Key points
- •
The dark circle is due to atrophy of fat between the skin and the dermis.
- •
Replacement of fat or volume in the depths of the nasojugal groove will improve the overall appearance.
- •
Fat grafts injected between the skin and the muscle or into the muscle usually cause some degree of lumpiness.
- •
Release of the suborbicularis fascia connection to the arcus marginalis alone will improve the dark circle appearance.
- •
After release of the suborbicularis fascia, the structure can be maintained by fat graft injections or even by hyaluronic acid derivative injections.
Fat grafting to correct the hollow orbit
Much has been written over the past 20 years about the surgical uses of fat graft in the facial and truncal areas. My experience with fat grafting spans over 15 years and has been concentrated mainly on the face, including the perioral and the periorbital areas. Generally, fat grafting is successful but the final outcome can sometimes be unpredictable. Much of the fat grafting performed depends largely on the quality of the donor fat, the readiness of the recipient area, the techniques used to harvest the fat and the way it is inserted into the desired location.
Usually, when replacement of volume is needed in an area of the face, it is necessary to use fine needle placement with multiple passes to expand the required area. This should be slightly over-corrected with an emphasis on spreading the fat throughout the tissue instead of concentrating it in one area. There are many ways described to insert the fat into the deficient areas which include injection with a blunt cannula, injection with sharp needles, placement of the fat near the periosteum, and placement of the fat in the subdermal area. In my experience and that of others, all of these techniques have validity and this is dependent on the particular deformity involved.
In cases where fine wrinkling is being caused by shrinkage of the dermis, in my practice, it has become increasingly common to place the fat grafts in the subdermal area with multiple passes. The placement of the graft in this area expands the dermis, corrects the volume deficiency, and improves the wrinkling which is secondary to the volume loss. Although good correction has often been achieved in these cases, it is sometimes necessary to do secondary fat grafting with either fresh or frozen fat. Because it is convenient and also useful to freeze the residual fat that has not been used in the first injection series, we have used subzero freezing to preserve fat for 2–3 months. The fat grafts can be taken out of the freezer where they are stored in individual 1 cc syringes and can be injected as a minor procedure using a small amount of local anesthetic. This allows secondary correction of areas which did not respond to the first injection.
Another technique which has proved useful in fat grafting is to perform an underlifting or release procedure of the depressed area. In the nasolabial fold, fat graft is placed in the subdermal area and deeply after which the bevel of the needle is passed in a sweeping manner which releases the underlying muscle from the attachment in the dermis. In this way, the crease is completely released, becomes smoother and loses the deep crease appearance. This release technique has proven very useful in treatment of nasojugal groove depressions.
In my experience, the reason for pursuing the current technique around the orbit area is that after fat grafting, certain deformities have been observed. Some patients have presented with lumpiness or irregularities around the lower orbit or nasojugal groove area that were difficult to improve because the fat itself was often lodged in small amounts where a cannula could not retrieve it. In these instances, two techniques were used; either the skin was elevated and the fat removed from the muscle and deeper tissues or the skin bulges themselves were excised risking the possibility of a visible post-operative scar.
Over the years, the problem of the hollow orbit has been addressed by many surgeons. Techniques such as dermal fat grafting, ‘pearls’ of fat placed in the orbit, fat injections by a needle or cannula, or the simple repositioning of orbital fat by placement in the orbital rim area have been described. Some of these techniques have produced good results and in the hands of experienced surgeons have had a moderate to good success rate. Additionally, methods of correction of tear trough deformity have also been documented. Release of the lower septum and transposing orbital fat over the orbital rim is capable of improving the depression or deep nasojugal groove deformity. Modification of release of the orbital septum and readjusting the septum and muscle positions at the level of the nasojugal groove has moderate success. Some authors have described the suborbicularis oculi fascia lift, which brings soft tissue from the malar area up to the orbital rim and ‘fills’ the area of the nasojugal groove to make it smoother. In some instances, where the orbital fat herniation of the lower lid increases the appearance of nasojugal groove depression, some authors use repair of this septal hernia as a way to smooth or improve the appearance of the lower lids. While this does not directly take care of the depression of the nasojugal groove, it gives a good overall appearance to the lower lids, giving the illusion of less depth in that groove.
A midface lift is often used as a way of improving the orbital and nasojugal groove. This is achieved by pulling up a thicker tissue into the groove area and thus smoothing out the obvious depression. Non-operative means, such as placement of hyaluronic acid or collagen filler into the depressions around the orbital rim, are also used by many surgeons. Although these are not always technically perfect, they can give good results and deemphasize the depressions, which are signs of aging, around the orbit. Transcutaneous fat grafting by injection into the area is a also a useful technique. This technique emphasizes overfill to the area, which I believe is the way that small bulges or nodules are avoided. By filling the area and then refilling the area in any residual trough or depression, a smooth and full underlid area can be achieved. In some instances, particularly after previous blepharoplasty where the orbital volume itself has been reduced, fat can be placed into the post-septal area to improve orbital volume. This has been described both with the use of fat pearls and dermis fat grafts.
A unique way to correct the tear trough by inserting a small implant along the tear trough area was described many years ago by Dr Flowers. This fills out the volume of the area which has formed as a result of fatty atrophy and allows the appearance of volume replacement by adding to the bulk of the bony orbital rim. Subperiosteal cheek lift has also been performed, and this is similar to the fascia-lift and midface lift. The differences between these three approaches are simply the plane of dissection and the amount of tissue with its composite layers brought up into position. Attachment of the released subperiosteal layer to the orbital rim gives a ‘fill’ to the area which overcomes the hollowing. Additionally, simple blepharoplasty is often capable of improving the appearance of hollowing around the orbit. The conservative removal of orbital fat results in a smoother appearance and a de-emphasis of orbital rim depressions, much like repair of the herniated orbital septum ( Figure 5.1 ).

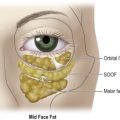
The causes of orbital rim depression have been debated, but on examination in most clinical cases they may be obvious. Where the patient has a deep nasojugal groove and has had this deformity since childhood, the distance between the skin and the bony orbital rim may be as little as 1 mm. However, in most other cases, there is a layer of subcutaneous fat between the skin and the deeper tissues of the orbital rim. This layer of fat is able to cushion that tissue and improve the fill of the area. In the face and other parts of the body, there is a constant shift in size of fatty deposits that is consistent with the aging process.
In the perioral area, there is atrophy along the lateral chin, in the marionette areas, the perioral crease areas, and the nasolabial folds. Additionally, there may be atrophy of the mid-cheek and the glabellar area, both of which may cause depression or wrinkling. However, concomitant with the atrophy of these areas is overgrowth of some of the fatty tissues in the anterior cheeks adjacent to the nasolabial folds, the jowls adjacent to the lateral mandibular ligament, and in the submental area. Where a patient has fatty atrophy in tissues around the face, there is often a remarkable loss of normal contour adjacent to the orbital rim because of this atrophy ( Figure 5.2 ).

The early part of this atrophy may occur only in the medial half of the nasojugal groove, but as the atrophy is more pronounced in some patients, it is also seen in the lateral portion over the orbital rim. This author has used techniques including midface lift, suborbicularis oculi fat (SOOF) elevation, injection of the depressions with fillers such as hyaluronic acid or collagen, and transposition of post-septal fat over the orbital rim. Many of these techniques are useful, but the most minor problems with healing can be clearly seen and often need to be corrected with surgical revision. Successes in many cases of fat injection with fine needle technique have led me to believe that injection in the submuscular area can improve this depression, particularly in the medial half of the lower lid and orbital area.
During blepharoplasty, after removal of the orbital fat pads or repair of the herniated septum containing the fat pads, injection in the lower part of the attachment of the orbicularis muscle to the orbital rim has the potential for elevating the nasojugal groove without subdermal aberrations or bulges. However, this is not the case because first the tissue needs to be released. The sharpness of the crease at the nasojugal groove area is directly related to the attachment of the layer of suborbicularis fascia to the orbital rim. While the preseptal muscle is continuous in the subdermal area above and below the orbital rim, it is held down rather tightly by the fascial attachment just at the rim. When this was approached surgically, it was not obvious that there was a layer of fascia, but simply that the tissue was attached so tightly that it could not be released. Upon releasing this, it was not obvious that the tissue itself was separating. Therefore, utilization of a dye marking technique to watch the expansion of the suborbicularis fascia allowed access to the bony attachments of the orbicularis muscle as well as a point of placement for fat grafts injected with a fine needle tip. In most cases, only after this technique was utilized was it possible to accurately overcome the depression of the nasojugal groove.
Persing et al have described a technique they refer to as the ‘shade’ procedure which changes the contour of the orbital rim by repositioning the fat as an apron over this. This incorporates the suture into the depressed midface fat and muscle and combines the two, which creates a bulk lifting of the floor of the nasojugal crease. It relies on fixation of the fat apron with fixation of the superior quadratus and zygomaticus muscle flap to the medial and lateral orbital periosteum ( ). Codner et al have described lower lid blepharoplasty with canthal support using fat transposition. After the orbicularis muscle is released from the orbital rim origin, orbital fat from the middle and medial compartments was transposed and sutured to the periosteum. Tightening of the skin muscle flap with canthopexy improved the overall result by improving lid laxity ( ).
Fezza has described the use of hyaluronic acid to improve the volume deficiency as well as lifting the lower lid tissue by expansion with this filler. He experienced 15 patients with cicatricial ectropion who also had volume deficiencies, both of which were greatly improved using this technique. He notes that the filler can improve correction for a year or longer and is reversible with injection of hyaluronidase ( ). Bosniak et al have described the hyaluronic acid ‘push technique’ for the nasojugal groove. This involves placing a bolus of hyaluronic acid along the surface of the inferior orbital rim then using digital palpation to push and distribute the filler into the desired location. While this technique is similar to the one described by Fezza, it differs enough to be significant and is primarily used for correction of volume deficiency ( ).
Muhlbauer and Holm describe correction of baggy lower eyelids by repositioning of the herniated fat into the orbit and performing a septorrhaphy as a hernia repair. While this did not directly address the orbital rim, removing the bulge above it resulted in a smoother, more filled appearance ( ). Sachs and Bosniak described true periorbital fat herniation as the cause of baggy lower eyelids. Their surgical correction involves identification and approximation of the dehiscent orbital septum to the capsulopalpebral ligament. This technique smoothes the appearance of the lower eyelids by tightening the septum and pushing the fat back into the orbital area. ( ).
Freeman describes the SOOF lift which is a transconjunctival approach to lifting of the suborbicularis oculi fat of the upper cheek with fixation to the orbital rim. This allows filling of the nasojugal deformity with the full tissue from the rim to give a fuller and smoother contour ( ). Parsa et al describe their technique of standard blepharoplasty in one eyelid and a capsulopalpebral fascia hernia repair in the contralateral lower eyelid. Follow-ups after 6 weeks and subsequently at 6 months reveal that the fascia hernia repair was less painful during the operation and less prone to post-operative bleeding and hematoma. After this technique, the hollowing of the lower lid and the sunken appearance of the globe remained absent after 6-month follow up ( ).
Hardy et al describe a procedure for rehabilitation of the volume deficient ophthalmic or enophthalmic socket. This technique is performed using microfat grafting or lipostructure as described by Coleman. A varied volume of fat from 0.8 cc to 4.5 cc increased exophthalmometry on average up to 2 mm in these patients ( ). Kontis and Papel described rejuvenation of the aging midface including the infraorbital area. They note that past rejuvenation used fat injections or synthetic implants and emphasize their technique of elevation of the malar and infraorbital fat pads with minimal surgical incisions. They include subperiosteal, suborbicularis oculi fat lift, and arcus marginalis release with orbital fat preservation in their technique to improve the nasojugal groove ( ).
Baker describes preservation and mobilization of orbital fat to the orbital rim periosteum and notes that preservation of this intraorbital fat to the relocated position improves atrophy of aging and gives the globe a youthful appearance ( ). Camirand and colleagues advocate repositioning the intraorbital fat behind the inferior orbital rim, secured by suturing the posterior capsulopalpebral flap to the arcus marginalis to reduce and contain the herniated fat. This is enhanced with lateral canthoplasty ( ).
Wise and Greco describe the use of Restylane® and CosmoDerm® for improving nasojugal groove deformity. Although they commonly use autologous fat for the face in general, to achieve the best results in the orbital area and nasojugal groove, they prefer the use of dermal fillers ( ). Other authors including Botti et al have taken the eclectic approach in using a variety of techniques including fat grafting, rotation of fat pads to the orbital rim, Flowers implants, and midface lift for correction. All of these authors note that the best procedure may differ depending on the different deformities observed in individual patients ( , , ).
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 No touch lower blepharoplasty
No touch lower blepharoplasty
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


