INTRODUCTION
Depending on the size and location of the targeted leg veins, any of a multitude of therapeutic options may be appropriate. While selecting the correct treatment techniques is important, management of patient expectations prior to the treatment can be equally vital. Key items should be thoroughly discussed with every prospective patient ( Box 5.1 ). The patient must understand that although improvement is expected, there is no guarantee regarding the degree of improvement. Risks accompany any medical procedure, and these must also be reviewed thoroughly. Once all necessary information is communicated, the patient should be encouraged to ask questions and should be provided with a detailed explanation of any concerns, as appropriate. If the patient appears excessively anxious, overly demanding, or simply unable to understand the procedure, then the patient may not be an ideal candidate for intervention.
Box 5.1
Topics of Pretreatment Discussion With Patient
-
•
Patient expectations
-
•
Expected discomfort during treatment
-
•
Number of treatments required
-
•
Benefits of treatment
-
•
Possible risks and complications of treatment
-
•
Treatment alternatives
-
•
Posttreatment care
-
•
Duration and nature of recovery phase
COMPRESSION
The use of external compression therapy (CT) is a fundamental strategy in the treatment of lower-extremity venous disease. Despite recent therapeutic advancements in leg vein treatment, compression remains a simple, effective, accessible, and inexpensive modality. It should be considered the primary treatment in many conditions and an adjunct when other treatments are employed ( Box 5.2 ).
Box 5.2
Indications for Leg Vein Compression
-
•
Deep vein thrombosis (DVT) prophylaxis
-
•
Active DVT treatment
-
•
Symptomatic varicose veins
-
•
Chronic venous insufficiency
-
•
Venous ulcers
-
•
Postsclerotherapy
-
•
Postphlebectomy
-
•
Postendovascular ablation
-
•
Pregnancy
-
•
Thrombophlebitis
ACTIVE AND PASSIVE COMPRESSION
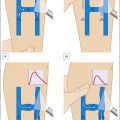
Compression can be either passive or active. Passive compression is applied using inelastic bandages. As muscles contract, the bandages resist the volume increase and thereby deliver increased pressure. As the muscles relax, the volume decreases so that minimal pressure is applied by the bandages. On the other hand, active compression using elastic bandages permits the application of pressure during both muscular exercise and at relaxation. This constant pressure may not be tolerated by bedridden or inactive patients and is generally contraindicated in those with arterial insufficiency ( Fig. 5.1 ).
( A ) Before compression. ( B ) Compression shifts the venous flow from superficial to deep system.
Whether passive or active, compression improves venous disease through several mechanisms. Compression narrows the lumens of the veins in the superficial system, which accelerates venous flow, decreases venous pooling, and helps shift venous flow from the superficial into the deep venous system. Compression also may partially restore valvular function and gradually reverse degenerative changes in the veins, thus reducing venous reflux.
COMPRESSION BANDAGES ( Tables 5.1 and 5.2 ; Fig. 5.2 )
Short-Stretch Bandages
Various modalities are available for compression. Completely rigid inelastic bandages, like the zinc gel Unna boot (Unna-Flex, Convatec, Princeton, NJ) and the Gelocast (Beiersdorf Inc., Norwalk, CT), both dry to form a cast around the leg. Short-stretch bandages such as Comprilan (Beiersdorf, Norwalk, CT) are made of fabric that stretches 30% to 50%. Inelastic bandages and short-stretch bandages exert passive compression to treat edema, DVT, or ulcerations due to chronic venous insufficiency (CVI). They must be applied by trained staff to ensure a proper fit and remain in place for several days continuously. However, as edema remits and leg circumference decreases, the inelastic nature of the bandages fails to accommodate for this change, and corresponding pressure loss can occur as early as within the first few hours of application.
Table 5.1
Manufacturers of Compression Stockings
| Brand | Location and Telephone Number | Website |
|---|---|---|
| Jobst | Charlotte, NC 1-800-537-1063 | www.jobst-usa.com |
| Sigvaris | Peachtree City, GA 1-800-481-5488 | www.sigvaris.com |
| JuZo | Cuyahoga Falls, OH 1-800-222-4999 | www.juzousa.com |
| Medi | Whitsett, NC 1-888-633-6334 | www.mediusa.com |
| Venosan | Asheboro, NC 1-800-322-7744 | www.venosanusa.com |
Table 5.2
Manufacturers of Compression Bandages
| Manufacturer | Type | Adherence/Name |
|---|---|---|
| Convatec Princeton, NJ | High stretch | Nonhesive/Tubigrip |
| Beiersdorf Norwalk, CT | Low stretch |
|
| Beiersdorf | High stretch |
|
| Beiersdorf | Nonstretch | Cohesive/Gelocast |
| 3 M Health Care St. Paul, MN | High stretch | Adhesive/Microfoam |
| Convatec Princeton, NJ | Nonstretch | Cohesive/Unna-Flex |
| Conco Medical Bridgeport, CT | Low stretch | Cohesive/Medi-Rip |
( A–C ) Proper application of stretch bandage post sclerotherapy.
Long-Stretch Bandages
Long-stretch bandages, made of fabric that can stretch 100% to 200%, provide active compression, indicated after surgery, sclerotherapy, or thrombophlebitis. Their main disadvantage is the potential hazard for patients with arterial occlusive disease. The application of bandages is dependent on the skill of the practitioner, with experienced clinicians able to consistently apply bandages with pressure ranging from 25 to 50 mm Hg. The less experienced typically achieve pressures in a broader range, from 15 to 70 mm Hg, and deviation on the high end can lead to arterial occlusion in those with preexisting arterial disease. Therefore, before application, arterial flow should be evaluated by checking the ankle/brachial index, and patients should be instructed on how to properly superimpose each successive layer. After being washed, the bandages tend to lose some of their compressive capability.
Multilayer Bandages
Multilayer bandages are a compromise between inelastic bandages and long-stretch elastic bandages. They are often comprised of four superimposing layers: (1) wool padding for comfort and to absorb exudates; (2) cotton bandage to hold the wool in place; (3) long-stretch elastic bandage for active compression; and (4) cohesive medium-stretch bandages. The different indications for the various bandage options are not absolute as the ultimate physiologic effect can be modified by the clinician applying the bandage. Comparative studies assessing the benefit of particular bandages for select indications are still inconclusive.
COMPRESSION STOCKINGS
Stockings provide an alternative to bandages. Varying in length and by degree of compression, stockings can be used for prophylaxis against DVT or development of varicose veins. Stockings are also indicated after surgery, phlebectomy, or sclerotherapy. Compression following sclerotherapy of varicose veins and larger reticular veins is a universally accepted intervention that encourages the direct apposition of the vein walls so as to decrease the likelihood of thrombus formation and subsequent recanalization of the treated vessel. The avoidance of thrombus formation also appears to limit hyperpigmentation and thrombophlebitis and subsequent telangiectatic matting. However, the utility of stockings following treatment of small telangiectasias continues to be debated. After leg surgery or phlebectomy, stockings help prevent hematomas. During pregnancy, stockings forestall the development of varicose veins that would otherwise proliferate further due to increased venous pressure and hormonal influences. Pressure stockings are also a key element in the treatment of superficial thrombophlebitis.
There are five stocking compression classes, designated 0 to IV ( Table 5.3 ). In each class, there are available various lengths, ranging from socks to thigh-high to full-length pantyhose. Proper selection is contingent on the indication and the patient’s ability to tolerate compression. Elderly patients may have difficulty putting on the stockings, especially the high-compression stockings, and devices have been developed to assist these individuals. An alternative strategy is to superimpose two pairs of compression stockings, with, for example, two pairs of Class 0 stockings offering the same pressure as one pair of Class I stockings. The two separate stockings are easier to pull on. Stockings tend to lose pressure with routine use and washing and may need to be replaced every 6 months.
Table 5.3
Classes of Compression Stockings
| Compression Class | Pressure (mm Hg) | Common Indications |
|---|---|---|
| 0 | 10–20 | Mild functional venous insufficiency |
| I | 20–30 | Chronic venous insufficiency, symptomatic varicose veins, DVT |
| II | 30–40 | Symptomatic varicose veins, DVT, venous ulcers |
| III | 40–50 | Venous ulcers |
| IV | >60 | Severe symptoms, difficult-to-control edema, significant skin fibrosis |
The classification of compression classes may vary among different countries and different brands.
DVT , Deep vein thrombosis.
Class 0 stockings are indicated in mild functional venous insufficiency that results in minimal varicose veins with associated mild edema or leg fatigue. Chronic venous insufficiency and more severely symptomatic varicose veins should be treated with either Class I or II stockings. Class I or II stockings are also indicated in the outpatient management of DVT, as they relieve pain and edema and enhance thrombus adhesion. Leg ulcer treatment requires Class II or III stockings in addition to local skin treatment. Alternatively, ulcerations may be amenable to other types of compression treatment such as multilayer bandages or inelastic bandages. Class IV is reserved for those with severe symptoms, difficult-to-control edema, and significant skin fibrosis.
There is no consensus on the duration or degree of compression needed after surgery. Although one study has shown equal efficacy between high- and low-pressure compression stockings in minimizing incidence of bruising and thrombophlebitis after varicose vein surgery, high-compression stockings are clearly necessary after sclerotherapy. However, there appears to be no difference between Class I and Class II compression stockings in controlling the objective and subjective parameters of venous insufficiency. Weiss et al. studied the duration of compression after sclerotherapy and found that subjects with the most improvement used 3 weeks of compression, followed by the group with 1 week of compression and then by the group who only used compression for 3 days. All treatment groups had significant improvement compared to the control group that did not receive compression. The 1- and 3-week groups also experienced less sclerotherapy-associated hyperpigmentation than the 3-day group and the control group.
TREATMENT OF SMALL-VESSEL DISEASE
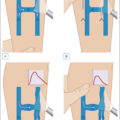
When larger truncal varicose veins are present, the associated telangiectasias cannot be successfully treated without addressing the underlying hydrostatic pressure elevation. In cases of great saphenous vein (GSV) incompetence, surgical techniques or endovenous ablative techniques may be required. Ambulatory phlebectomy allows for the treatment of virtually all large varicose veins, while sclerotherapy can be used to treat large varicose veins and reticular varicose veins. Only after the reticular, varicose, and deep incompetent veins have been treated should attention turn to treating the superficial telangiectasias with sclerotherapy or with laser- or light-based devices. In patients with only isolated telangiectasias without pressure problems in larger vessels, sclerotherapy or laser/light therapy may be used primarily ( Fig. 5.3 ).
( A ) Visualization of the leg vein. ( B ) Two-point counterpressure applied to the injection site. ( C ) Placement of the needle into the vein at 30 degrees. ( D ) Steady injection producing immediate blanching of vessel. ( E ) Immediate application of cotton ball and tape.
Sclerotherapy
The goal of sclerotherapy is to intravascularly infuse a chemical irritant to cause irreversible endothelial cellular destruction, which leads to vascular fibrosis and obliteration. Virtually any foreign substance can be utilized to induce venous endothelial damage, and several sclerosing solutions are commercially available for this purpose ( Table 5.4 ). The selection of solution type, concentration, and quantity is dictated by the type and site of the varicosity ( Fig. 5.4 ).
Table 5.4
Common Sclerosing Agents
| Solution | Category | Advantages | Disadvantages | Brands |
|---|---|---|---|---|
| Sodium tetradecyl sulfate | Detergent | Painful only with extravasation; capable of sclerosing larger veins; FDA approved | Necrosis if extravasation with >0.25% solution; pigmentation, matting | Sotradecol (Angiodynamics, Quensbury, NY) Fibrovein (STD Pharmaceuticals Inc., Hereford, UK) |
| Polidocanol | Detergent | Painless; rare necrosis; FDA approved | Urticaria at injection site; no pain to warn of arteriolar injection |
|
| Hypertonic saline | Hyperosmolar solution | Nonallergenic | FDA: off-label; painful injections, necrosis, pigmentation, matting | None |
| Glycerin | Toxin | Rare matting, pigmentation, necrosis | Too weak for large veins; more viscous; possible allergy; FDA off-label | Scleremo (Lab Therica, France) |
Sclerotherapy tray consisting of rubbing alcohol, needles and syringes, various sclerosants (shown here: 72% glycerin, 0.5% sodium tetradecyl sulfate, 0.2% sodium tetradecyl sulfate, and 0.1% sodium tetradecyl sulfate), compression bandage, three-way stopcock, gauze, and tape. Not shown are cotton balls.
Postsclerotherapy Compression
To decrease the incidence of thrombus formation, which may lead to subsequent recanalization and postsclerosis pigmentation, compression is also an essential adjunct to sclerotherapy of large varicose veins. Moreover, direct apposition of vein walls due to external compression increases the duration of sclerosant contact with the endothelium, thus making the procedure more effective. Finally, the reduced thrombotic and subsequent inflammatory phlebitic events may also minimize telangiectatic matting. Some authors argue that telangiectasias <1 mm require no compression after injection, but there is general agreement that sclerotherapy of larger telangiectasias, venulectasia, reticular veins, and varicose veins must be followed by several days of compression therapy. During sclerotherapy, elastic bandages are commonly applied immediately after the last sclerosant injections. Cotton balls or rubber cushions may be placed under these bandages to provide additional pressure at points of reflux or over larger veins to prevent thrombosis. Since bandages gradually lose the compressive force as they become loosened with patient movement, many clinicians prefer compression stockings after sclerotherapy, or they will advise patients to replace bandages with stockings a few hours after the procedure.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


