Abstract
Acne vulgaris is one of the skin disorders most frequently encountered by dermatologists as well as primary care providers. It is especially common in adolescents but also occurs in children and adults, and its psychological impact can be profound. Acne is an inflammatory disorder involving the pilosebaceous unit and results from the complex interplay of genetics, hormonal influences, innate and acquired immunity, and other environmental factors. Presentations range from a few comedones to a fulminant systemic condition, with multiple acne variants in addition to related acneiform eruptions. Treatments are geared at targeting as many of the pathogenic factors as possible in order to achieve disease control.
Keywords
acne vulgaris, acne fulminans, neonatal acne, infantile acne, acneiform eruptions, retinoids, isotretinoin, spironolactone, Propionibacterium acnes
Introduction
Acne vulgaris is a multifactorial disorder of the pilosebaceous unit. The clinical picture can vary significantly, from mild comedonal acne to fulminant systemic disease. Although all age groups may be affected by its many variants, the peak incidence is during adolescence. Acne has an undeniable psychosocial impact, and affected individuals have an increased likelihood of self-consciousness, social isolation, anxiety disorders, depression, and even suicidal ideation . Insights into the pathogenesis of acne have aided significantly in further defining the subtypes of acne and establishing effective treatment regimens.
History
In the sixth century AD, the term “acne” was first used by the Emperor Justinian’s physician, Aetius Amidenus. It was later translated from Greek into Latin, and through these translations confusion arose regarding its original meaning . The debate continues as to whether its origin is from the Greek acme , meaning peak, or whether acne was actually the original term. Its use became obsolete until the 1800s, when “acne” regained a place in medical dictionaries. In 1842, Erasmus Wilson separated acne simplex (acne vulgaris) from acne rosacea .
Epidemiology, Including Genetic and Dietary Factors
Acne vulgaris affects approximately 40–50 million individuals each year in the US alone, leading to an estimated annual cost in the US of at least $2.5 billion. Globally, acne accounts for ~0.3% of the total and ~16% of the dermatologic disease burden . With a peak incidence during adolescence, acne affects approximately 85% of young people between 12 and 24 years of age and is therefore a physiologic occurrence in this group. With the general trend over the past few decades for earlier puberty, preadolescent acne affecting children 7 to 11 years of age has also become more common . While typically thought of as a disease of youth, acne often continues to be problematic well into adulthood. In a survey-based study in the US, 35% of women and 20% of men reported having acne in their 30s, while 26% of women and 12% of men were still affected in their 40s . Caucasian boys and men have a tendency to have more severe nodulocystic disease than other groups.
Individuals at increased risk for the development of acne include those with an XYY karyotype or endocrine disorders such as polycystic ovarian syndrome, hyperandrogenism, hypercortisolism, and precocious puberty. Patients with these conditions tend to have more severe acne that is less responsive to standard therapy.
Genetic Factors
The precise role of genetic predisposition in the multifactorial pathogenesis of acne remains to be determined. The number, size, and activity of sebaceous glands is inherited. In addition, the concordance rate for the prevalence and severity of acne among identical twins is extremely high. It is a widely held belief that the tendency to have substantial acne (including the nodulocystic variant) runs in families, and an association between moderate to severe acne and a family history of acne has been observed in several studies . Genes found to have a possible link to acne via genome-wide association studies (GWAS) and other methods include those encoding components of the tumor growth factor-β pathway, other inflammatory mediators, and regulators of androgen metabolism .
Dietary Factors
The relationship between diet and acne remains a subject of controversy. Several observational studies in different ethnic groups have found that intake of milk, especially skim milk, is positively associated with acne prevalence and severity . Exacerbation of acne with the use of whey protein supplements for body building has also been reported. In addition, prospective studies have documented a link between a high glycemic-load diet and acne risk . A recent investigation found that vitamin B 12 supplementation can potentially trigger the development of acne by altering the transcriptome of skin microbiota, leading to increased production of proinflammatory porphyrins by Propionibacterium acnes .
Pathogenesis
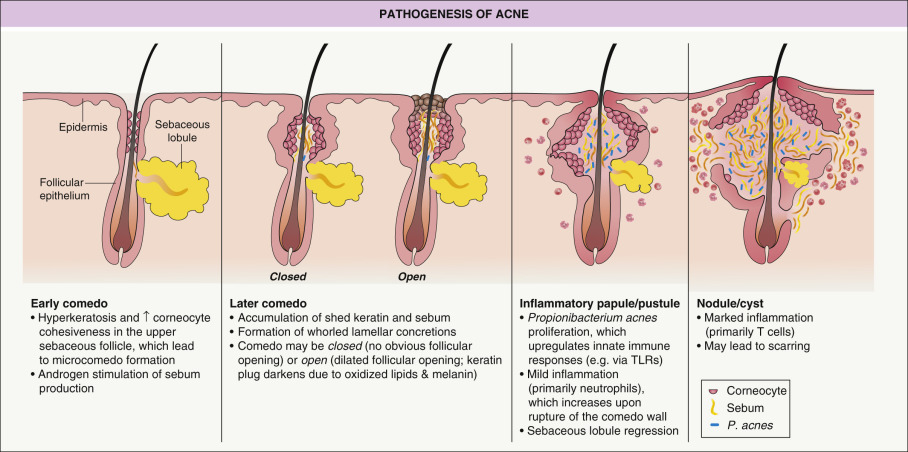
The development of acne involves the interplay of a variety of factors, including: (1) follicular hyperkeratinization; (2) hormonal influences on sebum production and composition; and (3) inflammation, in part mediated by P. acnes ( Fig. 36.1 ). Appreciating the anatomy and physiology of the pilosebaceous unit is essential to understanding the pathogenesis of acne and designing effective treatment regimens. The structure and function of sebaceous glands are reviewed in detail in Chapter 35 , with summaries of their roles in acne in Table 35.4 and Fig. 35.5 .
Follicular Hyperkeratinization
The microcomedo is thought to be the precursor of all clinically apparent acne lesions. It forms in the upper portion of the follicle within the lower portion of the infundibulum, the infrainfundibulum. Corneocytes, which are normally shed into the lumen of the follicle and extruded, accumulate due to increases in both follicular keratinocyte proliferation and corneocyte cohesiveness, leading to the development of a hyperkeratotic plug and a bottleneck phenomenon. The inciting event for microcomedo formation is unknown, but data support a putative role for interleukin-1α (IL-1α) .
Hormonal Influences on Sebum Production and Composition
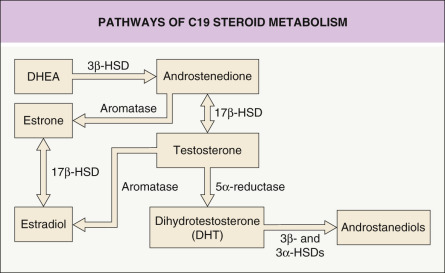
The sebaceous gland is controlled primarily by androgens, with additional influences from other hormones and neuropeptides (see Table 35.4 ). Androgens are produced both outside the pilosebaceous unit, mainly by the gonads and adrenal glands, and locally within the sebaceous gland via the action of androgen-metabolizing enzymes such as 3β-hydroxysteroid dehydrogenase (HSD), 17β-HSD and 5α-reductase ( Fig. 36.2 ). Androgen receptors, found in the cells of the basal layer of the sebaceous gland and the outer root sheath of the hair follicle, are responsive to testosterone and 5α-dihydrotestosterone (DHT), the most potent androgens. DHT has a 5–10-fold greater affinity than testosterone for the androgen receptor and is thought to be the principal androgen mediating sebum production.
The impact of androgens on sebaceous gland activity begins during the neonatal period. From birth until approximately 6–12 months of age, infant boys have elevated levels of luteinizing hormone (LH), which stimulates testicular production of testosterone. In addition, both male and female infants exhibit increased levels of dehydroepiandrosterone (DHEA) and DHEA sulfate (DHEAS) secondary to a large, androgen-producing “fetal zone” in the adrenal gland that involutes during the first year of life. Of note, sebaceous gland activity in infants is not due to persistent maternal hormonal stimulation, as was previously hypothesized. Both testicular and adrenal androgen production decrease substantially by 1 year of age and remain at a stable nadir until adrenarche.
With the onset of adrenarche, typically at 7–8 years of age, circulating levels of DHEAS begin to rise due to its production by the adrenal gland. This hormone can serve as a precursor for the synthesis of more potent androgens within the sebaceous gland (see Fig. 36.2 ). The rise in serum levels of DHEAS in prepubescent children is associated with an increase in sebum production and often the initial development of comedonal acne . Although the overall composition of sebum is similar in persons with or without acne, those with acne have variable degrees of seborrhea and their sebum tends to have higher levels of squalene monounsaturated fatty acids but less linoleic acid .
Little is known about the physiologic role of estrogens in modulating sebum production. Estrogen administered systemically in sufficient amounts decreases sebum production , although the dose of estrogen needed is greater than the dose required to suppress ovulation and increases the risk of thromboembolic events. However, acne often responds to treatment with lower-dose oral contraceptives containing 20–50 mcg of ethinyl estradiol or its esters, because suppression of ovulation itself inhibits ovarian androgen production. Postulated mechanisms for estrogen-mediated downregulation of sebogenesis include direct opposition of androgens within the sebaceous gland, a negative feedback loop that decreases androgen production via inhibition of pituitary gonadotropin release, and regulation of genes that affect sebaceous gland activity.
Inflammation in Acne
Although tremendous progress has been made in our understanding of acne as an inflammatory process, several questions remain regarding inflammation during acne lesion development. It is clear that when a follicle involved with acne ruptures, it exudes keratin, sebum, P. acnes , and cellular debris into the surrounding dermis, thereby significantly intensifying inflammation. However, inflammation is also seen early in acne lesion formation. For example, in acne-prone sites, the number of CD4 + T cells and levels of IL-1 have been shown to be increased perifollicularly prior to hyperkeratinization . In addition, insulin-like growth factor-1 has been found to increase the expression of inflammatory markers and sebum production in cultured sebocytes.
The type of inflammatory response determines the clinical lesion seen. If neutrophils predominate (typical of early lesions), suppuration occurs and a pustule is formed. Neutrophils also promote the inflammatory response by releasing lysosomal enzymes and generating reactive oxygen species; levels of the latter in the skin and plasma may correlate with acne severity . An influx of lymphocytes (predominately T helper cells), foreign body-type giant cells, and neutrophils results in inflamed papules, nodules, and cysts. The type of inflammatory response also plays a role in the development of scarring. Early, nonspecific inflammation results in less scarring than does a delayed, specific inflammatory response .
Propionibacterium acnes and the Innate Immune System
P. acnes is a Gram-positive, anaerobic/microaerophilic rod that is found deep within the sebaceous follicle, often together with smaller numbers of P. granulosum . In adults, P. acnes is the predominant organism in the microbiome of the face and other sebaceous skin. P. acnes produces porphyrins (primarily coproporphyrin III) that fluoresce with Wood’s lamp illumination.
For the most part, P. acnes is considered to be a commensal organism of the skin rather than a pathogen per se . Although studies have documented increased levels of P. acnes on the facial skin of acne patients, the P. acnes density does not correlate with clinical severity . Because P. acnes is nearly ubiquitous yet not everyone has acne, differences in the pathogenicity of particular P. acnes strains and variable host responses to P. acnes have been postulated. In a comparison of the microbiome of facial skin in individuals with and without acne, certain ribotypes of P. acnes (types 4 and 5) were more frequently found in acne patients, suggesting that these strains are either more capable of inducing acne or better suited to survive in an acne environment . However, another study showed that monocytes from the peripheral blood of patients with acne exhibited more robust cytokine release in response to P. acnes stimulation than did monocytes from individuals without acne, but no differences were observed when P. acnes strains isolated from acne lesions were compared to strains from the normal skin of unaffected adults .
The pathogenicity of P. acnes includes the direct release of lipases, chemotactic factors, and enzymes that contribute to comedo rupture, as well as stimulation of inflammatory cells and keratinocytes to produce proinflammatory mediators and reactive oxygen species. Interactions between the skin’s innate immune system and P. acnes play an important role in acne pathogenesis. One mechanism is via Toll-like receptors (TLRs), a class of transmembrane receptors that mediates the recognition of microbial pathogens by immune cells (monocytes, macrophages, and neutrophils) as well as by keratinocytes (see Ch. 4 ). TLR2, which recognizes lipoproteins and peptidoglycans as well as CAMP factor 1 produced by inflammatory strains of P. acnes , is found on the surface of macrophages surrounding acne follicles . P. acnes has also been shown to increase expression of TLR2 and TLR4 by keratinocytes. Through activation of the TLR2 pathway, P. acnes stimulates the release of proinflammatory mediators such as IL-1α, IL-8, IL-12, tumor necrosis factor-α [TNF-α], and matrix metalloproteinases . IL-8 leads to neutrophil recruitment, the release of lysosomal enzymes, and subsequent disruption of the follicular epithelium, while IL-12 promotes Th1 responses (see Ch. 4 ).
P. acnes has also been shown to activate the NOD-like receptor protein 3 (NLRP3) of inflammasomes in the cytoplasm of both neutrophils and monocytes, resulting in the release of proinflammatory IL-1β . In addition, recent studies have shown that P. acnes stimulates Th17 responses in acne lesions . Lastly, P. acnes can induce monocytes to differentiate into two distinct innate immune cell subsets: (1) CD209 + macrophages, which more effectively phagocytose and kill P. acnes and whose development is promoted by tretinoin; and (2) CD1b + dendritic cells that activate T cells and release proinflammatory cytokines .
Clinical Features
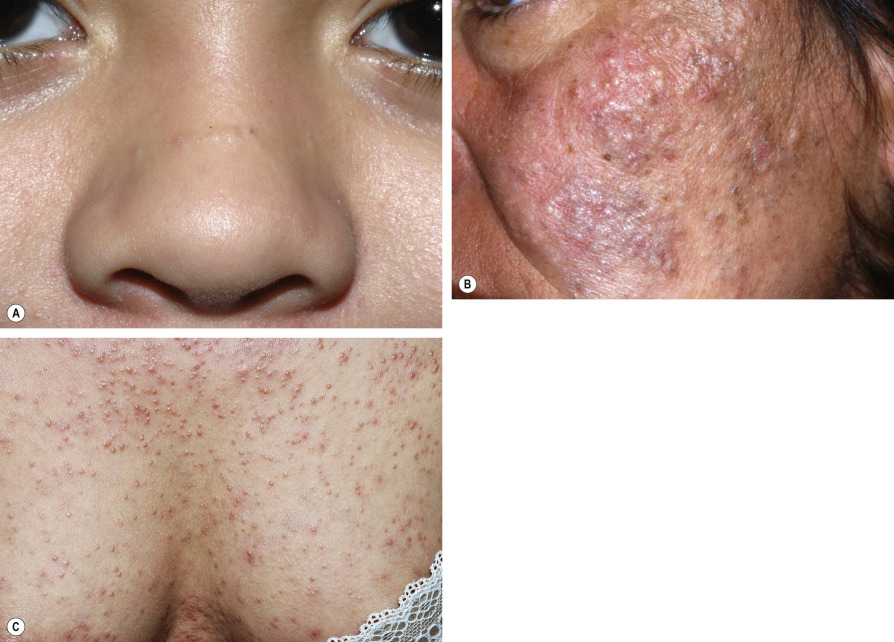
Acne is typically found in sites with well-developed sebaceous glands, most often the face and upper trunk. Despite evidence that inflammation is present in even the earliest comedones, acne lesions are divided into non-inflammatory and inflammatory groups based upon their clinical appearance. Non-inflammatory acne is characterized by open and closed comedones ( Fig. 36.3 ). The histologic features of these follicular-based lesions are reflected in their clinical appearance. Closed comedones (whiteheads) are generally small (~1 mm), skin-colored papules with no apparent follicular opening or associated erythema. These lesions may be subtle and better appreciated upon palpation, stretching, or side-lighting of the skin. In contrast, open comedones (blackheads) have a conspicuous dilated follicular opening that is filled with an inspissated core of shed keratin (see Fig. 36.5 ). Melanin deposition and lipid oxidation within the debris may be responsible for the black color.

Inflammatory acne is characterized by papules, pustules, and nodules of varying severity ( Figs 36.4–36.7 ). Erythematous papules typically range from 1 to 5 mm in diameter. Pustules tend to be approximately equal in size and are filled with white purulent material and normal flora, including P. acnes . As the severity of lesions progresses, nodules form and become markedly inflamed, indurated and tender. The pseudocysts of acne are deeper and filled with a combination of pus and serosanguineous fluid. In patients with severe nodulocystic acne, these lesions frequently coalesce to form large, complex, inflamed plaques that can include sinus tracts.




Early treatment of acne is essential for the prevention of lasting cosmetic disfigurement due to scarring. Erythema and postinflammatory hyperpigmentation ( Fig. 36.8 ) often persist after resolution of inflammatory acne lesions. Although the pigmentary changes usually fade over many months if the acne is brought under control, occasionally they can be permanent. Unfortunately, pitted scars ( Fig. 36.9 ) or hypertrophic scars (most commonly on the trunk; see eFig. 98.1 ) are often sequelae of nodulocystic acne.


Acne Variants
Post-adolescent acne in women
Inflammatory acne beyond 25 years of age is most common in women and may be associated with a high level of psychological stress . The majority of affected women present with findings similar to those of adolescent acne, with a mixture of inflammatory and comedonal lesions involving various facial sites and sometimes the trunk . Although the mandibular area is involved in ~80% of women with acne, a distinct smaller subset has inflammatory papules, pustules, and nodules exclusively in this location. Half of women report persistence of their acne since its onset, often during adolescence, while one-quarter describe periods of remission followed by recurrences. Premenstrual flares are common , but only ~20% of women with acne have irregular menses. Up to 30% of those in the latter group have other signs of hyperandrogenism, such as hirsutism and androgenetic alopecia (see below). A predominantly comedonal, adult-onset form of acne that is associated with smoking has also been described .
Acne fulminans
Acne fulminans is the most severe form of acne and is characterized by the abrupt development of nodular and suppurative acne lesions in association with systemic manifestations. This uncommon variant primarily affects boys 13–16 years of age. Patients typically have mild to moderate acne prior to the onset of acne fulminans, when numerous microcomedones suddenly erupt and become markedly inflamed. There is rapid coalescence into painful, oozing, friable plaques with hemorrhagic crusts ( Fig. 36.10 ). The face, neck, trunk, and arms are all affected. Lesions tend to ulcerate and can lead to significant scarring.

Osteolytic bone lesions may accompany the cutaneous findings; the clavicle and sternum are most commonly affected, followed by the ankles, humerus and iliosacral joints. Systemic manifestations include fever, arthralgias, myalgias, hepatosplenomegaly, and severe malaise. Erythema nodosum may also arise in association with acne fulminans. Laboratory abnormalities vary and include an elevated ESR, proteinuria, leukocytosis, and anemia. Laboratory studies are not required to establish the diagnosis, but their evolution may parallel the clinical course and response to therapy. The related s ynovitis, a cne, p ustulosis, h yperostosis, and o steitis (SAPHO) syndrome, which can accompany acne fulminans, is discussed in detail in Chapter 26 . Acne fulminans has also been associated with late-onset congenital adrenal hyperplasia and anabolic steroid use, including therapeutic testosterone.
Recommended treatment of acne fulminans includes prednisone 0.5–1 mg/kg/day as monotherapy for at least 2–4 weeks, followed by initiation of low-dose isotretinoin (e.g. 0.1 mg/kg/day) after the acute inflammation subsides; after at least 4 weeks of this combination, the isotretinoin dose can be slowly increased and the prednisone tapered over a period of 1–2 months . Paradoxically, an acne fulminans-like flare occasionally develops during the first few weeks of isotretinoin therapy for acne ; this may be avoided by starting with a low dose of isotretinoin and concomitant administration of oral corticosteroids at the first sign of a flare or possibly preemptively in high-risk patients (see Ch. 126 ). Additional treatment options for acne fulminans include topical or intralesional corticosteroids, oral antibiotics (generally of limited efficacy), TNF-α inhibitors, interleukin-1 antagonists, and immunosuppressive agents (e.g. azathioprine, cyclosporine). Dapsone may be particularly beneficial in the treatment of acne fulminans associated with erythema nodosum .
Acne conglobata and associated conditions
Acne conglobata is a severe form of nodulocystic acne that may have an eruptive onset but without systemic manifestations. This recalcitrant acne variant is part of the follicular occlusion tetrad, along with dissecting cellulitis of the scalp, hidradenitis suppurativa, and pilonidal sinus (see Ch. 38 ).
The association of sterile p yogenic a rthritis, p yoderma gangrenosum, and a cne conglobata can occur in the context of an autosomal dominant autoinflammatory disorder referred to as PAPA syndrome, which is caused by mutations in PSTPIP1 which encodes p roline– s erine– t hreonine p hosphatase i nteracting p rotein 1 . Dysfunction of PSTPIP1, which has a role in actin reorganization and interacts with the pyrin protein (defective in familial Mediterranean fever), compromises the physiologic signaling required for maintenance of a proper inflammatory response. PSTPIP1 mutations have also been identified in a patient with p yogenic a rthritis, p yoderma gangrenosum, a cne, and s uppurative h idradenitis (PAPASH) syndrome, but to date not in the related p yoderma gangrenosum, a cne, and s uppurative h idradenitis (PASH) syndrome . Of note, a possible association between nodulocystic acne and inflammatory bowel disease may potentially confound links that have been observed between the latter disorder and acne therapies such as tetracyclines and isotretinoin .
Solid facial edema
An unusual and disfiguring complication of acne vulgaris is solid facial edema (Morbihan disease). Clinically, there is a distortion of the midline face and cheeks due to soft tissue swelling ( Fig. 36.11 ). The woody induration may be accompanied by erythema. Impaired lymphatic drainage and fibrosis (potentially induced by mast cells) in the setting of chronic inflammation are thought to be involved in the pathogenesis of solid facial edema, and a report of its occurrence in identical twins with acne suggests that genetic factors may also have a role. Similar changes have been described in patients with rosacea (see Table 36.2 ). Although fluctuations in severity are common, solid facial edema does not usually resolve spontaneously. Treatment with isotretinoin (0.2–1 mg/kg/day) for 4–6 months has been reported to lead to improvement, although a more extended course of 9–24 months is often required . Combination of isotretinoin with ketotifen 1–2 mg/day (not available in the US) or prednisone 10–30 mg/day may have additional benefit .

Neonatal acne (neonatal cephalic pustulosis)
Neonatal acne occurs in more than 20% of healthy newborns (see Ch. 34 ). Lesions usually appear at about 2 weeks of age and generally resolve within the first 3 months of life. Small papulopustules (not comedones) arise primarily on the cheeks, forehead, eyelids and chin, although the neck and upper trunk can also be involved (see Fig. 34.6 ).
The pathogenesis of neonatal acne has been the subject of debate. An inflammatory response to Malassezia spp. (e.g. sympodialis, furfur ) has been proposed as the etiology by some investigators, leading to a renaming of the disorder as “neonatal cephalic pustulosis”. Additional support for this view comes from the clinical response to treatment with topical imidazoles (e.g. ketoconazole 2% cream). The active sebaceous glands and high sebum excretion rate in neonates (see Pathogenesis ) are also thought to play a role. The substantial decline in sebum production after the first few months of life helps to explain the limited period of susceptibility to neonatal acne. Given the transient and benign nature of this eruption, parental reassurance alone is usually adequate. However, as noted previously, therapy with topical imidazoles can be effective.
Infantile acne
Typically, infantile acne initially presents at 2–12 months of age . In contrast to neonatal acne, comedo formation is prominent and pitted scarring may develop in up to half of patients ( Fig. 36.12 ). Deep, suppurative nodules are occasionally seen. Its pathogenesis reflects the androgen production intrinsic to this stage of development (see above), including elevated levels of LH stimulating testicular production of testosterone in boys during the first 6–12 months of life and elevated levels of DHEA produced by the infantile adrenal gland in both boys and girls. These androgen levels normally decrease substantially by 12 months of age and remain at nadir levels until adrenarche. Patients with infantile acne should be assessed for signs of hyperandrogenism (see below), precocious puberty, or abnormal growth; if these findings are present, endocrinologic evaluation including a hand/wrist X-ray to determine bone age and laboratory testing of hormone levels should be performed.

Infantile acne usually resolves within 6–18 months and remains quiescent until around puberty, with an increased risk of severe acne during adolescence having been observed . Topical retinoids (e.g. tretinoin, adapalene) and benzoyl peroxide are first-line treatments for infantile acne. Oral antibiotics (e.g. erythromycin, azithromycin) can be helpful for patients with a more severe inflammatory component, and isotretinoin is occasionally required for recalcitrant or nodulocystic presentations .
Mid-childhood acne
Acne presenting between 1 and 6 or 7 years of age is categorized as “mid-childhood acne” . Because this is an uncommon time for acne development due to quiescent androgen production, the possibility of an underlying hyperandrogenic condition such as premature adrenarche, congenital adrenal hyperplasia, or an androgen-secreting tumor should be considered. In addition to a thorough history and physical examination to assess for signs of hyperandrogenism (see below) and precocious puberty, the child’s growth curve should be carefully reviewed and a hand/wrist bone age X-ray performed if there are signs of accelerated growth. A complete endocrine evaluation is required if any abnormalities are present . Treatment strategies are the same as for infantile acne.
Preadolescent acne
It is common for acne to begin to develop in children 7 or 8 to 11 years of age, often prior to other signs of pubertal maturation . Preadolescent acne tends to be primarily comedonal and favors the forehead and central face (“T-zone”). Polycystic ovary syndrome (PCOS) and other endocrinologic abnormalities should be considered when the acne is unusually severe or accompanied by signs of hyperandrogenism. Treatment is similar to that for adolescent acne, although tetracyclines should be avoided in children <8 years of age, and it is important to consider the degree to which the acne bothers the patient.
Acne excoriée
Acne excoriée occurs more often in young women, in whom it may be referred to as acne excoriée des jeunes filles. Typical comedones and inflammatory papules are systematically excoriated in a ritualistic manner, leaving crusted erosions that may scar (see Ch. 7 ). Linear erosions suggest self-manipulation, and an underlying psychiatric component should be considered. Individuals with an anxiety, obsessive-compulsive, or body dysmorphic disorder are particularly at risk, and antidepressants or psychotherapy may be helpful in these patients.
Acne associated with endocrinologic abnormalities
Although most patients with acne do not have overt endocrinologic abnormalities, hyperandrogenism should be suspected in women and late adolescent girls with irregular menstrual periods. Acne in such patients is often severe or more difficult to treat, and the onset can be fairly abrupt. Other signs and symptoms of hyperandrogenism in women and children include hirsutism (see Ch. 70 ), coarsening of the voice, a muscular habitus, androgenetic alopecia, clitoromegaly with variable posterior labial fusion, and increased libido. I nsulin r esistance and a canthosis n igricans can occur in association with h yper a ndrogenism in the HAIR-AN syndrome. These patients are at increased risk for accelerated cardiovascular disease and diabetes mellitus, and they should be followed by appropriate medical specialists.
The evaluation of patients suspected of having hyperandrogenism includes a thorough history and physical examination; the age of the patient and pubertal status are also important parameters. Prepubertal children, adolescent girls, and women with signs of hyperandrogenism should undergo appropriate evaluation, and laboratory studies should not be performed while the patient is taking oral contraceptives. Initial tests typically include serum levels of total and free testosterone, DHEAS, and 17-hydroxyprogesterone. Patients with clinical findings suggestive of hypercortisolism should also be initially assessed with either a late-night salivary cortisol level, 24-hour urine cortisol level, or low-dose dexamethasone suppression test. X-rays of the hand and wrist to evaluate bone age should be obtained in prepubertal children (see Mid-childhood acne ).
Understanding pathways of hormone production is essential in the evaluation of hyperandrogenic states (see Fig. 70.17 ). For example, an elevated serum DHEAS or 17-hydroxyprogesterone level indicates an adrenal source of excess androgen production. The degree to which levels of these hormones are increased is then useful in discerning an etiology. DHEAS values in the range of 4000–8000 ng/ml or 17-hydroxyprogesterone levels >3 ng/ml may be indicative of congenital adrenal hyperplasia. Defects in adrenal enzymes, most commonly 21-hydroxylase or (less often) 11-hydroxylase, lead to this condition. Patients with severe deficiencies of these enzymes become symptomatic during infancy, whereas those with partial deficiencies present in adolescence. If the serum DHEAS is >8000 ng/ml, with or without an elevated testosterone level, an adrenal tumor should be suspected.
If the testosterone levels (total and free) are elevated and the DHEAS level is relatively normal, an ovarian source is likely. Polycystic ovary syndrome (PCOS) is the most common condition associated with an elevated serum testosterone, with levels typically ranging from 100 to 200 ng/dl. An increased LH/FSH ratio (>2–3) is also commonly observed. Symptoms of PCOS include irregular menstrual periods, hirsutism, obesity, insulin resistance, and reduced fertility (see Fig. 70.12 ). When levels of serum testosterone exceed 200 ng/dl, an ovarian tumor should be considered.
Acne associated with genetic syndromes
Apert syndrome (acrocephalosyndactyly type I) is an autosomal dominant disorder that features disfiguring synostoses of the bones of the hands and feet, vertebral bodies, and cranium. Affected individuals have an increased incidence of severe, early-onset acne that tends to be nodulocystic and have a more widespread distribution than in classic acne, often involving the entire extensor aspects of the arms, buttocks and thighs . Acne in patients with Apert syndrome is typically resistant to therapy, although isotretinoin has been reported to be beneficial. Other cutaneous findings in this disorder can include marked seborrhea, nail anomalies (e.g. a single nail for the second through fourth digits), and diffuse pigmentary dilution of the hair and skin. Of note, Apert syndrome results from activating mutations in FGFR2 , which encodes fibroblast growth factor receptor 2; mosaicism for the same FGFR2 mutations has been found to underlie acneiform/comedonal nevi (see Ch. 62 ). FGFR2 signaling has been shown to have effects on follicular keratinocyte proliferation, sebaceous lipogenesis, and inflammatory cytokine production.
Borrone dermato-cardio-skeletal syndrome , an autosomal recessive disorder caused by SH3PXD2B mutations, is characterized by dysmorphic facies, thick skin, acne conglobata, vertebral abnormalities, and mitral valve prolapse. PAPA syndrome and related conditions are discussed in the section on acne conglobata.
Acneiform Eruptions
Drug-induced acne
Acne or acneiform eruptions (e.g. folliculitis) can be seen as a side effect of a number of medications ( Table 36.1 ). An abrupt, monomorphous eruption of inflammatory papules and pustules is often observed in drug-induced acne ( Figs 36.13 & 36.14 ), in contrast to the heterogeneous morphology of lesions seen in acne vulgaris. When a history of prescription medication use is not elicited, a comprehensive review of all over-the-counter medications and supplements, as well as recent medical procedures, may reveal the responsible agent (see Table 36.1 ). Bodybuilders and athletes should be questioned about anabolic steroid use.
| CAUSES OF DRUG-INDUCED ACNE | |
|---|---|
| Common | Uncommon |
| Anabolic steroids (e.g. danazol, testosterone) | Azathioprine |
| Bromides * | Cyclosporine |
| Corticosteroids (see Fig. 36.13 ) | Disulfiram |
| Corticotropin | Ethosuximide |
| EGFR inhibitors (see Fig. 36.15 and Ch. 21 ) | Phenobarbital |
| Iodides † | Propylthiouracil |
| Isoniazid (see Fig. 36.14 ) | Psoralen + ultraviolet A |
| Lithium | Quinidine |
| MEK inhibitors (e.g. trametinib) | Quetiapine |
| Phenytoin | TNF inhibitors |
| Progestins (see text) | Vitamins B 6 and B 12 |
* Found in sedatives, analgesics and cold remedies.
† Found in contrast dyes, cold/asthma remedies, kelp, and combined vitamin–mineral supplements.


High-dose intravenous or oral corticosteroids commonly induce characteristic acneiform eruptions with a concentration of lesions on the chest and back (see Fig. 36.13 ). Steroid-induced acne (and rosacea) can also result from the inappropriate use of topical corticosteroids on the face. Inflamed papules and pustules develop on a background of erythema that favors the distribution of corticosteroid application. Lesions eventually resolve following discontinuation of the corticosteroid, although “steroid dependency” can lead to prolonged and severe flares post-withdrawal (see Ch. 37 ).
E pidermal g rowth f actor r eceptor (EGFR) inhibitors used for the treatment of solid tumors also have a high incidence of acneiform papulopustular eruptions ( Fig. 36.15 ; see Chapter 21 ).

Occupational acne, acne cosmetica, and pomade acne
Exposure to insoluble, follicle-occluding substances in the workplace is responsible for occupational acne (see Ch. 16 ). Offending agents include cutting oils, petroleum-based products, chlorinated aromatic hydrocarbons, and coal tar derivatives. Comedones dominate the clinical picture, with varying numbers of papules, pustules and cystic lesions distributed in exposed as well as typically covered areas. Primarily comedonal facial acne, with a predominance of closed comedones, can also develop in sites chronically exposed to follicle-occluding cosmetics ( acne cosmetica ) or hair products. The latter, referred to as pomade acne , favors the forehead and temples.
Chloracne
Chloracne is due to exposure to halogenated aromatic hydrocarbons. It typically develops several weeks after systemic exposure, which can occur via percutaneous absorption, inhalation, or ingestion. The following agents, found in electrical conductors and insulators, insecticides, fungicides, herbicides and wood preservatives, have all been implicated: polychlorinated naphthalenes, biphenyls, dibenzofurans and dibenzodioxins; polybrominated naphthalenes and biphenyls; tetrachloroazobenzene; and tetrachloroazoxybenzene.
Comedo-like lesions and yellowish cysts with relatively little associated inflammation most commonly affect the malar and retroauricular areas of the head and neck (see Fig. 16.13 ), as well as the axillae and scrotum. The extremities, buttocks, and trunk are variably involved. Cystic lesions can heal with significant scarring, and the condition may persist for several years following cessation of exposure. Additional findings may include hypertrichosis and grayish discoloration of the skin.
Initial management is aimed at removal of the source of exposure. Topical or oral retinoids may be beneficial, but chloracne is often recalcitrant to therapy.
Acne mechanica
Acne mechanica is due to repeated mechanical and frictional obstruction of the pilosebaceous outlet. Comedo formation is the result. Well-described mechanical factors include rubbing by helmets, chin straps, suspenders, and collars. Orthopedic causes include acne mechanica in the axillae due to the use of crutches and on amputee stumps due to friction from prostheses. A classic example of acne mechanica is fiddler’s neck, where repetitive trauma from violin placement on the lateral neck results in a well-defined, lichenified, hyperpigmented plaque interspersed with comedones. Linear and geometrically distributed areas of involvement suggest acne mechanica. Treatment is aimed at eliminating the inciting forces.
Tropical acne
Tropical acne is a follicular acneiform eruption that results from exposure to extreme heat. This can occur in tropical climates or secondary to scorching occupational environments, as in furnace workers. Historically, tropical acne caused significant morbidity among military troops. Markedly inflamed nodulocystic acne involving the trunk and buttocks is typically seen, and secondary staphylococcal infection is a frequent complication. Treatment is often of limited efficacy until the patient returns to a more moderate climate.
Radiation acne
Radiation acne is characterized by comedo-like papules occurring at sites of previous exposure to therapeutic ionizing radiation. The lesions begin to appear as the acute phase of radiation dermatitis starts to resolve. The ionizing rays induce epithelial metaplasia within the follicle, creating adherent hyperkeratotic plugs that are resistant to expression.
“Pseudoacne” of the nasal crease
The transverse nasal crease is a horizontal anatomical demarcation line found in the lower third of the nose, which corresponds to the separation point between the alar cartilage and the triangular cartilage. Milia, cysts, and comedones can line up along this fold ( Fig. 36.16A ) . These acne-like lesions are not hormonally responsive and arise during early childhood prior to the onset of puberty. Treatment consists of mechanical expression or topical therapy with a retinoid or benzoyl peroxide as needed.