Introduction
Approximately 8% of females experience trauma during their pregnancies. Trauma in pregnancy is the most common cause of nonobstetric-related death ; more generally, trauma is the leading cause of death in the age group under 40 in the United States. Females in their reproductive years are the population at the greatest risk of trauma. Although it is rare to see a pregnant female in the burn intensive care unit (ICU) in industrialized nations, burn trauma is a great risk to pregnant females in developing countries. Correspondingly, recent literature regarding the care of burned pregnant patients more commonly comes from journals in these developing countries and consists mainly of small studies and case reports. Burn injury during pregnancy tends to happen in the home environment. In developing countries, this may be in part attributable to the large proportion of females who attempt suicide via self-immolation.
Because of the particular paper paucity pertaining to pregnant patients, there is no great consensus on the population of burned pregnant females, size of burn disease burden in the population, or mortality of mother and fetus. , However, what does exist in the literature reveals that the maternal mortality rate exceeds 50% and has been reported at 100% when total body surface area (TBSA) burned exceeds 40% to 60%. , This statistic remains unchanged from the study by Rode et al. in 1990 showing that when TBSA was greater than 50%, maternal survival “was unlikely.” These appalling mortality data contrast with a contemporaneous study by Herndon et al. that determined the lethal burn size for 50% (LD50) of pediatric patients reached 98% TBSA burned. Despite progress made in survival rates of other burn populations, pregnant burn patients suffer the same mortality rates as in the 1960s. In a 2016 study, 60% of burned pregnant burn patients died, with an overall 50% mortality rate of the fetus. As could be predicted, fetal survival greatly depends on maternal survival, although there is a high spontaneous labor rate among burned pregnant patients. Although pregnancy does not greatly influence treatment protocols, it might factor into maternal outcomes after thermal insult, given the enormously high mortality rate of pregnant females with severe burn injury when compared with the mortality rates of nonpregnant females and males with comparable burn wound sizes. However, more study is obviously necessary.
Mortality factors
A consensus in literature exists: burn size correlates most significantly with the mortality of both mother and fetus. Large burn size is the single most predictive indicator for mortality. , , The odds of mortality of the mother rise by 1.08 per percentage of TBSA burned ( P < 0.0001). Furthermore, there is an association between mortality, TBSA burned, and the incidence of intentional burns. Females who attempt suicide via self-immolation had greater TBSA and resultantly higher mortality rates, especially those with greater than 50% TBSA burned. Rode et al. reported a direct relationship between the size of burn and the frequency rates of spontaneous abortion and premature delivery. Rezavand et al. demonstrated that, in every trimester, maternal TBSA burned positively correlated with fetal death as well as maternal demise. Agarwal found fetal loss occurred at a higher rate than maternal death even at greater maternal TBSA burned.
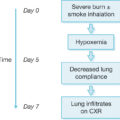
The second strongest predictor of mortality of both mother and fetus is smoke inhalation, the treatment of which remains controversial. Maternal fatalities and mothers with fetal losses were more common in those with concurrent inhalation injuries. The resultant hypoxia strongly correlates with maternal and fetal death. Closed and structural fires emit smoke potentially imbued with cyanide (CN) and carbon monoxide (CO) gases. Upon inhalation, CO and CN demonstrate synergistic effects; furthermore, they concentrate at higher levels in the fetus than the mother as fetal hemoglobin binds CO and CN more avidly than maternal. As such, providers must treat two patients with awareness of potential effects of CO and CN poisoning on both mother and child. Facial burns, large burns, and self-inflicted, intentional burns all strongly associate with inhalation injury. Significant thermal injury in the pregnant patient population can have not only direct but also indirect effects on the pulmonary system. Unique to the pregnant burn patient, vital lung capacity decreases while mucosal edema, oxygen consumption, and minute ventilation increase. As with the severely burned nonpregnant patient, should a pregnant burn patient be suspected of suffering from inhalation injury, emergent intubation ought to be instituted. Given the known physiologic changes of pregnancy, which are compounded by burn edema, early intubation in the severely burned pregnant patient should be strongly considered. Hydroxycobalamin, the cyanide antidote recommended in Chapter 26 , is a pregnancy category C drug and should only be used if the benefits outweigh the risks because cyanide crosses the placenta and will poison the fetus to a greater extent than the mother. ,
Gestational age was also a factor reported in several studies. , Argawal found fetal survival in the third trimester correlated less to maternal survival but rather strongly to gestational age. Liu determined gestational age-specific risk of birth to be greater among the population of injured mothers than noninjured in each gestational week until week 38, irrespective of medical condition. Gestational age is not the sole criteria for neonatologists and obstetricians in determining viability of a fetus. The fetal weight benchmark of 500 g has been adopted, which is the lower size limit at which intubation is feasible. , Given the potentiality of obstetric intervention, it is imperative to precisely ascertain the gestational age and weight of the fetus via fetal ultrasound and menstrual and sexual patient history data early in the management of acute burns.
Hypovolemic shock and sepsis have also been found to be complications resulting in maternal and fetal death. Recurrent septicemia is a major challenge in the management of a severely burned obstetric patient. Intraabdominal hypertension and abdominal compartment syndrome develop in most severely burned patients within 48 hours of injury. Intraabdominal hypertension is present when intraabdominal pressure measures in excess of 12 mm Hg, and abdominal compartment syndrome exists when intraabdominal pressure is greater than 20 mm Hg, particularly if additional organs display dysfunction. Pregnancy induces physiologic changes in all major maternal organ systems, mimicking early perturbations seen in multisystem organ dysfunction (MOD). All these complications potentially lead to MOD, compounding the existing state present in the pregnant population and further jeopardizing severely burned obstetric patients.
Fetal viability
Managing obstetrical complications provides an additional challenge to the burn team. Second to death of the mother, placental abruption is the most common cause of the death of the fetus after trauma. Because of the intense kinetics undergone by a pregnant patient postburn, the fetus often spontaneously delivers. In layman’s terms, this is a miscarriage. Consistently, studies show that fetal mortality rates are highest during the first trimester in the setting of major burns. , However, with aggressive fetal monitoring, appropriate obstetrical intervention can preserve the life of the fetus earlier in pregnancy. Studies indicate this approach starts approximately in the 22nd week of gestation. Determining the gestational age and weight , of the fetus enables the healthcare team to most effectively guide this care. In a large study, Linder et al. demonstrated that early-preterm, low-risk deliveries increased the risk of fetal complications with higher rates of neonatal ICU (NICU) admission, sepsis, and antibiotic treatment compared with late-term neonates or the gestational control population. Although the study only began evaluation at gestational week 37 of low-risk singleton deliveries, it did show that neonatal morbidity risk corresponds with early-term deliveries. The burn, obstetric, and neonatal teams must collectively weigh the risks of preterm delivery against the risks of the fetus remaining in utero besieged by the expected effects of severe burn trauma.
Practical management algorithm
Adverse pregnancy outcomes are not associated with incidents of minor trauma during pregnancy. However, severe burns are major trauma. As a practical matter, management of the pregnant burn patient can be divided into five phases: previablity, periviability, early viability, viability, and term ( Table 28.1 ). Obstetrical complications (e.g., uterine rupture and placental abruption) are potential mechanisms of preterm delivery after acute maternal trauma. During the period of previability, defined as the period in the pregnancy from conception to gestational week 22 or 23 , , and a fetal weight of less than 500 g, the fetus cannot survive independent of the mother. Although the previability stage of pregnancy is currently defined at gestational week 24 by the American College of Obstetrics and Gynecology, neonatologists and maternal-fetal medicine specialists have extended the gestational age of periviability to 22 weeks. However, this is dependent on a fetus of 500 g. , , Most obstetricians will attempt resuscitation at 22 weeks, but 24 weeks and 500 g remain the benchmark for viability because fetal mortality at 22 weeks remains incredibly high. Providing total burn care to the mother makes the womb the optimal incubator, thereby managing fetal care as best as possible. The data indicate that there is a high spontaneous abortion rate ; however, there is no proven advantage to performing a termination of the pregnancy unless maternal death seems likely otherwise. Effort should be exerted to avoid medications known to be hazardous to the fetus but not to the extent that the mother succumbs to shock and/or sepsis, which have very high rates of fetal loss.
Table 28.1
Indications for Emergent Caesarian Section in the Setting of Severe Burns when the Fetus Is in Distress
| FETAL DELIVERY IN THE SETTING OF SEVERE MATERNAL BURN | ||
|---|---|---|
| Fetal Stage | Gestational Age | Delivery Indicated |
| Previability | 0–21 weeks | No |
| Periviability, weight < 500 g | 22–26 weeks | No |
| Periviability, weight ≥ 500 g | 26–28 weeks | Yes |
| Early viability | 26–28 weeks | Yes |
| Viability | 28–32 weeks | Yes |
| Preterm | 32–37 weeks | Yes |
| Term | 37–40 weeks | Yes |
The multidisciplinary team must balance burn care among several factors during periviability (22–26 weeks) and early viability (26–28 weeks). Prophylactically, antenatal corticosteroids should be administered upon admission in the setting of a severely burned obstetric patient. Demonstrated to be the optimal interventions to reduce morbidity and mortality in premature neonates, these also promote organ growth , and can be administered for fetuses as young as 23 weeks. , Betamethasone (two 12-mg doses given 24 hours apart) and dexamethasone (6 mg every 12 hours in four doses) are the most commonly used antenatal corticosteroids. , There is no benefit to shorter dosing intervals, and it is recommended that the first dose be applied even if administration of a second dose is unlikely. However, antenatal corticosteroids remain contraindicated when the risk to mother and child is greater by prolonging the pregnancy than is emergent delivery. Effective to forestall labor for up to 48 hours, tocolytic therapy is particularly useful in situations needing to delay labor until after the administration of antenatal corticosteroids or transfer of the patient to an appropriate burn center. , In the setting of severe burns, tocolytic therapy may be indicated before viability to inhibit contractions incited by intraabdominal surgery. , Many different drug classes have been employed (e.g., calcium-channel blockers, β-mimetics, and magnesium sulfide), but a study in 2015 showed prostaglandin inhibitors to be the optimal first-line tocolytic agents to delay labor with the lowest maternal side-effect profile. Calcium-channel blockers potentially have the best neonatal outcomes of the tocolytic therapies. , Although traditionally used to inhibit acute preterm contractions, predelivery administration of magnesium sulfate conveys neuroprotection , and has been shown to be ineffective as a tocolytic agent. Transdermal nitroglycerin for pregnancies of less than 28 weeks is not recommended because of its significant side-effect profile. Because these medications can exacerbate the burn shock besetting a patient, coordination among critical-care clinicians, obstetrics, neonatologists, and pharmacists is critical to guide therapy and avoid further risk to mother and child.
The dilemma of delivery and resuscitation must be measured against the fetus’s odds of survival and chances of leading a normal life. If the perceived risk to the child remaining in utero exceeds the risk in the NICU, the infant should be delivered and cared for ex utero. During in utero critical care, the fetus must be monitored and medications chosen to avoid fetal harm. If toxic medications must be given, the risk should be balanced against the risk of fetal harm. Additionally, if intrauterine fetal death results, irrespective of the reason, the uterus should be evacuated. Retained stillbirth, septic abortion, and missed abortion can lead to disseminated intravascular coagulation (DIC). , Correlating with high rates of maternal morbidity and mortality, DIC induced by fetal loss is best prevented by prompt evacuation of the dead conceptus. , It is ethically reprehensible to attempt resuscitation on a child who has or will soon perish regardless of measures taken.
Treatment
It is widely acknowledged that burn patients suffer from altered pharmacokinetics that make them unique among trauma patients. Although it could be presumed the treatment protocols would alter significantly given the fetus, they do not ( Fig. 28.1 ). Early wound excision and coverage, aggressive fluid resuscitation, antibiotic administration (though limited in options), and sufficient nutrition are the foundation of managing burned pregnant patients. However, emergency responders and the burn team may be unaware a patient is pregnant. Thus the first simple and requisite precaution in treating reproductive-age female burn patients is to suspect pregnancy until proven otherwise. Immediately upon determination of pregnancy, high-risk obstetric consultation must be sought, even before excision of the wound. Fetal heart tones must be established and an ultrasound performed to corroborate gestational age obtained from patient menstrual history to determine fetal viability. If the fetus is deemed viable, administer antenatal corticosteroids to mature the lungs for delivery, regardless if the fetus displays signs of distress. This also delays delivery, enlarging the time for stabilization and prep of the mother, and it improves outcomes for the child. After these consults and corticosteroid treatments, initiate antibiotic therapy and coagulopathy support before wound excision and/or emergent delivery.
Algorithm of the optimal treatment of the burned pregnant patient.
TBSA , Total body surface area; NICU , neonatal intensive care unit.
As with nonpregnant burn patients, early wound excision is key in managing severely burned pregnant patients. Surgical interventions include escharotomies, as indicated, and coordination with an obstetrics team if fetal distress is evident. The burn team must proceed with the awareness that two patients require care. Studies have demonstrated that maternal demise strongly correlates to fetal death. We advocate early excision of abdominal eschar to prevent abdominal compartment syndrome and decrease the risk of infection. Should the fetus be viable and in distress, excision of the burn wound can proceed immediately upon delivery. However, early wound excision with fetal survival is rare in the setting of major burns. If early wound excision is indicated and the fetus is not of gestational age or sufficient weight to support emergency caesarean section (e.g., at least 22–24 weeks by either ultrasonographic measurements and/or patient history of last menstrual period , and measured fetal weight of 500 g by ultrasound ), published data and our experience indicate that the mother will not carry the fetus to term. The best chance of both fetal and maternal survival is to deliver the fetus upon signs of distress and manage the maternal burn injuries. If the fetus shows no signs of distress, proceed with early excision and wound coverage and monitor the fetus. In this setting, should the fetus become distressed, perform an emergent caesarean section. If the fetus does not display distress, the mother remains the best incubator, but diligent monitoring is required. Even if the fetus is not viable gestationally, the burn team must proceed with the burn wound excisions because the mother would be subjected to an unacceptable risk of shock and sepsis. The care of the mother must take precedence over that of the child.
The anatomic and physiologic changes brought about by pregnancy drastically increase the difficulty in the anesthetic, obstetric, and surgical management of burn patients. “Normal” vital signs and labs in pregnant patients sometimes differ from those of nonpregnant individuals. Current early warning system triggers used to evaluate deteriorating patients are based on nonpregnant values and thus require refinement for the pregnant population. Therefore awareness of the differences and consultation with appropriate specialists are fundamental to proper care. The changing cardiovascular profile includes increases in cardiac output, uterine blood flow, and blood volume as the fetus matures. Crucially, pelvic blood flow autoregulation is absent because pregnancy maximally dilates the uterine vasculature. Resultantly, uterine blood flow depends solely on maternal mean arterial pressure. Furthermore, dilutional anemia of pregnancy may complicate assessments of blood loss and sufficiency of the oxygen-carrying capacity in burn patients. Aggressive fluid resuscitation is vital in the early stages of maternal and fetal salvage. Early interventions during resuscitation include close monitoring of hemodynamics and perfusion indices to evaluate how those respond to initial resuscitation. We further recommend institution of a Foley catheter, central venous catheter, and an arterial line with advanced hemodynamic monitoring upon admitting a severely burned obstetric patient to determine adequate volume status and perfusion. The approach to fluid resuscitation remains the same in the pregnant population as in the nonpregnant group, with the goal to support fluid and plasma loss, early recognition of hypoperfusion, and prompt management of shock while avoiding hypoxia. We use a modified Parkland formula to begin resuscitation at 3 mL/kg/TBSA burned and titrate accordingly, with a targeted urine output of 0.5 mg/kg/h. Careful monitoring of hemodynamics as well as of blood pressure, hematocrit, and heart rate should tailor resuscitation. Interestingly, one recent case report suggested that it is optimal to decrease the infusion volume of fluid resuscitation, especially after the delivery of the fetus, should that be necessitated, but this has yet to be corroborated. After the 8th week of gestation, pregnant females should present with physiologic dilutional anemia, which, if absent, is an early marker of hemoconcentration (Hg > 13 g/dL) and hypovolemia. During the third trimester, instituting an intraabdominal bladder pressure monitor for resuscitation is a necessary precaution to monitor those patients receiving in excess of 5 mL/kg/TBSA burned. The inability to accurately and timely assess for intraabdominal hypertension and compartment syndromes in severely burned pregnant patients presents an additional challenge to the burn team. Care must be taken to ensure the pregnant patient does not develop acidemia, hypoperfusion, hypoxia, or thromboembolic complications stemming from high levels of coagulation factors common to pregnant females. Supportive modalities include serial electrolyte and hematologic monitoring to support normalization of electrolyte levels, monitoring of hemoconcentration and fluid balance, and maintaining normothermia. Should such complications arise, the life of the fetus could be jeopardized. When that occurs, a review of the literature reveals that the pregnancy most often spontaneously aborts. , , Should obstetrical intervention be indicated, such action must be taken expeditiously to preserve the lives of both mother and child. However, greater study is merited to determine the most efficacious triggers for obstetrical intervention as well as the optimal amount for fluid resuscitation.
The U.S. Food and Drug Administration (FDA) classified drug recommendations by five grades (A, B, C, D, and X) according to the possible side effects for the fetus when administered to pregnant and/or lactating females ( Table 28.2 ). Animal studies showed no adverse reactions to grade B drugs (e.g., macrolides, cephalosporins, penicillins, lincomycin, and clindamycin), and these are presumed safe to treat pregnant patients. In fact, benzylpenicillin remains the most common antibiotic administered to pregnant females. Categories C, D, and X have been demonstrated to generate negative side effects in fetal development. In cases where the benefits of treating a pregnant female with a grade C drug, such as quinolones and fluconazole, greatly outweigh the risks associated with the drug or no alternative exists, they are warranted for use in pregnant females. Drugs belonging to class D rarely warrant administration—only if the risk of harm is strongly outweighed by the benefit. Category X should only be administered in instances where fetal loss is assured or an accepted ramification exists for using the medication to preserve the life of the mother. Adding to the complexity, recommendations vary depending on trimester or for a lactating burn patient. As part of the multidisciplinary team, the clinical pharmacist plays an integral role in assuring safe and effective pharmacologic therapy for each patient in the burn unit. A pharmacist should be knowledgeable and current on the changing recommendations of all drugs safe for administration to pregnant and nursing patients, from antibiotics to renal doses. Therefore the clinical pharmacist is indispensible in advising the team on the optimal therapy for burned pregnant patients.
Table 28.2
Available Pharmaceuticals for Pregnant and Lactating Females and Their Recommendations
| DRUG RECOMMENDATIONS FOR PREGNANCY AND/OR LACTATION IN BURN PATIENTS | ||||
|---|---|---|---|---|
| Drug | Pregnancy Category | Pregnancy Recommendations | Lactation Recommendations | Comments |
| A. Topicals | ||||
| Bacitracin-like products | C | Compatible | Compatible | Limited fetal exposure would be expected after topical use |
| Dakin solution (Na hypochlorite 0.125%, 0.25%, 0.5%) | _ | May use during pregnancy; no human data available; risk for fetal harm not expected based on limited systemic absorption | Safety unknown; inadequate literature available to assess risk; caution advised | |
| Mafenide | C | No human data; should not be withheld because of pregnancy | No human data | |
| Miconazole | C | Avoid vaginitis treatment in the first trimester or application to large areas at any time during pregnancy | ||
| Mupirocin | B | No human data; probably compatible | No human data; probably compatible | |
| Nystatin | C | Compatible | Compatible | |
| Silver nitrate | C | None | No human data | |
| SSD | B | No recommendations | ||
| B. Antibiotics | ||||
| Aminoglycosides | D | Human data—LR | Compatible | Streptomycin linked to hearing loss in newborns and should be avoided, unless specific benefit established. Short-term use of others in class acceptable with monitoring, if benefits outweigh the risk |
| Penicillins | B | Compatible | Compatible | Generally safe to use |
| Carbapenems (meropenem) | B | Probably compatible | Probably compatible | Use with caution only when penicillins or cephalosporins not an option |
| Cephalosporins (all generations) | B | Compatible | Compatible | Generally safe to use; use ceftriaxone with caution at term because of risk for kernicterus |
| Clindamycin | B | Compatible | Compatible | Appears to be safe and effective |
| Daptomycin | B | Limited human data; animal data—LR | Limited human data; probably compatible | May use if benefits outweigh risks |
| Vancomycin | B | Compatible | Limited human data; probably compatible | Safe and effective |
| Metronidazole | B | Human data—LR | Hold breastfeeding (single dose); see comments | Contraindicated first trimester; lactation is potentially toxic for divided dose; “topical” metronidazole should be avoided |
| Linezolid | C | Compatible | No human data; potentially toxic | May use if benefits outweigh risks |
| Sulfamethoxazole, trimethoprim | C | Human data suggest risk in third trimester | Limited human data; potentially toxic | Avoid in first trimester because of major congenital malformations. Sulfamethoxazole should be avoided after 32 weeks’ gestation because of risk for kernicterus |
| Tetracyclines | D | Contraindicated in second and third trimesters | Doxycycline; compatible | Should be avoided |
| Tigecycline | D | Contraindicated in second and third trimesters | Limited human data; probably toxic | Avoid in pregnancy unless benefits outweigh risks |
| C. Antifungals | ||||
| Fluconazole | D/C | Associated with fetal mortality and congenital abnormalities | Compatible | |
| Posaconazole | C | Animal data suggest risk of skeletal malformations | No human data; potential toxicity | |
| Voriconazole | D | Animal studies have demonstrated fetal harm | No human data; potential toxicity | |
| Micafungin | C | Animal data revealed embryotoxic effects but have not been replicated in adults | No human data; probably compatible | |
| Amphotericin | B | Observational data suggest rate of human birth defects is similar to that of the general population | Not recommended | |
| D. Pain Medications | ||||
| Codeine | C | Human data suggest risk | Limited human data; probably compatible | Although the AAP has classified codeine as compatible with breastfeeding, data suggest that, for some females, codeine can not be considered safe during nursing, especially if therapy is >1–2 weeks |
| Fentanyl | C | Human data suggest risk in third trimester | Compatible | Neonatal withdrawal, respiratory depression |
| Hydrocodone/Acetaminophen | C | Human data suggest risk in third trimester | Limited data; potential toxicity | |
| Morphine | C | Human data suggest risk in third trimester | Limited human data; probably compatible | |
| Oxycodone | C | Human data suggest risk in third trimester | No human data; probably compatible | |
| Tramadol | C | |||
Related posts:
 A brief history of acute burn care management
A brief history of acute burn care management
 Treatment of infection in burn patients
Treatment of infection in burn patients
 Respiratory care
Respiratory care
 Hematology, hemostasis, thromboprophylaxis, and transfusion medicine in burn patients
Hematology, hemostasis, thromboprophylaxis, and transfusion medicine in burn patients
 Acute renal failure in association with thermal injury
Acute renal failure in association with thermal injury
 Critical care in the severely burned: Organ support and management of complications
Critical care in the severely burned: Organ support and management of complications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


