• The evolution of techniques in reconstructive maxillofacial surgery has led to safe and efficacious surgery of the facial soft tissue, the natural extension of which was surgery purely to enhance the appearance.
• The soft tissue overlying the bone defines the contour and appearance of the face, whereas the bony foundation provides attachment and support to the soft tissue.
• This interdependent relationship serves as a scaffold from which techniques of aesthetic facial surgery evolved.
• Every tissue layer should be assessed to determine the appropriate intervention to achieve a desired result.
Introduction
Aesthetic facial skeletal surgery has become one of the most popular and demanding fields of surgery today. With the technologic advancements and the development of surgical techniques, it is possible to not only make an abnormal face more normal but also modify the normal face to create a supranormal or aesthetically enhanced face. A key concept, however, makes this field quite challenging. The human face is composed of different components and building blocks; therefore any attempt to alter facial features must consider establishing or reestablishing harmony among the components, rather than making isolated alterations. In other words, aesthetic enhancement often involves form, whereas certain alterations must consider the functional elements as well. Orthognathic surgery, for instance, although used to create the ultimate aesthetic face, requires the consideration of functional elements to create osteotomies and stable fixations in addition to the critical soft tissue projections determining the aesthetic outcome. Moreover, the facial form is recognized as a summation, contributed to by both the skeletal foundation and the overlying soft tissue. Due to the challenges mentioned, facial aesthetic surgery necessitates not only a deep and profound knowledge of normal aesthetic relations and physical anthropologic values but also an understanding of patient values and expectations often influenced by gender, cultural, societal, and psychologic factors.
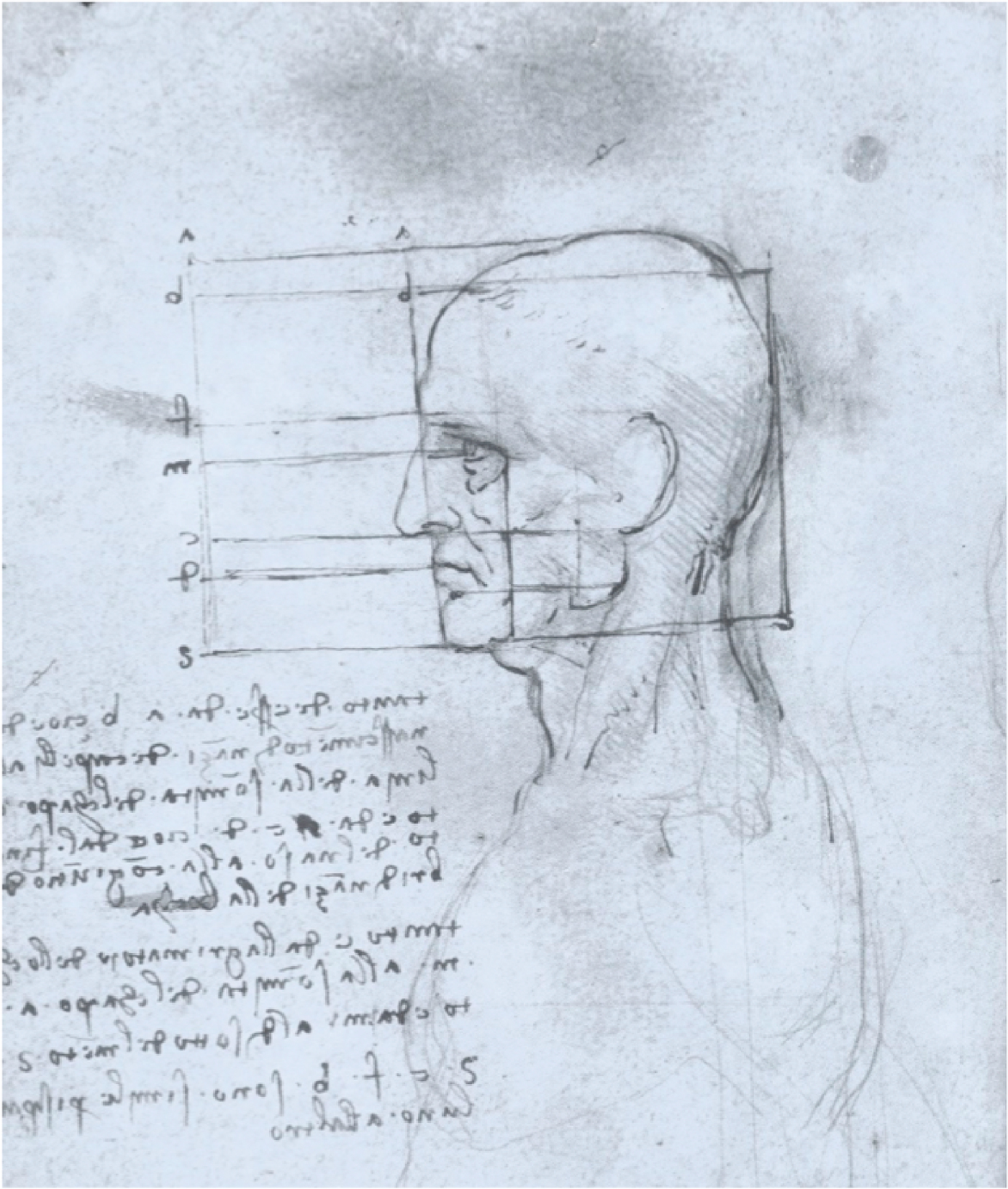
Webster’s unabridged dictionary defines beauty as “the quality which makes an object seem pleasing or satisfying in a certain way.” For instance, the golden ratio, first described by Euclid, is said to be an important feature, found in many classically appealing and harmonious architectural structures, objects, and many natural phenomena. The aesthetics of the human face also falls within the principles mentioned before. Simply put, attractive faces, across different cultures, whether in drawings or in reality, feature certain proportions that create a full and harmonious appearance, which is appealing to the eye. Leonardo da Vinci, for instance, confirmed the presence of the golden ratio in the human face in the sketch shown in Fig. 1.1 . Since ancient times, many artists, scientists, and surgeons have attempted to quantify beauty to propose guidelines for facial alterations. , However, there is no one universal formula that defines beauty. On the other end of the spectrum, certain facial features, such as asymmetry, tissue excess, or deficiencies, to mention a few, are considered unattractive by many.
Evolution of thought and technique
Due to the central positioning, the plane of projection, and the rather soft cartilaginous foundation, the nose is considered the key element in defining beauty to oneself and others. As a result, nasal injuries or deformities are readily detectable in the face and could result in serious self-image issues and social limitations besides functional limitations. Since ancient times, the nose has been viewed as the “organ of reputation,” and rhinokopia, or nasal amputation, was previously used as a punishment to humiliate individuals for the crimes they committed. Due to their high prevalence and the highly noticeable features, nasal injuries and deformities, therefore, received extensive attention with regard to reconstruction throughout the ages. The Edwin Smith Surgical papyrus, dated circa 3000 BC, is an ancient document describing 48 surgical case reports. Among the procedures described, there is what seems to be the first detailed description of the treatment of nasal fractures by manipulation of the nasal bones and cartilage. Total nasal reconstruction can be traced back to the Sanskrit texts of ancient India. During the sixth century BC, Indian potters developed techniques to harvest skin from the forehead and cheeks to reconstruct the nose. Although the exact timeline is not known, pedicled tissue transfer took the place of skin grafts to correct larger defects involving the soft tissue surrounding the nose as well. By the nineteenth century, techniques in rhinoplasty had improved dramatically. In his famous work Rhinoplastik, which was published in 1818, Carl Ferdinand Von Graefe described three different surgeries in nasal reconstruction: the Indian technique with the forehead flap used to correct nasal defects; the delayed Italian flap, a technique formulated by Tagliacozzi; and the German method, which entailed a graft harvested from the arm to reconstruct the nose. The first nasal reconstruction in the United States was performed by Dr. J. M. Warren in Boston in the late 1830s. The discovery of local anesthetics, the vasoconstrictive properties of cocaine, and the antiseptic qualities of phenol further facilitated performance of such procedures as more and more patients were undergoing such corrective surgeries. In fact, it was in 1887 that Dr. John Orlando Roe published an article describing the first purely aesthetic rhinoplasty using an internal approach to correct a “pug nose,” which is described as a deformity caused by large lower lateral cartilages with or without a dorsum concavity. Therefore nasal reconstruction served as a gateway to understanding the challenges and interplay of soft and hard tissues in aesthetic facial skeletal surgery.
The late nineteenth century is considered a revolutionary period in the history of American facial plastic and reconstructive surgery. As techniques in rhinoplasty improved, attention was directed to other components of the face. In 1881, while a staff member of the Manhattan Eye, Ear, and Throat Hospital in New York, Robert Talbott Ely performed an otoplasty on a 12-year-old boy with protruding ears. After such landmark interventions, such as Ely’s otoplasty, more and more surgeons felt comfortable modifying facial structures with cartilaginous foundations and rather thin overlying skin. Furthermore, injuries that resulted during World War I challenged many surgeons to push the limits and develop new techniques in an attempt to correct facial deformities caused by injuries. In addition to soft tissue modification and transfer techniques, many injuries required restoration of bony structure with bone grafts from other sites of the body.
Parallel to the development of techniques in restoration, alteration, or enhancement of the soft tissue structures of the face, five major concepts were developed, allowing restoration and modification of the facial components:
- 1.
Autogenous bone grafting for augmentation or enhancing existing structures
- 2.
Osteotomies to move the positions of bone in three-dimensional space
- 3.
Alloplastic implants and injectable fillers
- 4.
Skeletal contour reduction procedures
- 5.
Understanding of the soft and hard tissue relationships
Autogenous bone grafts and allogeneic bone substitutes
During this era, Dr. Paul Tessier, among other surgeons, developed and described techniques and instruments for the purpose of harvesting of (1) iliac, (2) costal, (3) tibial, and (4) calvarial autogenous bone grafts. Tessier further characterized craniofacial defects and the approaches required for restoration. He correctly identified that the borders of craniofacial defects associated with agenesis are not normal bone due to the lack of periosteum and, thus, required freshening of the edges to reach bleeding bone that had better healing potential. Furthermore, as techniques in alterations of the midface and the upper face developed, he soon recognized that autogenous bone grafts can be used not only to alter facial contour but also to restore defects in terms of volume, provide resistance to masticatory forces, and reestablish the buttress system in the face. Later on, such techniques were further developed for purely aesthetic purposes to enhance the bony prominences of the face, notably the supraorbital temporal ridge, malar–midface, and mandible–chin. However, early bone substitutes, although successful in reestablishing or modifying facial contour, failed to reestablish the structural integrity needed to resist the functional forces in the face. Autogenous bone grafting techniques, although effective, could not, however, be used to correct larger defects because revascularization and blood supply limited the healing potential of such defects.
Osteotomy techniques and procedures
An 1858 article by Norman W. Kingsley is considered the first formal report on dentofacial principles and facial aesthetics. Kingsley analyzed the subunits of the face and recognized the relationship between the maxilla and the mandible and the problems associated with the discrepancies associated with the two. He further recognized the importance of the ocular region, stating “the eye soon tires of the stiffness and formality of unbroken uniformity, and is only permanently pleased with the beauty which comes from graceful variation.” Further work by Edward H. Angle in the classification of occlusion and the invention of the cephalometer by Holly Broadbent in 1931 were two milestones facilitating evaluation of the facial skeleton and association with dentofacial deformities.
Circling back to 1849, Simon Hullihen described a procedure that is considered the first anterior mandibular “set back” osteotomy for the treatment of prognathism. Almost 5 decades later, on December 19, 1897, Vilray Blair, one of the pioneers of plastic and reconstructive surgery, described a procedure to treat asymmetrical mandibular prognathism to correct anterior open bite; the procedure was a modification of Hullihen’s original procedure. Through his procedure, he performed osteotomies that allowed for rotation of the mandible, closure of the open bite, and mandibular set back to modify the lower face quite effectively after application of maxillomandibular fixation and healing.
Even though David Williams Cheever reported the first LeFort I osteotomy designed to expose and remove a nasopharyngeal polyp, it was Hugo Obwegeser who described the total horizontal LeFort I osteotomy with complete down fracture to mobilize the maxilla for midface modifications, the intraoral sagittal split osteotomy of the mandibular ramus, and a simultaneous procedure to modify the mid- and lower face. The animal studies completed at the laboratory of William H. Bell further provided biologic evidence regarding the osteosynthesis basis of these procedures, and with the development of compression plating by Hans Luhr, the long-term stability and healing potential of these procedures significantly improved. With the correction of facial deformities by using osteotomies and major bony movements, the new and harmonious face not only had better functional outcomes but also appeared more aesthetically pleasing. In the lower face, improved tooth–lip relationship provided a more aesthetic smile while minimizing the appearance of a “gummy” smile.
The work of Harold Gillies, one of the founders of modern plastic and reconstructive surgery in terms of soft tissue rearrangement, and further work by Dr. Paul Louis Tessier, who used a transcranial approach to modify orbits via the anterior skull base, were two key steps in the advancement of facial skeletal surgery and techniques in orthognathic surgery. Through his treatment of congenital and posttraumatic anomalies, Tessier developed effective techniques that allowed him to safely and effectively modify the upper face.
Considering the challenges posed by prosthetic implants, Hugo Obwegeser, in 1957, attempted to surgically correct micrognathia by using an intraoral approach with transoral sliding osseous genioplasty. Using this technique, Obwegeser performed a transverse osteotomy, which allowed advancement of the anterior bony segment while maintaining the geniohyoid muscle pedicle. The “Obwegeser technique” gained popularity due to its more reliable results; however, many patients found the procedure rather aggressive and traumatic, and the search for a more friendly and reliable grafting material continued.
Synthetic implants and injectables
In addition to rhinoplasty, blepharoplasty, and otoplasty, patients were pursuing additional surgical solutions to enhance beauty. Among the available options, malar augmentation and genioplasty grew in popularity due to the rather effective transformations. Due to the limitations of autologous grafting, such as resorption, distortion, limited availability, and donor site morbidity, synthetic implants became more popular. Although certain metallic implants had been used due to their inert nature and low toxicity, they were soon replaced by softer, more biocompatible alternatives. Among the available options, acrylic resin was found to be biocompatible and easy to use. Following the use of acrylic resin, however, many surgeons noted the wear and tear and failure of this material with time. The next major advancement was the introduction of silicone elastomers in the 1960s, which provided a rather inert and stable biofriendly material.
The development of prosthetic materials and implants drastically changed plastic and reconstructive surgery. Expanded polytetrafluoroethylene, polydimethylsiloxane, polyester fiber, polyamide mesh, high-density polyethylene, and polymethylmethacrylate implants are only a few popular examples. However, some of the synthetic materials, although biocompatible, were not long-lasting and showed signs of deformation. Soon surgeons realized the potential shortcomings of alloplastic implants, such as susceptibility to infection, capsule formation, and resorption of underlying bone, all of which dramatically reduced the aesthetic outcomes. Considering such shortcomings, dermal fillers that are both temporary and permanent were introduced. Hyaluronic acid, calcium phosphate, and polylactate fillers have gained popularity as “injectables” and have supplanted collagen. Because many of these substances occur naturally in the body, they are less immunogenic and offer a minimally invasive solution for restoration of soft tissue contour and reversal of aging features, such as wrinkles. However, despite satisfactory results, many of these fillers are not permanent and require continued periodic injections to maintain optimal form.
Circling back to the end of the nineteenth century, Gustav A. Nueber (1850–1932) used fat harvested from the patient’s arm to transplant and correct an inferior orbital soft tissue defect cause by osteomyelitis. However, despite the rather simple technique, this procedure did not gain popularity due to the significant volume loss after transplantation and scar formation, especially in the face. It was not until the 1980s that techniques involving liposuction were developed, and autologous fat grafting and injections to augment soft tissue gained enormous popularity. As more surgeons utilized liposuction, the technique was developed to a more sophisticated, atraumatic procedure, and finally in the 1990s, with the principles developed by Sidney Coleman, the survival rate of the grafted material increased significantly. Coleman believed that the key to increasing the longevity of the fat graft was to (1) use low negative pressure to harvest fat, (2) use centrifugation to purify the harvested material, and (3) increase the surface area of contact between adipocytes and the accepting tissue by using multiple tunnels and minimal adipocytes.
Contour reductive procedures
Many individuals pursue aesthetic facial surgery to produce a “stronger” chin, more fullness of the angles of the mandible, higher cheek bones, or pronounced supraorbital areas. These alterations often require augmentation for facial rejuvenation, with or without soft tissue procedures, and to reverse bony changes and thinning and expansion of the soft tissue envelope. However, the same highlight areas of the face can be reduced to provide “softer” facial features. Shaving of the supraorbital ridges and the glabella, zygomatic arch reduction, reduction genioplasty, and softening of the mandibular angles have become more common in Asian cultures in the past decade, with the goal of narrowing the face and producing “softer” features. However, despite such cultural trends, each individual may find one set of features more desirable as opposed to others, depending on personal values influenced by sexual orientation and gender identity. Therefore what constitutes facial feminization or facial masculinization plays an integral role in a patient’s future in terms of the challenges posed by society in terms of sexuality and gender identity. This has been a pivotal point in the evolution of facial aesthetic surgery, allowing surgeons and many patients to achieve what was not possible previously.
Soft and hard tissue relationship
With modifications of abnormal faces using hard tissue modification to improve form and function, surgeons not only created normal faces but also discovered the concept of improving normal faces to supranormal by optimizing soft and hard tissue relationships. Procedures such as orthognathic surgery, which were developed to correct malocclusion and other functional deficits, yielded more aesthetic outcomes, such as optimal tooth–lip relationship and nasal projection. Midface augmentation procedures with canthopexy further showed the enhancing effects of resuspension of the lateral canthus to a superior position in relation to the medial canthus, which had dramatic effects on facial aesthetics. As a result, a new aesthetic philosophy of surgery—where the relationship of the soft tissue in reference to hard tissue was modified with the sole purpose of enhancing aesthetics and beauty—was born. The first rhytidectomy, for instance, was reportedly performed by Eugen Holländer in Berlin in 1901, for an elderly female aristocrat who asked the surgeon to “lift her cheeks and corners of the mouth” for a more youthful appearance; this was achieved by excising an elliptical piece of skin around the ears. Considering this new philosophy, standards of facial aesthetics were developed and guided many surgeons to perform procedures focusing on enhancing beauty. It was further noted that in the upper face, soft tissue thickness is rather uniform, showing a slight increase in thickness inferiorly, resulting in the greatest thickness in the supraorbital rim region. In the midface, soft tissue is thin directly inferior to the orbit, thickening progressively toward the body of the zygoma and thinning again over the zygomatic arch. Of note, moving from superior to inferior in the malar midface region, the soft tissue depth increases. In the chin area, increasing soft tissue thickness is seen moving from the chin–lip fold to the mental eminence with a decrease in thickness directly beneath the chin. The soft tissues over the angle of mandible, considered the thickest in the face, are heavier over the anterior ramus and occlusal areas of the maxilla and the mandible than in the gonion region.
Facial analysis with gender considerations
Historically, many artists, scientists, and surgeons have attempted to quantify beauty to propose guidelines for facial alterations. For instance, in his work on anthropometrics, Farkas , , showed that the facial measurements devised by Renaissance scholars, although appealing, may not accurately represent the facial features present in the population. However, such proportions and the more recent analysis of facial proportions described in the surgical and orthognathic literature remain the general guidelines used in examination of the face.
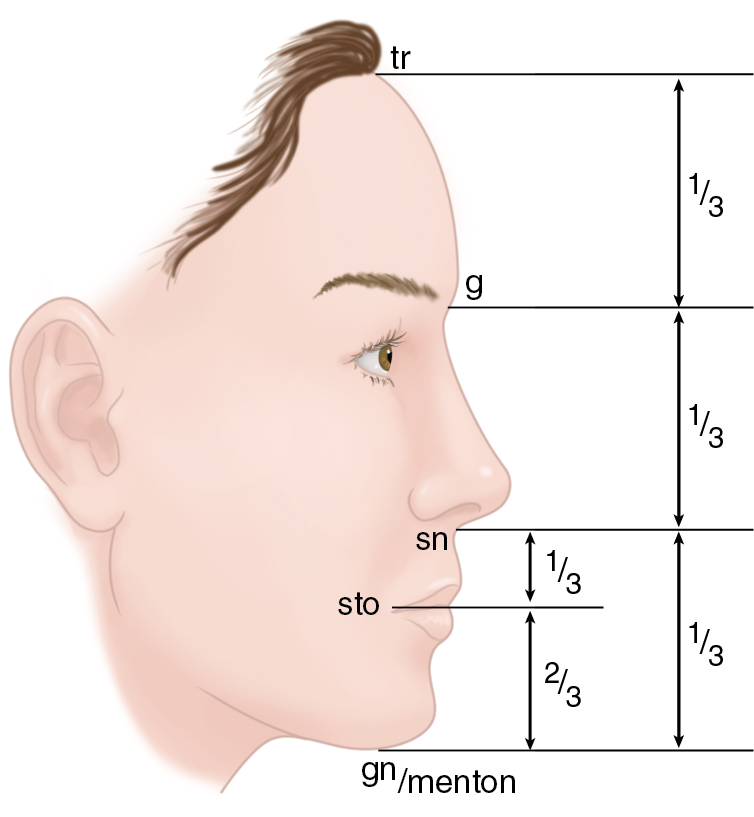
Facial analysis and therefore preoperative planning may start by analysis of facial symmetry, height, and width as shown in Fig. 1.2 . Although some variation is considered normal, facial height can be divided into three equal segments, otherwise known as horizontal thirds: upper face, measured from the trichion (hairline) to the glabella; middle face, measured from the glabella to the subnasale; and the lower face, measured from the subnasale to the gnathion or the menton. Ideally in the lower third, the distance from the subnasale to the stomodeum is roughly one third of the lower third height, whereas the distance from the stomodeum to the menton is two third of the total lower thirds height. In reality, the most frequent variation is the lower third height being slightly greater than the upper third height, both of which are virtually always greater than the midface height. In terms of facial width, according to Farkas et al, the nose width equals the eye fissure length and the interocular diameter. Further, the mouth is 1.5 times the width of the soft nose, the face four times the width of the soft nose, and the head five times the interocular diameter, whereas the nose and the ear ideally are equal in inclination and size. Transversely the widest portion of the face is through the malar midface complex, with the bitemporal and bigonial widths roughly equal to and 10% less than bizygomatic distances as shown in Fig. 1.3 . However, from the profile view, a line drawn perpendicularly from the glabella in the head held in Frankfurt horizontal position ideally passes through the subnasale and nearly intersects the anterior projection of the chin, as shown in Fig. 1.4 .