Key points
- •
By the end of the third decade, aging is manifested by skeletonization of the periorbital area.
- •
The aging lower eyelid appears to elongate with increased height of the lower eyelid, and a defined eyelid–cheek junction.
- •
The amount of orbital fat varies, but instead of removing the fat as in traditional blepharoplasty, most can be preserved and transposed over the orbital rim with a ‘septal reset’.
- •
In addition to the septal reset, the cheek fat and cheek musculature must be moved towards the orbit in a superior-lateral vector to produce a high cheek mass compatible with young anatomy.
- •
The periorbital rejuvenation is created by a unique comprehensive procedure including a forehead lift, facelift, necklift, and a zygorbicular midface lift called a composite rhytidectomy that creates harmony in facial rejuvenation.
Introduction
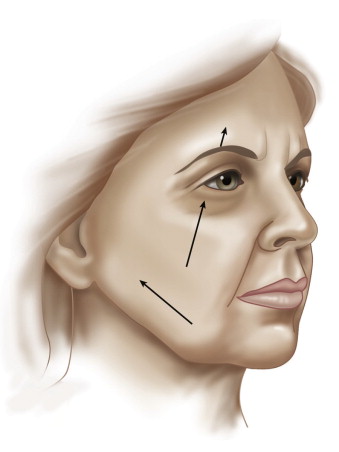
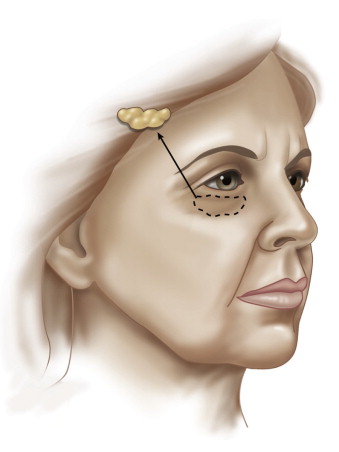
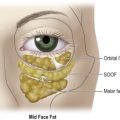
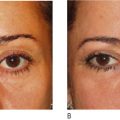
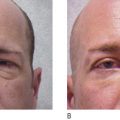
The composite facelift is a comprehensive facial procedure designed to rejuvenate every part of the aging face, with particular emphasis to the periorbital area, an area largely ignored in the many years of facelift history. In general, conventional facelifts include subcutaneous or skin lifts, SMAS procedures, and deep plane or ‘malar fat’ procedures, and all share the common characteristic of moving the tissues of the face and cheeks in a superior lateral vector ( Figure 8.1 ). By contrast, the composite facelift moves the cheek and malar tissues in a superior medial vector ( Figure 8.2 ). The other difference that distinguishes a composite facelift from a conventional procedure is the treatment of the orbital fat of the lower eyelid. Since 1928, removal of lower eyelid fat has been done routinely when performing a lower blepharoplasty ( Figure 8.3 ). In composite facelifting, an arcus marginalis release and septal reset is done, as the septum orbitalae is preserved and sutured over the orbital rim ( Figure 8.4 ).


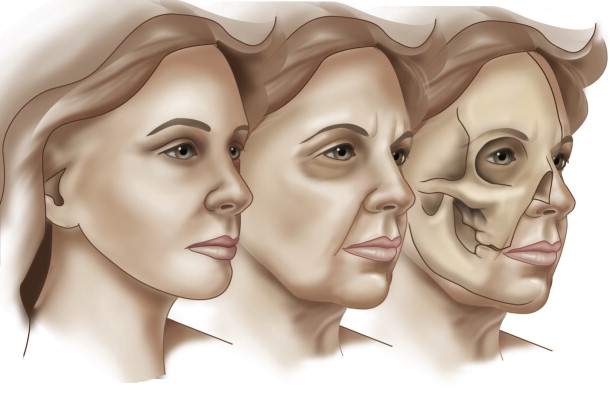
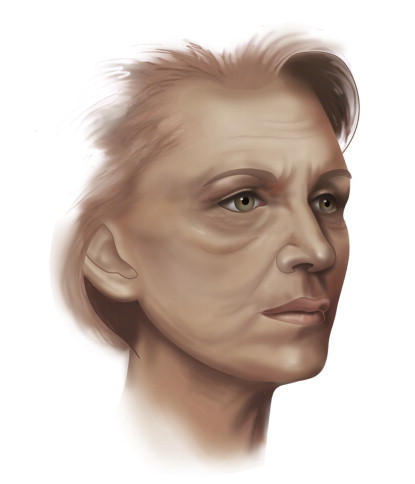
The advantage of this approach lies in the understanding of the changes that are normal to the aging of the human face. In youth, the lower eyelid and cheek junction is blended because the contour of the lower eyelid is convex. In the course of normal aging, the periorbital area becomes skeletonized, as the soft tissue change allows the appearance of the underlying bony anatomy not previously seen ( Figure 8.5 ). Thus, the soft tissue contour becomes concave, and an ‘eye socket’ slowly develops, usually around the end of the fourth decade. The vertical height of the lower eyelid elongates and the eyelid–cheek junction becomes clearly defined. The two unique features of composite facelift, the superior-medial vector of lift and resetting of the periorbital fat and septum, can dramatically change the aging face by returning the youthful convexity to the periorbital area and obliterating the aging eyelid–cheek junction.
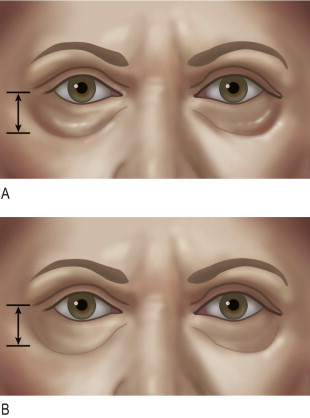
Of equal importance is that the composite facelift not only produces a more harmonious rejuvenation but it prevents the possible unfortunate results commonly seen following conventional procedures. The ‘hollow eye’ and ‘lateral sweep’ are typical results that may appear following conventional procedures, since fat removal and an unopposed lateral vector SMAS lift can create a more concave lower eyelid ( Figure 8.6 ) and pull of the lower face ( Figure 8.7 ). In patients who have these signs following previous facelifts, the composite facelift can effectively reverse these unwanted results.
The evolution of this technique took place over a 25 year period and was developed by the senior author. Beginning in 1973, the Skoog type facelift was adopted by the senior author, as this was the first procedure that moved deep tissue rather than skin. Skoog included the platysma of the lower face, later known as SMAS. This was modified in 1978 as a ‘tri-plane facelift’ which kept the platysma and skin of the lower face en bloc, but included a preplatysma cervical dissection, and the creation of a ‘meso-mandibularis’ separating the preplatysma neck undermining from the subplatysmal lower face plane. This continued to be used until 1985. Attention was then directed at the nasolabial fold which was usually not well corrected in conventional facelift surgery. That was when the cheek fat or malar fat was added to the facelift flap, and was published as the ‘deep plane’ facelift. At this point there was still no periorbital rejuvenation. In 1990, the orbicularis oculi was added to the flap, and the first real step in creating a more youthful eyelid was accomplished. This was published as the composite facelift since the flap contained skin, muscle, and fat.
In 1991, the first step was taken to preserve the lower eyelid fat by releasing all of the fat and suturing the fat across the orbital rim. The septum orbitalae was removed for fear of scar contracture of the lower eyelid. This was published as the arcus marginalis release. Although effective, the orbicularis muscle repositioning and fat transfer was not always predictable, so in 1996 this was further modified to include the zygomaticus musculature coupled with the orbicularis oculi in the flap and this was published as the ‘zygorbicular dissection’ for midface elevation. At the same time, the orbital fat transfer over the orbital rim was modified to include the septum orbitalae. This was more clearly described as the ‘septal reset’ and was recently published as such.
The advantage is clear that this procedure results in a more harmonious and youthful appearance without the stigma of a facelifted or surgical appearance. The disadvantage is that as in all cases of advanced surgery there is a learning curve. The surgeon is also required to perform a complete rather than a partial rejuvenation operation. Nevertheless, patients who understand the advantages usually accept the slightly longer recovery time knowing that the results will be worthwhile in that they are long lasting and disallow the chances of a ‘lateral sweep’.
The composite facelift is indicated for all patients seeking facial rejuvenation, and used for both men and women. For young patients who have only aging signs of the eyelids, an upper blepharoplasty and cheek lift including the septal reset would be sufficient. This procedure is always used for secondary facelifts and is uniquely suited to reverse the unfortunate results occasionally seen following facelifts.
Indications
The composite facelift has been shown to be applicable either as a primary or a secondary procedure to essentially every patient type. It is ideal as a primary procedure because the periorbital rejuvenation that is unique to this operation is indicated for any aging face as each one demonstrates the inevitable skeletonization of the periorbital region. It is indicated in both the female and male patient. Because the superior medial vector of the midface lift may cause bunching of the temple area, a forehead lift is obligatory in every patient with few exceptions, and this alone ensures a harmonious result in every primary case.
As a procedure for secondary cases, it is perhaps the first facelift technique published that has been shown to correct the unattractive signs following conventional rhytidectomy. Hollow eyes following aggressive lower lid fat removal can be effectively corrected by an arcus release and septal reset. Of equal importance is the correction of the lateral sweep or ‘pulled face’ so often seen following conventional facelifts that utilize the lateral vector approach.
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Lower lid blepharoplasty with fat grafts for correction of the tear trough
Lower lid blepharoplasty with fat grafts for correction of the tear trough
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 No touch lower blepharoplasty
No touch lower blepharoplasty
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


