The medial retinaculum represents a fixed fulcrum point to maintain medial canthal position. This allows the orbicularis muscles to act on lid position rather than displacing medial canthal position.
Related posts:
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Lower lid blepharoplasty with fat grafts for correction of the tear trough
Lower lid blepharoplasty with fat grafts for correction of the tear trough
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 No touch lower blepharoplasty
No touch lower blepharoplasty
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


