Key points
- •
The infraorbital rim and adjacent midface skeleton support the lower lid and midface soft tissues.
- •
Young, attractive women have convex midface skeletons with narrow eyeball, short lower lids and full cheeks.
- •
Deficient soft tissue support intrinsic to concave midface skeletons lends itself to rounding of the palpebral fissure, lengthening of the lower lid and flattening of the cheek.
- •
Concave midfaces are predisposed to lower lid descent after conventional blepharoplasty.
- •
Alloplastic augmentation of the infraorbital rim can transform midface concavity to convexity.
Patient selection
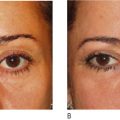
The relative prominence of the eyes impacts on the position and shape of the lower lid and therefore is an important consideration in aesthetic blepharoplasty. Eye prominence results from a deficiency in skeletal support, or less commonly, an excess of orbital soft tissue volume. Eye prominence correlates with a more inferior position of the lower lid (resulting in scleral show) and a more medial position of the lateral canthus. Descent of the lower lid increases the height of the palpebral fissure while the more medial position of the lateral canthus decreases its width. Hence, patients with poorly projecting upper midface skeletons have ‘round eyes’ when compared to the long narrow eyes characteristic of young people with a normal periorbital morphology. Furthermore, in the skeletally deficient, the lack of infraorbital rim projection and cheek prominence often allows their lower lid fat compartments to be visible giving them ‘early bags’ ( Figure 7.1 ).


Negative vector
Patients with prominent eyes, either because of maxillary hypoplasia or thyroid ophthalmopathy, have long been recognized to develop symptomatic lower lid descent (with exaggeration of their ‘round eyes’) after conventional lower blepharoplasty. Patients with prominent eyes are therefore considered morphologically prone to develop symptomatic lid malposition after lower blepharoplasty. Globe–orbital rim relationships and the tendency for the development of lower lid malposition after blepharoplasty have been categorized ( Figure. 7.2 ). In the sagittal view, a vertical line or ‘vector’ is placed along the most anterior projection of the globe. A positive vector relationship exists when the most anterior projection of the globe is posterior to the cheek prominence. A negative vector relationship exists when the most anterior projection of the globe lies anterior to the cheek prominence. Patients whose orbital morphology has a negative vector relationship are prone to lid malposition after lower blepharoplasty.
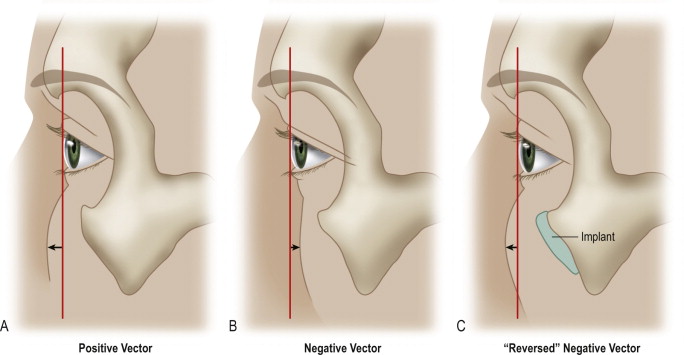
Reversing the negative vector
Augmentation of the infraorbital rim in patients with a retruded infraorbital rim can bring it into a better relationship with the globe, thereby reversing the negative vector ( Figure 7.2 ).
Reversing the negative vector
Augmentation of the infraorbital rim in patients with a retruded infraorbital rim can bring it into a better relationship with the globe, thereby reversing the negative vector ( Figure 7.2 ).
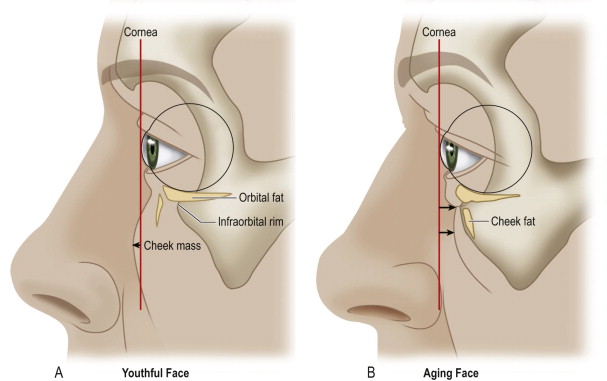
Aging
Globe–orbital rim relationship changes with age. Pessa’s group studied two groups of individuals, young and old, using three-dimensional computerized tomography. Their findings are summarized in Figure 7.3 . In the youthful face, the cheek fat lies anterior to the cornea and the orbital fat lies slightly anterior to the orbital rim. With aging, the cheek mass tends to lie posterior to the anterior surface of the cornea, the orbital fat moves slightly anterior, and the infraorbital rim has a significant movement posteriorly. Hence, retrusion of the infraorbital rim with aging will make the eyes appear more prominent by changing globe–rim relations, and it will significantly impact the appearance of the lower lid bags, particularly in those who tend toward maxillary hypoplasia.
Indications
The periorbital appearance of patients with poorly projecting infraorbital rims (morphologically prone, negative vector) can be normalized with a procedure that combines infraorbital rim augmentation, subperiosteal midface elevation, and, if necessary, lateral canthopexy. An alloplastic implant increases the sagittal projection of the infraorbital rim, effectively reversing the negative vector. The implant provides support for the cheek and lid tissues. The midface elevation repositions the descended cheek and recruits lower lid tissue. When necessary, the lateral canthopexy repositions the lateral canthus and provides additional support for the lower lid. This operation can be adapted for morphologically prone patients who are first seeking improvement in their periorbital appearance or for those whose lid malposition and round eye appearance have been exaggerated by previous lower blepharoplasty. It is adapted from experience treating the post-traumatic, Graves’ ophthalmopathy, and post-blepharoplasty lower lid retraction.
Operative technique
Pre-operative preparation
In young, healthy adults, the average projection of the cornea beyond the infraorbital rim is 3 mm. This relation is an approximate goal of augmentation. Documenting the amount of disproportion is useful for preoperative planning and postoperative evaluation, and it can be done with measurements by a Luedde exophthalmometer or with life-size photographs. A disproportion in sagittal globe–rim relations (negative vs positive vector) is usually obvious and correction is made by clinical judgment.
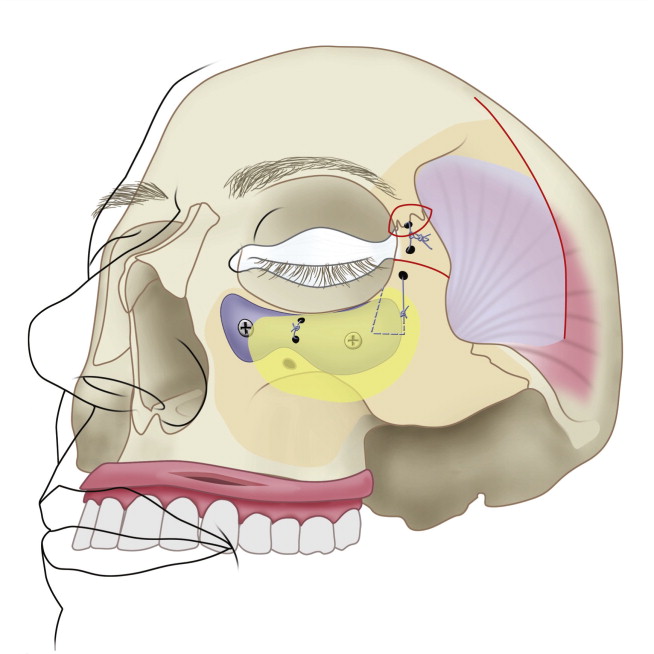
Technique
This procedure involves two, and sometimes three, basic maneuvers ( Figure 7.4 ). Augmentation of the infraorbital rim with an alloplastic implant effectively changes the facial skeletal morphology (negative to positive vector) thereby providing support for the lower lid and midface soft tissues. Subperiosteal freeing and elevation of the lower lid and midface recruits lid tissues and allows lower lid repositioning. In patients undergoing surgery to correct lid malposition after previous blepharoplasty, lateral canthopexy restores palpebral fissure shape and provides additional lower lid support.
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Midface elevation: one single suture
Midface elevation: one single suture
 No touch lower blepharoplasty
No touch lower blepharoplasty
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


