Key points
- •
Deepening of the tear trough is often one of the first signs of peri-orbital aging.
- •
Hyaluronic acid can be utilized effectively for non-surgical correction of the tear trough.
- •
Appropriate patient selection and knowledge of the anatomy are prerequisites to optimal correction.
- •
Deep injection prevents surface irregularities, lumpiness and visibility
- •
The tear trough is one component of facial volume loss and its correction should be performed in conjunction with that of the adjacent areas and the whole face.
Introduction
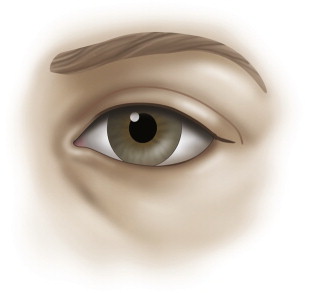
The formation of the tear trough deformity at the nasojugal groove is one of the first signs of aging around the eyes. Unique to this area, the tear trough is often present in youth but it comes to light as it deepens with age.
Most lower lid blepharoplasty techniques do not fully correct the tear trough deformity, and some can further accentuate it. Surgery may not be well justified or easily accepted in the early stages of tear trough formation in the young patient, or in a patient who has undergone a blepharoplasty with worsening of peri-orbital hollowing or with residual concavity in the tear trough.
Prior to the advent of new fillers, autologous fat was the best option for volume augmentation aside from implants. The limitations of fat however are labor intensiveness of harvest, availability, lack of predictability, risk of lumpiness around the eyes, possible change of volume with weight change, and prolonged edema.
Injectable hyaluronic acid has the advantages of gel consistency and favorable flow characteristics. These together with easy availability and reversibility make it an ideal filler for the tear trough. The longevity of the effect in this area is acceptable with the stability up to 6 months on average followed by a slow decrease after this point. The effects are expected to be satisfactory up to a year. It is not uncommon to have a lasting effect over one year.
Patient selection and indications
Patient selection is the most important variable in obtaining good results with this procedure. The best candidates are patients with good skin tone and minimal skin laxity with tear troughs and peri-orbital hollowing that is mild to moderate. This procedure has excellent utility in post-surgical patients who have an uncorrected tear trough or over-resected orbital fat. High risk candidates are those who have very thin or transparent skin, those with significant skin laxity, and those with extremely deep tear toughs and extensive volume loss.
Patients who would clearly benefit from surgery are those with orbital fat herniation and skin laxity. These patients are unlikely to obtain good results from injecting the tear trough alone and should be advised of this. This procedure is an effective surgical adjunct and I recommend it as needed after lower lid blepharoplasty.
Anatomy
The most medial aspect of the peri-orbital hollow is referred to as the tear trough deformity, and in early aging it may be the only area of concavity visible. In order to devise the optimal correction for the tear trough, understanding the anatomy of this area is critical.
The concavity in the groove may be associated with orbital fat herniation in the lower lid. The presence of excess orbital fat often camouflages the tear trough deformity and distracts from this independent problem. Removal of excess orbital fat alone does not correct the tear trough. There is individual variation in depth and morphology of the tear trough and the hollowness along the rim ( Figure 4.1 ) .
The orbicularis oculi muscle has a direct attachment to the inferior orbital rim from the anterior lacrimal crest to the medial limbus or approximately 30% of the length of the rim. Lateral to this, the attachment to the bone is via the orbicularis retaining ligaments (ORL) which have variable length at different points along the inferior orbital rim. The length increases to a maximum centrally and then decreases laterally until the ORL merges with the lateral orbital thickening in the lateral canthal region. The levator labii superioris originates just below the orbicularis oculi muscle attachment to the medial orbital rim ( Figure 4.2 ).
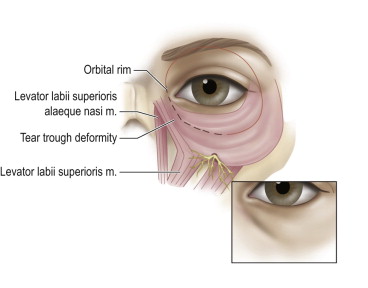
It is in this area, along the attachment of the orbicularis oculi muscle to the orbital rim, that the tear trough deformity first manifests as a concavity that gets deeper with time. The depression is bordered by the orbital portion of the orbicularis oculi, the levator labii superioris, and levator labii superioris alaeque nasi muscles. There is scant subcutaneous tissue between the skin and the orbicularis muscle, therefore the tear trough is comprised of thin skin adherent to the orbicularis muscle which is attached to the orbital rim.
The deformity manifests itself at the junction of eyelid skin above and the nasal and cheek skin below, with attenuated subcutaneous tissue overlying the maxillary bone. The tear trough is at the inferior orbital rim most medially but very quickly falls below the rim, with the maximal distance from the rim occurring centrally. The hollowing can continue laterally in more advanced aging, presenting at or just below the orbital rim, where the retaining ligaments are thicker and less distensible.
The peri-orbital pattern of volume loss is categorized into three classes based on clinical presentation:
- •
Class I is limited to the tear trough or medial orbit. These patients sometimes show very mild flattening of the central area along the orbital rim in a reverse triangular pattern.
- •
Class II patients exhibit volume loss laterally as well as medially and they may have mild volume deficiency in the medial cheek and mild flattening of the central triangle.
- •
Class III patients exhibit a depression circumferentially along the orbital rim in a full and continuous pattern of hollowing medially to laterally ( Figure 4.3 ). This pattern is often associated with more advanced volume deficiency in the medial cheek, central reverse triangle, and malar eminence as well as demonstration of an oblique cheek crease highlighting the malar bags superiorly . The depth of the tear trough is a guide as to the volume required for correction. Deeper and more extended patterns of volume loss (Classes II & III) are usually associated with relative medial cheek/midface flattening, malar volume loss, as well as volume loss in the temporal region, brow and lower face.
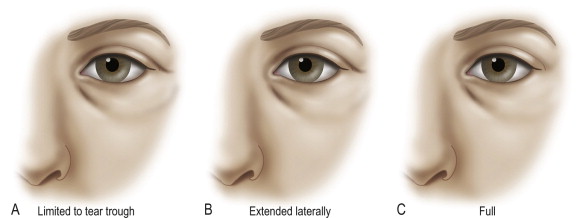
Figure 4.3
Classification of morphology of the peri-orbital volume loss patterns: a. Class I – Limited to the tear trough or medial orbit (sometimes associated with very mild flattening of the central area). b. Class II – Medial and lateral depression apparent (can be associated with mild volume deficiency in the medial cheek and mild flattening of the central triangle). c. Class III – Full depression visible circumferentially at the orbital rim (often associated with more advanced volume deficiency in the medial cheek, central reverse triangle/midface and malar eminence, as well as the oblique cheek crease extension highlighting the malar festoons).
Patients at any stage, i.e., in any of the three classes can present with excess orbital fat or significant skin laxity. These patients would benefit from surgery or surgery followed by filling of the tear trough and thus are not good candidates for this approach. An attempt at non-surgical correction using filler in this group of patients can result in suboptimal aesthetics and unsatisfied patients.
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Lower lid blepharoplasty with fat grafts for correction of the tear trough
Lower lid blepharoplasty with fat grafts for correction of the tear trough
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 No touch lower blepharoplasty
No touch lower blepharoplasty
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


