Abstract
Tumors composed of keratinocytes, both premalignant and malignant, account for significant morbidity and some mortality. Primary and secondary prevention efforts, from public health awareness campaigns and improved protection against UVR-induced skin damage to screening of high-risk individuals, can have a positive impact.
Key elements of clinical care include: (1) identification of patients at increased risk for the development of actinic keratoses (AKs), basal cell carcinomas (BCCs), and squamous cell carcinomas (SCCs) who require screening; (2) recognition of the clinical features, including dermoscopic ones, of early skin cancer; (3) knowledge of appropriate biopsy techniques and the histopathology of cutaneous carcinomas; and (4) counseling regarding changes in behavior that lead to a reduction in exposure to UVR. Once the diagnosis is established, treatment options vary from observation to field treatments in the case of AKs and destruction to surgical excision with margin control for BCCs and SCCs. More recently, oral medications for advanced or metastatic BCCs have been introduced that take advantage of insights into signal transduction pathways.
Keywords
keratinocyte carcinoma, skin cancer, actinic keratosis, basal cell carcinoma, superficial basal cell carcinoma, nodular basal cell carcinoma, morpheaform basal cell carcinoma, fibroepithelial basal cell carcinoma, squamous cell carcinoma, Bowen disease, non-melanoma skin cancer, verrucous carcinoma, keratoacanthoma, 5-fluorouracil, imiquimod, pigmented actinic keratosis, vismodegib, sonidegib, basal cell nevus syndrome, basosquamous carcinoma
▪ Solar keratosis and senile keratosis are non-preferred synonyms for actinic keratosis (solar keratosis is abbreviated to SK, causing confusion with seborrheic keratosis) ▪ Bowen disease: squamous cell carcinoma in situ , intraepidermal carcinoma ▪ Basal cell epithelioma and rodent ulcer are antiquated synonyms for basal cell carcinoma ▪ Basal cell nevus syndrome: nevoid basal cell carcinoma syndrome, Gorlin syndrome, Gorlin–Goltz syndrome
- ▪
Keratinocyte carcinoma, also referred to as non-melanoma skin cancer (NMSC), represents the most common malignancy among Caucasians
- ▪
The major risk factor for BCCs and SCCs is exposure to UVR; other factors include exposure to ionizing radiation, arsenic or organic chemicals, human papilloma virus infection, immunosuppression, and genetic predisposition
- ▪
Prevention efforts are aimed at lowering incidence and morbidity via educational programs and sun protection campaigns
- ▪
If neglected or inappropriately managed, skin cancer can cause significant morbidity and even death
- ▪
Surgery remains a mainstay of treatment, but additional modalities include topical chemotherapy and immunomodulators, photodynamic therapy, and drugs that address genetic defects
Introduction
Keratinocyte carcinomas, specifically basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), represent the most frequently observed malignancy among Caucasians. In individuals with fair skin, approximately 75–80% of these malignancies are BCCs and up to 25% are SCCs . The incidence of both continues to rise, leading to an increasing burden of disease.
History
In 1775, Sir Percivall Pott noted an etiologic relationship between SCC and chimney soot exposure in his short treatise Chirurgical Observations Relative to the Cancer of the Scrotum . During the Industrial Revolution, links to arsenic, coal tar, shale oil, and creosote were also identified. In the late 1800s, Paul Unna noted a connection to UVR, when he described skin cancer development in chronically sun-exposed sites in sailors.
Evidence of the basal cell nevus syndrome (BCNS), consisting of jaw cysts, syndactyly and bifid ribs, has been identified in Egyptian mummies almost 4000 years old. In the 1850s, Lebert first used the term “rodent ulcer” to describe untreated BCCs of long duration. Several years later, Sir Jonathan Hutchinson published a review of 42 cases of BCCs, identifying the tumor as a single entity with many different clinical and histopathologic forms. Krompecher first suggested that a BCC arose from the cells of the basal layer of the epidermis, but there were additional theories regarding the site of origin of this tumor, including from the hair follicle and other adnexal structures.
Epidemiology
Keratinocyte carcinomas occur worldwide in all races. It is estimated that ~5.5 million occurred in ~3.3 million individuals in the US in 2012 . There are more skin cancers in the US population than there are all other cancers combined and it is estimated that one in five Americans will develop skin cancer during their lifetime (over 95% will be NMSC).
The most important factor related to development of these neoplasms appears to be skin phenotype ( Table 108.1 ) , but other factors also play a significant role. As an example, the incidence is about ten times higher in white versus Hispanic men and five times higher in white versus Hispanic women .
| INFLUENCE OF SKIN COLOR ON EPIDEMIOLOGY OF NMSC AND CUTANEOUS MELANOMA | ||
|---|---|---|
| Characteristic | Lightly pigmented individuals | Darkly pigmented individuals |
| NMSC – annual incidence per 100 000 | 230 | 3.4 |
| BCC : SCC ratio | 4 : 1 | 1.1 : 1 |
| BCC male : female ratio | 1.5 : 1 | 1.3 : 1 |
| SCC male : female ratio | 2 : 1 to 5 : 1 | 1.3 : 1 |
| % of SCCs developing in scars and chronic non-healing ulcers | <2 | 30–40 |
| NMSC incidence rates | Increasing | ? |
| NMSC mortality rates | Decreasing | Decreasing |
| Melanoma – annual incidence per 100 000) | 29 | 1 |
| Deaths due to melanoma – annual incidence per 100 000 | 4.3 | 0.2 |
The exact incidence of BCCs and SCCs may be difficult to determine due to issues such as diagnostic accuracy and diagnostic criteria (e.g. differentiation between actinic keratoses and SCC in situ ). In addition, deriving precise data is hampered by the fact that these neoplasms are not routinely included in state cancer registries and they are often treated in private offices.
The average amount of annual UVR correlates with the incidence of skin cancer. There is also a direct relationship between the incidence and latitude, in that the closer individuals are to the equator, the greater their exposure to UVR. In Australia, in 2002, the cumulative risk by age 70 years of having at least one BCC or SCC was 70% for men and 58% for women. Incidence also increases with age, with a sharp increase in BCCs in men after the age of 60 years. In those under 40 years of age, the majority of NMSC is found in women, but, by age 80, the incidence in men exceeds that in women by a 2–3 : 1 ratio .
Actinic keratoses (AKs) are most often found in fair-skinned individuals, but can be seen in all races. AKs are so common that it has been estimated that currently up to 12% of individuals in the US have them . Over 80% of AKs occur in sites with the most cumulative sun exposure, e.g. the bald scalp, superior helices of the ears, face, dorsal hands, extensor forearms. Risk factors include skin phototypes I and II, significant cumulative sun exposure, a prior history of AKs, increasing age, immunosuppression, and male gender . AKs are also markers for an increased risk of developing invasive SCC , but the rates of transformation are low and difficult to assess (see below) .
The demographics of SCC are similar to those of AKs, with the majority of SCC occurring on the head, neck, upper extremities , or shins. In light-skinned populations, the degree of UV exposure is related to SCC development while chronic irritation or injury can play a role in all populations. SCC is found more frequently in men (3 : 1 male : female) and the incidence increases significantly after age 60 years . The incidence of SCC has been rising worldwide in all age groups over the last several decades at an estimated 3–10% per year, with >400 000 cases of invasive SCC diagnosed annually in the US . Similar incidence trends have been noted worldwide.
Weinstock reported an age-adjusted mortality rate for confirmed cases of SCC in Rhode Island of 0.26/100 000. SCC-associated mortality is higher in whites and older persons, and men have a 3 : 1 greater SCC mortality rate as compared with women . SCCs located on the ear, lip and genitalia appear to have a higher risk of death. While melanoma among whites is responsible for 90% of skin cancer deaths before 50 years of age, in adults over 85 years of age, the majority of skin cancer deaths are attributable to SCC .
BCC is the most common skin cancer in humans, and men generally have higher rates of BCC than do women (1.5–2 : 1) . Over the last 30 years, it is estimated that incidence rates have risen between 20% and 80%. In the US, a disproportionate increase has been observed in young women. Similar increases in incidence rates have been noted worldwide, with the incidence doubling in Finland and Switzerland and increasing in Wales by 50% over the past two decades.
Incidence rates for BCC also increase with age and the median age at diagnosis is 68 years. In 2002, an incidence rate for BCC of 884 per 100 000 per year was observed in Australia; if documented trends in overall rates of keratinocyte cancer are applied to this figure, the annual incidence rate in 2011 would be 1850 cases of BCC per 100 000 . In this geographic location, SCC typically occurs at half the rate of BCC among men and at about one-third the rate among women.
Mortality from BCC is quite rare and occurs primarily in immunocompromised patients and individuals with BCNS. Cases of metastatic BCC are more likely from tumors with aggressive histopathologic patterns (morpheaform, infiltrating, metatypical, basosquamous). Perineural growth, also referred to as perineural invasion, may be an indicator of aggressive disease . Metastases often involve regional lymph nodes, lungs, bone, and skin. The mean age at the time of death is higher than with SCC, and the age-adjusted mortality rate for BCC has been estimated at 0.12 per 100 000. Mortality risk is related to increasing age, Caucasian race, and male gender (>2× compared with women).
Pathogenesis
See Chapter 107 .
Risk Factors ( Table 108.2 )
Environmental Exposures
Ultraviolet radiation
UV exposure is the predominant cause of BCC and cutaneous SCC as evidenced by migrant studies, the correlation of incidence to latitude, and animal studies. There is, however, a difference in the type of UV exposure (see Table 108.2 ). For BCCs, intermittent intense episodes of UV exposure and sunburns at any age appear to increase risk, whereas cumulative long-term UV exposure and childhood sunburns increase the risk for developing SCCs and AKs .
| RISK FACTORS FOR THE DEVELOPMENT OF BASAL CELL CARCINOMAS (BCCs) AND SQUAMOUS CELL CARCINOMAS (SCCs) | ||
|---|---|---|
| SCC | BCC | |
| Environmental exposures | ||
| UV exposure | + | + |
| Other exposures to UV light (PUVA, tanning beds) | + | + |
| Ionizing radiation | + | + |
| Chemicals, including arsenic, mineral oil, coal tar, soot, mechlorethamine (nitrogen mustard), polychlorinated biphenyls, 4,4′ bipyridyl, psoralen (plus UVA) | + | + |
| Human papillomavirus (HPV) | + | (+) |
| Cigarette smoking | + | |
| Pigmentary phenotype | ||
| Fair skin, always burns, never tans | + | + |
| Freckling | + | + |
| Red hair | + | + |
| Genetic syndromes | ||
| Xeroderma pigmentosum | + | + |
| Oculocutaneous albinism | + | + |
| Epidermodysplasia verruciformis | + | (+) |
| Dystrophic epidermolysis bullosa (primarily recessive) | + | |
| Ferguson–Smith syndrome | + | |
| Muir–Torre syndrome | + * | + * |
| Basal cell nevus syndrome | + | |
| Bazex–Dupré–Christol and Rombo syndromes | + | |
| Predisposing clinical settings | ||
| Chronic non-healing wounds | + | |
| Longstanding discoid lupus erythematosus, lichen planus (erosive), or lichen sclerosus | + | |
| Porokeratosis (especially linear) | + | |
| Nevus sebaceus | + | + † |
| Immunosuppression | ||
| Organ transplantation | + | + |
| Other (e.g. chronic lymphocytic leukemia treated with fludarabine, AIDS patients with HPV infection) | + | (+) |
* Both SCCs (keratoacanthoma type) and BCCs typically have sebaceous differentiation.
Sun exposure early in life appears to have a greater influence on subsequent skin cancer risk than at a later age. For example, individuals born in countries with high ambient UV radiation such as Australia have significantly higher incidence rates of BCC and SCC as compared to those with a similar genetic background (e.g. British, northern Europeans) who migrated to these locales later in life from countries with lower ambient UV radiation .
Indoor tanning usage
Several studies have demonstrated an increased risk for the development of BCCs and SCCs in those who are exposed to artificial sources of UV radiation. Intentional tanning has been shown to increase the risk of SCC development and Karagas et al. demonstrated that any use of tanning devices was associated with odds ratios of 2.5 for SCC and 1.5 for BCC, even after adjustment for history of sunburns, sunbathing, and sun exposure. In response to these findings, many countries have passed legislation aimed at regulating indoor tanning facilities, including banning minors. Notably, Australia has actually completely banned this commercial industry .
Therapeutic UVR exposure
Individuals with psoriasis have been shown to be at increased risk for the development of keratinocyte carcinomas. While long-term follow-up of psoriasis patients who underwent UVR plus tar (Goeckerman) therapy found no increased risk, long-term PUVA therapy was associated with a significant, dose-related risk of SCC development (adjusted relative risk = 8.6 for an accumulated exposure of between 100 and 337 treatments) . With prolonged therapy, a slightly increased risk for BCC development was noted as well. In addition to the direct effects of PUVA, PUVA-induced immunosuppression may also play a role.
Ionizing radiation
Exposure to ionizing radiation leads to a threefold increased risk for BCC and SCC . The risk is in proportion to the radiation dose. Larger fractionated doses (>12–15 Gy) are thought to be necessary to induce tumor formation, so the risk with a given total dose may be less if a larger number of smaller fractionated doses are given. Most SCCs and BCCs that arise after exposure to ionizing radiation do so after a long latency period of up to several decades, with most tumors appearing ~20 years after the initial exposure.
Treatment of tinea capitis with radiation (prior to the discovery of effective systemic antifungal medications) has been linked to the development of multiple BCCs. In a study of 2224 children given X-ray therapy for tinea capitis (compared with a control group of 1380 tinea capitis patients given only topical medications), the relative risk for developing BCC of the head and neck among irradiated Caucasians was 3.6 .
Patients with BCNS are exquisitely sensitive to ionizing radiation and it should be avoided if possible (see below).
Occupational risk factors
Persons with outdoor occupations have a higher risk of developing skin cancer. Airline pilots, who are exposed to ionizing radiation at flight altitudes, have been shown to have an elevated risk for both BCC and SCC . Other occupations associated with an increased risk for NMSC include agricultural workers, sailors, locomotive engineers, and textile workers.
Chemical exposures
Multiple organic chemicals have been associated with an increased risk for the development of keratinocyte carcinomas (see Table 108.2 ). Occupational chemical exposures which can lead to skin cancer most commonly involve pesticides, asphalt, tar, and polycyclic aromatic hydrocarbons, and they typically result in SCC. The skin cancers induced by chemical exposures are usually localized as well as multiple, most often appearing on the arms .
Arsenic is a well-defined cause of SCC (see Ch. 88 ). A clue to arsenic exposure is the presence of palmoplantar arsenical keratoses. BCC has also been reported following extensive arsenic exposure. The typical latency period from exposure to tumor development is 20–40 years .
Human Papillomavirus Infection
Human papillomaviruses (HPV) represent a large group of DNA tumor viruses that infect the epithelia of both skin and mucosae, inducing hyperproliferative lesions, most commonly warts. HPV is associated with anogenital SCCs, particularly in HIV-infected patients. Individuals with the genetic condition epidermodysplasia verruciformis (EV) are known to have a significantly increased risk of developing SCCs, especially in sun-exposed sites. Infection with the HPV types referred to as EV- or beta-types (see Table 79.1 ) is also observed in the general population, in particular in immunosuppressed solid organ transplant recipients . Because specific HPV subtypes are thought to act as co-carcinogens in conjunction with UVR in the early development of SCC , a goal is to design HPV vaccines that address this issue .
Immunosuppression
Organ transplantation
Solid organ transplant recipients have a markedly increased incidence of skin cancer, primarily SCC. The incidence of BCC in organ transplant recipients is up to 5–10 times greater than in the general population, while the incidence of SCC is 40–250 times greater. Risk factors include skin phototypes I/II, cumulative sun exposure, age at transplantation, and the degree and the length of immunosuppression.
SCC is a significant cause of morbidity and mortality in transplant recipients . The pathogenesis of skin cancer in transplant recipients is multifactorial, involving decreased immunity, direct carcinogenic effects of immunosuppressive medications, and HPV infection in addition to UVR exposure. Transplant recipients are prone to developing numerous lesions and are more likely to suffer local and regional recurrences and metastases . AKs and SCCs begin to appear with increasing frequency several years after transplantation. Lesions are often multiple and usually develop in sun-exposed areas. HPV DNA is found in approximately 70–90% of transplant-associated SCCs. Tumors from transplant recipients contain HPV strains that occur in common benign cutaneous warts (HPV types 1 and 2), EV (HPV-5 and others), high-risk oncogenic warts (HPV types 16 and 18), and low-risk oncogenic genital warts (HPV types 6 and 11). Sometimes, several HPV types are detected within a single tumor.
In one series of renal transplant patients from the US, 5% of the patients died of skin cancer. In another series of heart transplant patients from Australia, 27% died of skin cancer. Two-thirds of these deaths were due to SCC. Several studies have shown that in renal transplant patients sirolimus, an mTOR inhibitor, reduced the development of SCCs when compared to calcineurin inhibitors (e.g. cyclosporine, tacrolimus) . In an Australian study, the SCCs in those receiving sirolimus were more superficial, but this has not been observed in other studies. Based upon currently available data, sirolimus appears to be preferable in patients with a history of SCCs or strong risk factors. Unfortunately, 30–50% of renal transplant patients may not tolerate prolonged administration of sirolimus .
Patients who receive hematopoietic transplants do not experience this marked increase in skin cancer incidence (unless they have received long-term voriconazole), presumably because of a shorter duration of immunosuppression.
Immunosuppressive drugs
Use of immunosuppressive drugs, including systemic immunomodulators (“biologics”), increases the risk for the development of skin cancer . Risk of SCC development is directly related to length of immunosuppressive drug usage. In one study, the risk of SCC was significantly increased among recipients of oral glucocorticoids (odds ratio = 2.31) and the risk of BCC was also elevated (odds ratio = 1.49) . Similarly, thiopurine use for inflammatory bowel disease has been shown to increase the risk for NMSC .
HIV infection
Patients with HIV infection are at increased risk for the development of several cancers, including cutaneous SCC . The incidence of HPV-related SCC of the anus is significantly increased in this population, and can be more aggressive. For monitoring, anal cytology can be performed.
Other Risk Factors, Including BRAF Inhibitors
Up to 25% of patients receiving selective BRAFV600 inhibitors (e.g. vemurafenib, dabrafenib) can develop either SCCs or keratoacanthomas (KAs). They develop primarily in individuals with cutaneous photodamage and can appear within weeks of beginning the kinase inhibitor. Fortunately, the combination of a selective BRAF inhibitor with a MEK inhibitor, as is routinely done nowadays, significantly reduces the incidence of side effects of both drugs, including the formation of SCCs and KAs.
Other possible risk factors include residence at high altitudes, thermal burns, chronic ulcers, and tobacco abuse . While evidence from animal models suggested a relationship between fat intake and skin cancer incidence, results from subsequent epidemiologic studies were inconsistent and failed to show any strong evidence for either this association or for other dietary factors (e.g. vitamins, minerals) .
Genetic Risk Factors
Genetic predisposition
Phenotypic characteristics such as red hair, light skin, poor ability to tan, and freckling have been identified as risk factors for melanoma as well as NMSC . Pigmentation is a polygenic trait, with polymorphisms in several genes leading to the variation observed in the human race (see Ch. 65 ). A key gene encodes the human melanocortin-1 receptor (MC1R) which is expressed on the cell surface of melanocytes. Population-based studies in diverse ethnic groups have shown that the coding region of the human MC1R is remarkably polymorphic. In Caucasians, there is a strong association between nine common MC1R variant alleles and the red hair/fair skin phenotype, thus placing these individuals at higher risk of photocarcinogenesis . Based upon genome-wide association studies and candidate gene studies (see Ch. 54 ), ~30 and at least 11 susceptibility loci for BCC and SCC, respectively, have been identified, and they include multiple pigmentation loci.
Genetic syndromes associated with an increased risk of BCCs and/or SCCs
Xeroderma pigmentosum
Xeroderma pigmentosum (XP) consists of a group of autosomal recessive disorders characterized by defects in unscheduled DNA repair (see Ch. 86 ). A markedly increased incidence of keratinocyte carcinoma and melanoma is observed in these individuals, if they are exposed to sunlight. SCCs and BCCs appear at an early age (median age, 8 years), and in affected individuals who are <20 years of age the risk is 4800 times that of the general population. Strict UV avoidance can significantly decrease skin cancer formation.
Oculocutaneous albinism
Oculocutaneous albinism encompasses a group of autosomal recessive disorders in which there is a variable degree of pigmentary dilution of the skin, eyes, and hair (see Ch. 66 ). At a relatively early age, NMSC, especially SCC, and cutaneous melanoma develop with increased frequency. As in XP, strict sun avoidance for life can greatly minimize tumor development. However, metastatic cutaneous SCC is still a significant problem in areas of the world such as equatorial Africa.
Epidermodysplasia verruciformis
Epidermodysplasia verruciformis (EV) is a rare, usually recessively inherited disorder, in which there is widespread colonization of the skin by HPVs of multiple subtypes, most often 5 and 8 (see Ch. 79 ). Evidence for an association between cutaneous HPV infection and SCC was first reported in these patients. One-third to one-half of patients will develop SCCs as adults, usually in sun-exposed regions, and several decades earlier than is typical for SCC development in the general population. Aggressive biologic behavior, including perineural spread, metastases and death, have been reported.
Dystrophic epidermolysis bullosa
Dystrophic epidermolysis bullosa with significant scarring can result from both dominant and recessive mutations in the type VII collagen gene. SCCs more commonly appear in the recessive forms, where they are the most common cause of death. Tumors usually develop during the third to fifth decades of life, are frequently multiple, and demonstrate aggressive behavior in terms of recurrences and metastases.
Basal cell nevus syndrome (BCNS)
BCNS is an autosomal dominant disorder due to an inactivating mutation in PTCH1 or rarely PTCH2 . Manifestations of the syndrome include multiple or early-onset BCCs, odontogenic keratocysts of the jaw, palmoplantar pits, calcification of the falx cerebri, and skeletal anomalies ( Table 108.3 ; Fig. 108.1 ). Affected individuals may develop specific neoplasms such as medulloblastomas, meningiomas, (bilateral) ovarian fibromas, and cardiac fibromas. Of note, the medulloblastomas usually arise during early childhood, so suspicion of BCNS at an early age allows screening of at-risk individuals .
| DIAGNOSTIC CRITERIA FOR BASAL CELL NEVUS SYNDROME (BCNS) |
| Major criteria |
|
| Minor criteria |
|

BCCs usually appear after puberty, but they may develop during childhood. The number of BCCs in a single patient varies from a few to more than a thousand and the size from pinpoint to >5 cm (see Fig. 108.1A ). The BCCs favor the sun-exposed areas of the face, neck and upper trunk, but may occur in sun-protected sites. As in the general population, nodular BCCs usually occur on the face, while superficial BCCs are found primarily on the torso. Individual lesions may be papulonodular, pedunculated, pigmented, eroded, ulcerated, or have a combination of these features. The pigmented BCCs are sometimes misdiagnosed clinically as melanocytic nevi (see Fig. 108.21 ). The clinical course of the cutaneous tumors is usually indolent prior to puberty, after which they enlarge and eventually ulcerate, as in the general population. Individuals with BCNS are exquisitely sensitive to ionizing radiation, and hundreds of tumors can develop in children within radiation ports following radiotherapy for medulloblastoma. Additional cutaneous findings include epidermoid (infundibular) cysts and facial milia.
Bazex–Dupré–Christol syndrome and Rombo syndrome
Bazex–Dupré–Christol syndrome is a rare condition, consisting of follicular atrophoderma (usually occurring as circumscribed areas on the dorsal aspect of the hands and feet), hypotrichosis, localized hypohidrosis, milia, epidermoid cysts, and multiple, primarily facial, BCCs. The BCCs develop during the second decade of life and frequently have a trichoepithelioma-like histopathologic appearance. In most families, the inheritance pattern is X-linked dominant. Sometimes a source of confusion is the completely different Bazex syndrome (acrokeratosis paraneoplastica), in which psoriasiform plaques of the fingers, toes, ears and nose are often associated with SCC of the upper aerodigestive tract.
The so-called Rombo syndrome has many of the features of Bazex–Dupré–Christol syndrome. Patients have an atrophoderma vermiculatum-like appearance on the cheeks, with evidence of sweat duct proliferation histologically. In addition, they often have hypotrichosis, blepharitis, peripheral (facial/acral) telangiectatic erythema, milia, trichoepitheliomas, and BCCs.
Risk of Additional Cancers
Individuals who have had a BCC or SCC are at increased risk for the development of additional BCCs and SCCs , compared to the general population. They are also at increased risk for developing cutaneous melanoma . Based upon epidemiologic studies, persons with a history of BCCs or SCCs are at increased risk for developing and dying from other (non-skin) cancers .
Actinic Keratosis and Squamous Cell Carcinoma
Clinical Features
Actinic keratosis
Actinic keratoses (AKs) were initially described as solar keratoses (due to their suspected cause) and senile keratoses (due to the age of onset). The term “actinic keratosis” is preferred over solar keratosis, partly because the abbreviation SK also stands for seborrheic keratosis.
AKs have historically been characterized as being “precancerous” or “premalignant” because the atypical keratinocytes within these lesions are confined to the epidermis. There is no risk of metastasis until these lesions evolve into invasive carcinoma. The likelihood of an invasive SCC evolving from a given AK has been estimated to occur at a rate of 0.075–0.096% per lesion per year. Additional estimates of progression to invasive SCC range from 0 to 0.6% per year; the latter figure was derived from an elderly population with a history of keratinocyte carcinoma .
AKs are among the most frequently encountered skin lesions in clinical practice. They present on sun-damaged skin of the head, neck, upper trunk, and extremities ( Fig. 108.2A ). Individuals at higher risk of developing AKs include the elderly, those with lighter skin phototypes and those with a history of chronic sun exposure. The primary lesion is a rough erythematous papule with white to yellow scale. Patients may report tenderness. AKs can range in size from a few millimeters to large confluent patches several centimeters in diameter, especially in patients with severe photodamage. One of the earliest signs is slight erythema with almost imperceptible scale ( Fig. 108.2B ), although some lesions are devoid of visible erythema and present only as slight scale with indistinct borders. A clue to their presence is background photodamage, i.e. dyspigmentation, telangiectasia and solar elastosis (see Ch. 87 ). Advanced lesions are typically thicker and well-defined with more visible hyperkeratosis and erythema. Lesions typically are clustered in areas of highest cumulative sun exposure, such as the superior helices of the ears, upper forehead, supraorbital ridge, nasal bridge, malar eminences, dorsal hands, extensor forearms, shins, and the bald scalp ( Fig. 108.2C ). Of note, clinically, AKs may spontaneously regress, but then can reappear in the same site .
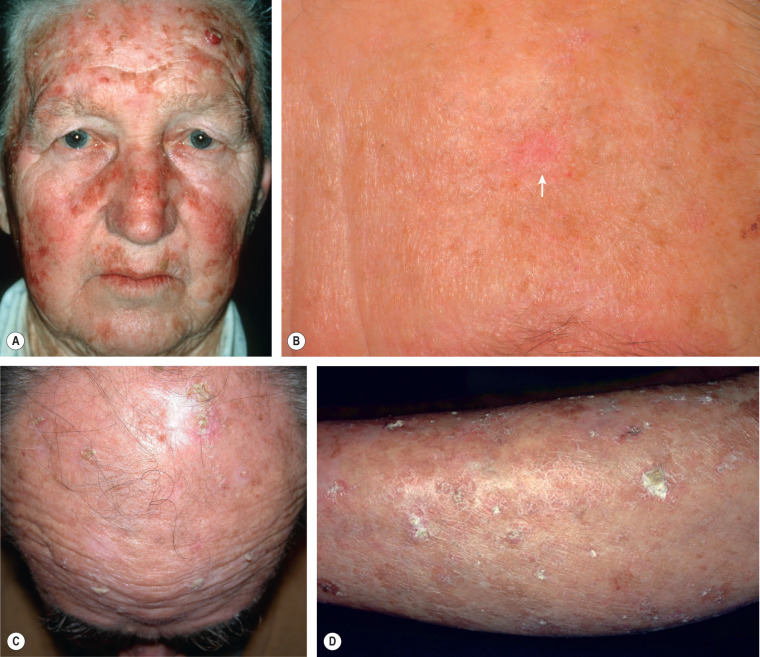
Visual inspection is best performed with simultaneous palpation to detect lesions that may not be readily apparent. This is especially true in individuals with significant background erythema from chronic sun exposure or rosacea. Tenderness on palpation should alert the clinician to the possibility that the lesion has evolved into carcinoma. Clinical subtypes of AKs include the classic variant already described, hypertrophic (or hyperkeratotic), pigmented, lichenoid, atrophic, bowenoid, and actinic cheilitis.
Hypertrophic (hyperkeratotic) AKs are easily identified on visual inspection as papules and plaques with scale or scale-crust and an erythematous base ( Fig. 108.2D ). The erythematous base often extends beyond the overlying hyperkeratosis. The hyperkeratotic scale can become white or yellow–brown over time. Due to their thickness, patients often find these lesions to be bothersome. Sometimes distinction from SCC can be difficult and biopsy is warranted. Occasionally, hyperkeratotic AKs may develop cutaneous horns which manifest as columns of thick cornified material that protrude above the skin. These should be biopsied to exclude the possibility of an underlying malignancy, as ~15% of cutaneous horns have invasive SCC at their bases .
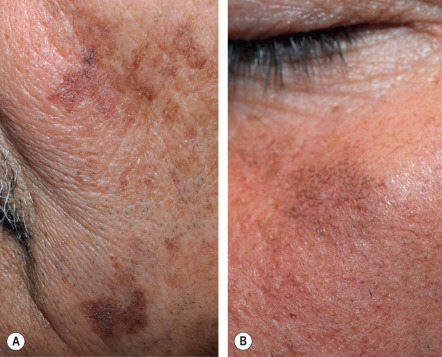
Pigmented AKs, sometimes called superficial pigmented AKs (SPAKs), represent a subtype that often lacks associated erythema and has a hyperpigmented or reticulated appearance ( Fig. 108.3 ). These lesions can at times be difficult to distinguish from reticulated seborrheic keratoses, lentigines, or even the lentigo maligna subtype of cutaneous melanoma. Dermoscopy may be a useful adjunct in these situations. Clinical clues are the location on sun-exposed skin, background solar changes, and hyperkeratosis that is sometimes appreciable by palpation. In cases in which the diagnosis is questionable, a biopsy is required to exclude the possibility of melanoma.
Lichenoid AK is characterized histopathologically by the presence of a dense band-like inflammatory infiltrate. Clinically, this lesion is similar to the classic form of AK but has more erythema surrounding the base of the lesion. Patients may relate pruritus or tenderness that coincides with the onset of the lichenoid infiltrate in a pre-existing AK. It may be confused with a related lesion, the lichen planus-like keratosis, which also arises within areas of sun-damaged skin and can be pruritic, multiple, and eruptive .
Atrophic AKs usually have minimal surface change but are appreciated as pink to red, slightly scaly macules or patches (see Fig. 108.2B ) that are found by histopathologic examination to have an atrophic epidermis.
Actinic cheilitis is the term used to describe the characteristic changes that occur on the lower vermilion lip of individuals with moderate to severe photodamage. Actinic cheilitis may resemble the classic form of AK, with well-demarcated, erythematous papules or thin plaques with scale. In other patients, the erythema and especially the scale is more diffuse and can involve the entire lower vermilion lip; areas of leukoplakia may also be present ( Fig. 108.4 ). When clinical distinction between actinic cheilitis and SCC of the lip is not possible, a biopsy should be performed. The potential for evolving into invasive SCC is higher for actinic cheilitis than it is for classic AKs.

Squamous cell carcinoma in situ
SCC in situ is commonly called Bowen disease ( Fig. 108.5 ). The most common presentation of SCC in situ is an erythematous scaly patch or slightly elevated plaque that often arises within sun-exposed skin of an elderly individual. However, it can develop in younger individuals with significant photodamage or in sun-protected sites. Bowen disease may arise de novo or from a pre-existing AK. The head and neck, followed by the extremities and trunk, are the most common sites. Lesions can become crusted and in SCC in situ of anogenital mucosa, erosions may be prominent ( Fig. 108.6 ).


Clinical distinction of SCC in situ from AK, superficial BCC, psoriasis, or chronic eczema may at times be difficult (see Fig. 108.5B,E ). Generally, AKs are smaller lesions and superficial BCCs often have a more translucent quality with slight elevation of the leading edge as well as characteristic dermoscopic features (see Ch. 0 ). Patients with psoriasis and diffuse actinic damage can pose a diagnostic dilemma, as concomitant psoriatic papules and plaques may clinically resemble AKs and Bowen disease.
Arsenic-induced SCC in situ resembles the classic variety clinically but has a marked tendency to be multifocal and to arise in sun-protected areas of the trunk. Associated findings include palmoplantar keratoses and guttate hypopigmentation superimposed on hyperpigmentation (see Ch. 88 ).
Bowenoid papulosis is a term used when histopathologic changes of SCC in situ are found within genital warts, usually due to infection with an oncogenic strain such as HPV-16 or -18. Dermatologists often prefer to use this term when multiple papules are present, as opposed to calling all of them SCC in situ , because the lesions rarely become invasive. The clinical appearance can vary from small brown papules of the penis to perianal pink papules to corrugated pink to brown plaques of the inguinal creases (see Chs 73 & 79 ). Whether this entity represents true SCC in situ , or is a histopathologic simulant, is a matter of debate.
Other variants of SCC in situ include a pigmented variant often seen in individuals with darker skin types and a verrucous form. Pigmented SCC in situ may be mistaken for a pigmented AK or even a superficial melanoma and verrucous SCC in situ may simulate a seborrheic keratosis or a wart clinically.
Invasive cutaneous squamous cell carcinoma
Invasive cutaneous SCC usually arises within a background of sun-damaged skin, most commonly on the bald scalp, face, neck, extensor forearms, dorsal hands, and shins ( Fig. 108.7A,B ). The color usually varies from erythematous to skin-colored; rarely there are pigmented variants. SCCs are often papulonodular, but can be plaque-like, papillomatous, or exophytic. The degree of associated scale varies, with some lesions becoming quite hyperkeratotic; other secondary changes include crusting, erosions, and ulcerations ( Fig. 108.7C,D ).

The natural history of SCCs also varies, from slowly enlarging to rapidly growing with significant tenderness and even pain. Of note, paresthesias, anesthesia and pain may be signs of perineural invasion. The clinical differential diagnosis, in addition to hypertrophic AK, is outlined in Table 108.4 .
| BASAL CELL CARCINOMA (BCC), SQUAMOUS CELL CARCINOMA (SCC), AND KERATOACANTHOMA (KA) – CLINICAL DIFFERENTIAL DIAGNOSES | |||
|---|---|---|---|
| BCC | SCC | KA | |
| Benign and malignant neoplasms and reactive disorders with pseudoepitheliomatous hyperplasia | |||
| Seborrheic keratosis, including inflamed or irritated | √ | ||
| Lichen planus-like keratosis | √ | √ | |
| Verruca vulgaris, especially periungual | √ | √ | |
| Amelanotic melanoma * | √ | √ | |
| Merkel cell carcinoma | √ | √ | |
| Atypical fibroxanthoma | √ | ||
| Prurigo nodularis | √ | √ | |
| Hypertrophic lichen planus | √ | ||
| Hypertrophic lupus erythematosus | √ | √ | |
| Additional entities | |||
| Cysts, especially inflamed or proliferating variant | √ | ||
| Adnexal carcinomas | √ | √ | |
| Lymphoma cutis, especially ALCL mimicking SCC | √ | ||
| KA-like lesions in cutaneous ALCL and in LyP | √ | √ | |
| DFSP, cutaneous leiomyosarcoma | √ | ||
| Cutaneous metastases from visceral carcinomas | √ | √ | √ |
| Mammary and extramammary Paget disease | √ | √ | |
| Epithelioid sarcoma | √ | ||
| Verrucous melanoma | √ | √ | |
| Molluscum contagiosum | √ | ||
* Pigmented variants of BCC and SCC can also be confused with melanoma.
Staging of SCC takes into account tumor volume as measured by diameter (<2 cm vs ≥2 cm) and depth of invasion (>2 mm), and SCCs arising within sun-damaged skin are often early stage, i.e. T1/AJCC Stage I ( Table 108.5 ). Anatomic sites with a greater risk of aggressive biologic behavior include the ear , the lips ( Fig. 108.8 ), and mucosal sites including the vulva and penis (see Fig. 108.7D ). Clinical examination of patients with invasive SCC includes palpation of regional lymph nodes for enlargement and firmness, followed by assessment of size if enlarged.
| STAGING OF CUTANEOUS SQUAMOUS CELL CARCINOMA (SCC) OF THE HEAD AND NECK | |||
|---|---|---|---|
| T, N, M | |||
| Primary tumor (T) | |||
| TX | Primary tumor cannot be identified | ||
| Tis | Carcinoma in situ | ||
| T1 | Tumor <2 cm in greatest dimension | ||
| T2 | Tumor 2 cm or larger, but smaller than 4 cm in greatest dimension | ||
| T3 | Tumor 4 cm or larger in maximum dimension or minor bone erosion or perineural invasion or deep invasion * | ||
| T4 | Tumor with gross cortical bone/marrow invasion (4a); skull base invasion and/or skull base foramen involvement (4b) | ||
| Regional lymph nodes (clinical) (cN) | |||
| NX | Regional lymph nodes cannot be assessed | ||
| N0 | No regional lymph node metastasis | ||
| N1 | Metastasis in a single ipsilateral lymph node, ≤3 cm in greatest dimension and ENE(−) | ||
| N2 | Metastasis in a single ipsilateral lymph node, >3 cm but <6 cm in greatest dimension and ENE(−) (2a); or in multiple ipsilateral lymph nodes, none >6 cm in greatest dimension and ENE(−) (2b); or in bilateral or contralateral lymph nodes, none >6 cm in greatest dimension and ENE(−) (2c) | ||
| N3 | Metastasis in a lymph node, >6 cm in greatest dimension and ENE(−) (3a); or metastasis in any node(s) and ENE(+) (3b) | ||
| Distant metastasis (M) | |||
| M0 | No distant metastasis | ||
| M1 | Distant metastasis | ||
| Stage | |||
| T | N | M | |
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
| III | T3 | N0 | M0 |
| T1 | N1 | M0 | |
| T2 | N1 | M0 | |
| T3 | N1 | M0 | |
| IV | T1 | N2 | M0 |
| T2 | N2 | M0 | |
| T3 | N2 | M0 | |
| T Any | N3 | M0 | |
| T4 | N Any | M0 | |
| T Any | N Any | M1 | |
* Deep invasion is defined as invasion beyond the subcutaneous fat or >6 mm (as measured from the granular layer of adjacent normal epidermis to the base of the tumor); perineural invasion for T3 classification is defined as tumor cells within the nerve sheath of a nerve lying deeper than the dermis or measuring 0.1 mm or larger in caliber, or presenting with clinical or radiographic involvement of named nerves without skull base invasion or transgression.

Keratoacanthoma
Keratoacanthomas (KAs) are considered by some to be a variant of SCC and by others to represent benign tumors (i.e. pseudomalignancy). The exact nosology is still uncertain, although there are some data that support its differentiation from “conventional” SCC. Typically, a rapidly enlarging papule evolves into a sharply circumscribed, crateriform nodule with a keratotic core over a period of a few weeks ( Fig. 108.9A,B ), and then it may resolve slowly over months to leave an atrophic scar . Most lesions occur on the head and neck or in sun-exposed areas of the extremities, with or without symptoms of pain or tenderness.
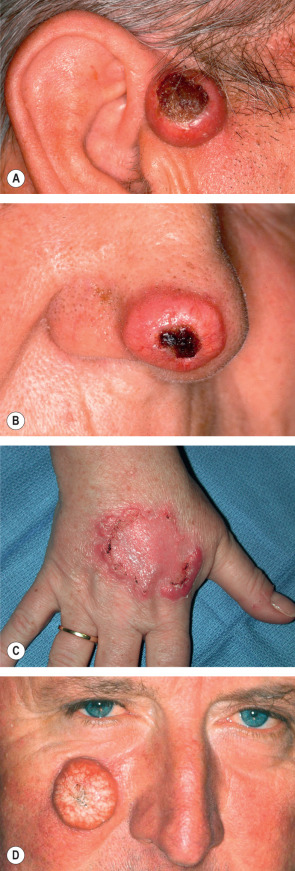
There are several distinct clinical presentations of KA, including solitary, multiple, grouped, keratoacanthoma centrifugum marginatum ( Fig. 108.9C ), giant ( Fig. 108.9D ), subungual, palmoplantar, intraoral, multiple spontaneously regressing (Ferguson–Smith), multiple non-regressing, and generalized eruptive (Grzybowski). KAs are also seen in patients with Muir–Torre syndrome and they may have sebaceous differentiation (see Ch. 63 ). In addition, multiple KAs have been associated with chemical exposures, immunosuppression , BRAF inhibitors, and HPV infection .
By far the most common presentation is the solitary KA. While most of these tumors are small (5 to 15 mm), some KAs (e.g. keratoacanthoma centrifugum marginatum [see Fig. 108.9D ]) may reach several centimeters in diameter, persist for months before resolution, and heal with prominent scarring. Grouped KAs may resolve more slowly than solitary KAs, while subungual KAs have been associated with underlying bony destruction.
The Ferguson–Smith syndrome is an autosomal dominant condition due to mutations in TGFBR1 which encodes TGF-β receptor type 1. Multiple KAs develop within sun-exposed areas, usually beginning during the third decade of life. Lesions typically regress over weeks to months, but rare examples of metastases have been reported.
Multiple KAs of the Grzybowski type present as thousands of papules resembling milia or early eruptive xanthomas. They develop rapidly and may slowly resolve over a period of months . Patients often have scarring, ectropion, and a mask-like facies.
Verrucous carcinoma
Verrucous carcinoma is a rare, well-differentiated variant of SCC which tends to occur in middle-aged and older adults. It is considered a low-grade malignancy with three major subtypes: (1) epithelioma cuniculatum (plantar surface of the foot); (2) giant condyloma acuminatum of the genitalia (also known as Buschke–Löwenstein tumor; see Ch. 79 ); and (3) oral florid papillomatosis (oral mucosa). Of note, the “cuniculatum” refers to the rabbit burrow-like appearance with crevices.
Clinically, verrucous carcinomas present as large (sometimes huge), exophytic tumors with a papillomatous or verrucous surface ( Fig. 108.10A,B ). They are commonly associated with HPV infection, and distinguishing between a verrucous carcinoma and a large wart or condyloma acuminatum can be difficult. Gradual penetration of verrucous carcinomas into underlying tissues can result in destruction of subcutis, fascia, and bone. These tumors can arise within scars and amputation stumps ( Fig. 108.10C ) as well as in association with osteomyelitis fistulae and chronic venous insufficiency. Verrucous carcinomas often recur after attempted removal, but they usually do not metastasize, except for recurrent or irradiated tumors with anaplastic transformation.










