INTRODUCTION
Chronic venous disease in the lower extremities affect 10% of patients worldwide, and varicose veins affect more than 20% of patients in Western countries. If left untreated, chronic venous disease can gradually progress to various complications such as ulceration and thrombosis. Endovenous thermal ablation (EVTA), such as endovenous laser ablation (EVLA) and radiofrequency ablation (RFA), have become the first-line therapy. Treatment with EVTA avoids general anesthesia, promoting faster recovery and improving patient’s quality of life. However, thermal application requires tumescent anesthesia and graduated compression stocking (GCS) after the procedure. EVTA is also associated with an increased risk to superficial nerves. Catheter-guided cyanoacrylate adhesive closure (CAC), a nonthermal, nontumescent technique, has been introduced as an alternative to EVTA, as it does not require tumescent infiltration or GCS.
N-butyl cyanoacrylate ( n -BCA) is injected intravenously, solidifying rapidly by a polymerization reaction that produces inflammation. Following entry into the target vessel, the delivered product forms a cast and adjusts to the shape of the vessel lumen. The reaction causes fibrosis of the vessel wall and permanent vessel occlusion. In the United States, VenaSeal (Medtronic, Santa Rosa, CA, United States) is the only cyanoacrylate approved by the Food and Drug Administration (FDA) for commercial use, providing a nonthermal, nontumescent alternative for closure of superficial truncal veins. The other catheter-guided system available in the United States is Varithena (polidocanol endovenous microfoam 1%) (Boston Scientific, Marlborough, MA). Catheter-guided systems available outside the United States are VenaBlock (Invamed, Ankara, Turkey), VariClose (Biolas, Ankara, Turkey), and Venex (Vesta Medical, Ankara, Turkey). The two cyanoacrylates available for percutaneous injections are VeinOff (Invamed, Ankara, Turkey) and VenaBlock. VenaSeal and VenaBlock are the two most commonly used CAC systems globally and in clinical studies. A comparison of the two systems properties is included in Table 9.1 . There are no published studies comparing the efficacy of the different CAC systems.
Table 9.1
Comparative Features of the Two Most Commonly Used Cyanoacrylate Adhesive Closure Products
| VenaBlock | VenaSeal | |
|---|---|---|
| Company | Invamed | Medtronic |
| FDA approval | No | Yes |
| Viscosity at 37°C(cP) | 20 | >1200 |
| Polymerization time | 5 s | 20 s |
| Glue delivery method | Continuous | Segmental |
| Rigidity | Relatively firm | Soft and flexicle |
| Catheter coating | PTFE | PTFE |
| FDA , Food and Drug Administration; cP , centipoise (viscosity of water is 1cP at 20°C); PTFE , polytetrafluoroethylene. | ||
Compared to VenaBlock, VenaSeal has a higher viscosity and a longer polymerization time. Polymerization occurs after 5 seconds of contact with blood and extends to 3 minutes for nearly complete polymerization. The higher viscosity of the cyanoacrylate decreases the risk of extension of the adhesive to the adjoining nontarget vessels.
PATIENT SELECTION
Similar to EVTA, a clinical history, physical examination, and duplex ultrasound (DUS) are first obtained from the patient to ensure they are an appropriate candidate for the procedure. Indications and contraindications for CAC are listed in Box 9.1 and Box 9.2 , respectively. The off-label use of CAC in the treatment of perforating veins has been reported, but further studies are needed regarding the efficacy and safety of this approach.
Box 9.1
Cyanoacrylate Adhesive Closure Indications
-
•
Clinically symptomatic venous reflux in the superficial truncal veins including GSV, SSV, and ASV
-
•
Significant reflux documented on DUS
-
•
Off-label use of VenaSeal via direct injection has been reported for the treatment of tributary veins and perforators
Box 9.2
Cyanoacrylate Adhesive Closure (CAC) Contraindications
-
•
Deep vein obstruction resulting in inadequate support to venous drainage after treatment.
-
•
History of immediate or delayed hypersensitivity reactions to acrylates and commercial or medical-grade CA preparations.
-
•
Previous adverse event to CAC, including extensive phlebitis, necrosis, or edema.
-
•
Acute venous thromboembolism (VTE), including deep venous thrombosis, pulmonary embolism, and septic thrombophlebitis.
-
•
In patients with predisposed increased risk or VTE or increased hypercoagulable state (i.e., immobility, active malignancy, or on tamoxifen), prophylactic anticoagulation should be considered.
-
•
Uncontrolled systemic inflammatory disorders, including systemic autoimmune, granulomatous, hypersensitivity, and mast cell disorders; special precaution should be taken in patients with history of sarcoidosis where known antigen or various antigens are implicated.
-
•
Granulomatous vasculitic disorders, such as granulomatosis with polyangiitis or eosinophilic granulomatosis with polyangiitis, should be considered absolute contraindications.
-
•
Acute or uncontrolled localized or systemic infection, including cellulitis of an affected leg, widespread folliculitis, and organ-specific infections.
-
•
CAC is contraindicated in the first trimester and should only be delivered in the third trimester if medically necessary and no other treatment option is available.
-
•
Due to increased risk of VTE in the immediate postpartum, venous intervention should be avoided in the first 3 months.
APPLICATION
CAC has been successfully and safely used for closure of the great saphenous vein (GSV), small saphenous vein (SSV), and anterior accessory saphenous vein (AASV). Most studies reported the treatment of truncal veins with diameters less than 2 cm. Further information is needed regarding the treatment of veins with diameters larger than 2 cm or superficial truncal veins other than GSV, SSV, and AASV. Off-label, direct percutaneous injection of VenaSeal has been reported by clinicians, but no long-term studies were found especially regarding the treatment of perforators with CAC. The catheter-guided system is described in more detail later.
Patch testing with a dermatologist and/or prick testing with an allergist can be considered prior to treatment with CAC if deemed appropriate based on a detailed clinical history. A positive patch test to acrylates is an absolute contraindication to CAC due to possible cross-reactivity between other acrylates and n -BCA. However, it is important to note that the acrylates panels do not include n -BCA, and a negative patch test result does not exclude an allergic reaction to n -BCA. Similarly, the prick testing panel does not include n -BCA.
EQUIPMENT AND TECHINQUE
The equipment and supplies common to catheter-guided CAC procedures are listed in Box 9.3 . As VenaSeal is the only FDA-approved product in the United States, the equipment and procedure details are specific to this system. CAC delivers n -BCA via a dispensing gun that is attached to a delivery catheter. The sheath and dilator are high-density polyethylene, and the delivery catheter is a polytetrafluoroethylene product. The amount of adhesive needed is a function of the vein length and diameter. The VenaSeal system provides 5 mL of glue in one package, 1.4 mL of which is wasted in the dead space of the catheter. The remaining 3.6 mL of adhesive can be used to treat up to 90 cm of vein length if the vein diameter is <6 mm.
Box 9.3
Equipment Common to Cyanoacrylate Adhesive Closure
-
•
Duplex ultrasound
-
•
Needle for percutaneous entry and introducer sheath
-
•
Dispensing catheter
-
•
3 mL syringe (to attach to a dispensing gun)
-
•
Sterile barriers, including ultrasound probe cover, drapes, gowns, gloves, masks, and gauze
-
•
Ultrasound gel
-
•
Antiseptic solution
-
•
Local anesthetic
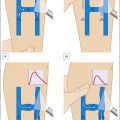
The steps common to the VenaSeal system are as follows:
-
1.
Identify access point based on clinical indication and treatment plan. Perform DUS to map the vein to be treated. Mark the proposed venous access site.
-
2.
Position the patient in supine position.
-
3.
Prep the patient for the sterile procedure, and drape the leg to be treated.
-
4.
Visualize the access site with DUS, and then local anesthetic (without epinephrine) is injected to access the target saphenous vein.
-
5.
Insert the access needle into the vein to be treated under ultrasound guidance, followed by the guidewire. Confirm intravenous placement with ultrasound.
-
6.
Insert the introducer sheath, and advance to 5 cm distal to the saphenofemoral junction (SFJ)/saphenopopliteal junction (SPJ). Flush with normal saline.
-
7.
Prime the syringe with n-BCA , and then connect to the dispenser gun and the dispensing catheter.
-
8.
Prime the catheter with n -BCA to 3 cm short of the tip.
-
9.
Insert the dispensing catheter into the introducer sheath, and pull back the sheath so that the tip of the dispensing catheter is 5 cm distal to the junction.
-
10.
Pressure with ultrasound probe is applied to occlude the SFJ/SPJ during the first two aliquots.
-
11.
Inject 0.1-mL glue aliquots by pulling the trigger of the dispenser gun, and hold for 3 seconds.
-
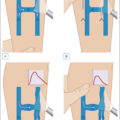
12.
Pull back 1 cm, and deliver another 0.1 mL of adhesive for 3 seconds.
-
13.
Pull catheter and sheath by 3 cm, and maintain proximal compression with ultrasound probe and light digital compression for 3 full minutes before dispensing additional adhesive.
-
14.
Maintaining proximal compression with ultrasound probe, deliver 0.1 m aliquots of adhesive at 3 -cm intervals followed by waiting 30 seconds after each subsequent trigger pull.
-
a.
For veins larger than 6 mm in diameter, consider 0.1-mL aliquots at 2-cm intervals instead of 3 cm.
-
a.
-
15.
Stop 5 cm proximal to the access site.
-
16.
Confirm vein closure with ultrasound prior to withdrawing the delivery system.
-
17.
Pull the dispensing catheter into the delivery sheath.
-
18.
With the introducer still in place, retract the catheter through the introducer until the catheter’s proximal laser mark is visible 1–5 cm outside of the introducer hub.
-
19.
Withdraw the dispensing catheter and introducer sheath, and remove the system.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


