Introduction
Many small burn injuries can be treated in the outpatient clinic once it is determined that there are no other injuries, complicating medical problems, or suspicion of abuse. As with burn care in the hospital setting, the goals of outpatient burn care are to adequately heal wounds with minimal scarring or deformity, reduce pain and the risk of infection, and decrease impaired function. To achieve these, outpatient burn care encompasses wound management, rehabilitation, and psychosocial support, as well as involving family and other social support systems.
Outpatient burn care can also extend to follow-up treatment of patients with larger burns after discharge. Care for these patients is similar, with evaluation for proper healing wounds and monitoring for areas that may need surgical revision, along with ongoing physical and psychosocial therapy and scar control management.
Who can be managed as an outpatient?
The American Burn Association (ABA) provides guidelines to assist in identifying patients who should be referred for treatment at a burn center, which will be discussed in more detail later ( Table 5.1 ). Careful medical history and physical examination will help to guide your decision-making as to whether the patient should be admitted or can be treated as an outpatient. Patients should be carefully evaluated to determine whether outpatient management of the burn would be sufficient for the course of medical treatment that your institution can provide. Crucial factors to note include the extent and depth of burn injury, cause of the burn, associated trauma, and premorbid diseases. Patients who require intravenous (IV) fluid resuscitation should be treated in the inpatient setting, as should those for whom it will be difficult to effectively manage pain as an outpatient. However, once resuscitated and pain is controlled with oral pain medication, subsequent treatment may be performed in the community setting depending on the severity of the burn injury.
Table 5.1
American Burn Association Burn Center Referral Criteria
Image provided with permission from the American Burn Association. All rights reserved.
| Immediate Consultation with Consideration for Transfer | Consultation Recommendation | |
|---|---|---|
| Thermal burns |
|
|
| Inhalation injury |
|
|
| Pediatrics (≤14 years or <30 kg) |
|
|
| Chemical injuries |
|
|
| Electrical injuries |
|
|
TBSA, Total body surface area.
Percent of the burn
The ABA recommends referral to a dedicated burn center for all patients with greater than 10% partial-thickness total body surface area (TBSA) burn, or any percent of full-thickness burn. The TBSA may be estimated by using the Wallace rule of nines, or the rule of palm, which estimates the body surface area involvement by using the size of the patient’s palm and fingers, with the thumb extended and all fingers adducted as a guide to estimate approximately 1% of the TBSA for that patient. The rule of palm is useful especially in children, who because of their body proportions do not follow the rule of nines. A more accurate method of estimating burn size is the Lund-Browder chart. It is important to note that hand size may overestimate the size of the burn, and both the rule of nines and the Lund-Browder chart may have significant error when estimating the burn size of obese patients. , Therefore it is important to understand that these methods of determining burn involvement are not exact and to know the limits of your facility and staff. No matter the size of the burn, however, all pediatric patients may benefit from referral to a burn center.
Depth of the burn
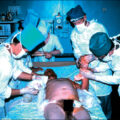
The depth of the burn injury is important to note during the evaluation of the patient because it is recommended that any patient with a third-degree burn be referred to a burn center because of the additional care needed. First-degree burns and third-degree, full-thickness burns are relatively easy to identify at the time of presentation except for perhaps in scald injury. First-degree burns, like sunburns, only involve the epidermis and are dry, painful, and do not blister. Third-degree burns involve the epidermis, dermis, and the subcutaneous tissues. These wounds can appear black, white, or leathery, and they will not blanch to the touch or be sensate or painful ( Fig. 5.1 ). It is still possible to elicit pain because manipulation of a full-thickness burn may stimulate the edges of the burn, which are inflamed and sensate. Second-degree burns can be divided into superficial partial-thickness and deep partial-thickness injuries. The difference between these two can be subtle during the initial evaluation. All partial-thickness burns will be painful, moist, and can have blisters ( Fig. 5.2 ). However, superficial wounds will have clear fluid in blisters, and deeper wounds may have bloody fluid with late presentation. Superficial wounds will also blanch to pressure as opposed to deeper wounds. Occasionally, wounds that appear perfused with ruptured blisters that initially appear to be superficial may progress to a more severe injury due to thrombosis of the small blood vessels in the wound, leading to the wound becoming a deeper injury. , Superficial partial-thickness wounds will heal within 2 weeks, whereas deep partial-thickness wounds may take longer to heal or require excision and grafting. Scald injuries can appear to be red when they are full-thickness, but are still insensate and dry. A scald burn occurs when the skin is damaged by contact with hot liquid or steam. This is the most common type of burn in young children, who have thinner skin and are more likely to burn. Although scalds are usually accidental, they can also be intentional. In fact, they are the most common cause of intentional burns seen in children. The pattern of distribution of the burn is an important factor in determining etiology of the burn. Also, the account of how the burn occured must fit both the abilities of the child and the distribution of the burns. If there is any doubt if the burn is accidental or not, the patient should be referred to a burn center as intentional scald burns are associated with greater morbidity and mortality.
Third-degree burn. Note the leathery appearance of this burn.
Second-degree burn.
Burn injuries can be divided into three zones ( Fig. 5.3 ). At the point of greatest damage is the zone of coagulation, in which there is irreversible tissue damage. Surrounding this is the zone of stasis, an area of the wound that can potentially necrose with inadequate treatment or heal if the area is properly perfused. Should the patient be underresuscitated, this region of the burn wound may progress to become part of the zone of coagulation. The third zone, at the edge of the burn injury, is the zone of hyperemia, which will likely heal with treatment if the region maintains perfusion and infection is not involved.
Zones of injury.
Distribution of the burn
According to ABA guidelines, burns involving the hands, feet, face, genitalia, and perineum, and those that cross major joints should also be treated in a burn center. Lasting damage to these areas can have a severe impact on patient outcomes. Impairments to the hands can affect grip and can therefore have deleterious effects on the ability to work or handle activities of daily living. Burns of the feet or those that cross joints can severely limit mobility, whereas burns to the face can impair vision and the ability to eat, as well as have an emotional impact due to altered appearance. Finally, burns to the genitalia and perineum can restrict patient autonomy, hindering urinary and sexual function or the ability to defecate. Although burns to these areas may not necessitate specific inpatient treatment, they should be treated at a burn center with the proper resources to handle the special reconstructive and rehabilitative needs of these patients.
Special consideration should be given to burns that are completely circumferential around a part of the body, such as a limb or the trunk. Because the tissues beneath the wound become edematous, circumferential wounds can cause increased pressure, resulting in compartment syndrome and leading to ischemia. The classic symptoms are the five Ps, which are pain, pallor, paresthesia, pulselessness, and paralysis. The physician should have a high index of suspicion for compartment syndrome, which necessitates inpatient treatment.
Injuring agent
Electricity
All patients exposed to high-voltage electricity should be referred to a burn center because of increased deep-tissue injury and subsequent increased amputation rates, organ failure, and mortality as compared with patients with comparable TBSA thermal burns. Fatal cardiac dysrhythmias are a major risk after electrical injury; therefore all patients with electrical injuries should have an electrocardiogram (ECG) performed, and all meet the criteria for referral to a burn center. Additionally, bony tissue is noted to have higher resistance leading to increased heat from electrical injury; therefore these injuries may have burned tissue adjacent to bone despite superficial tissue appearing normal. Injuries due to low voltages are usually smaller; therefore these patients, as long as no ECG abnormalities are present and no loss of consciousness occurred, can be treated as outpatients should there be no other indication for admission. The presence of dysrhythmia, ECG abnormalities, or a history of loss of consciousness is grounds for admission to the hospital for monitoring. A common means of injury from low-voltage energy sources is that of children sucking on a defective electrical cord, resulting in damage to the lips, tongue, gums, or dentition. Such patients may need admission because oral intake may be hindered. Such injuries to the mouth are at risk of resulting in rupture of either the superior or inferior labial arteries, especially from days 4 through 7 post burn ( Fig. 5.4 ). If treating as an outpatient, the caregiver should be educated on this risk and instructed in proper first aid, which consists of pinching the labial commissure between the index finger and thumb.
Labial burn.
For patients with low-voltage injuries who can be treated as outpatients, consideration should be made for follow-up with a burn center for delayed symptom onset, including vision problems.
Chemicals
Although not caused by thermal injury, chemical burns are treated by burn surgeons, and chemical injury is one of the criteria for referral to a burn center. Initial management of a patient with a chemical injury involves brushing off dry chemicals and copious flushing of areas affected by wet chemicals. , The authors recommend flushing until the patient is pain free, and, with alkaline exposure, until the skin pH is 7, which is the pH of water. The normal skin pH is around 5, but once the pH has reached 7, further injury seems unlikely. As with thermal injuries, prompt irrigation of chemical injuries results in decreased full-thickness injury and shorter hospital stays. Irrigation of the chemical burn may need to continue in excess of 1 hour. In the authors’ experience, it often takes longer in alkaline exposures to reach a pH of 7.
Specific considerations need to be made depending on the causative substance. Phenol compounds do not flush well with water, so polyethylene glycol or vegetable oil followed by water lavage may be used. Water needs to be avoided if metallic sodium or potassium is suspected because the resultant exothermic chemical reaction may worsen the burn injury. Hydrofluoric acid injuries are treated with calcium after water lavage, and a calcium gel can be used to cover the injury. Some recommend that the tissues should be injected with calcium gluconate to alleviate pain and to prevent tissue necrosis. The authors use intraarterial calcium gluconate, slowly injecting into the artery supplying the affected part until the patient is pain free. This may have to be repeated in a few hours. Dermal exposure to hydrofluoric acid results in the absorption of the dissociated fluoride anion and subsequent insoluble salt formation by binding with calcium and magnesium. The patient may then develop hypocalcemia and hypomagnesemia, accompanied by hyperkalemia due to potassium efflux from cells. Hypocalcemia is the main cause of death after hydrofluoric acid poisoning via the induction of fatal dysrhythmias. As little as 1% TBSA exposure to 50% concentration hydrofluoric acid or 5% TBSA exposure to any concentration is enough to result in potentially fatal hypocalcemia, therefore initial ECG and measurement of serum electrolytes is indicated. Identification of the chemical and communication with local poison control centers is recommended if needed. After the appropriate removal of the causative chemical, treatment is the same as for any other wound.
Contact with gasoline is another cause of chemical burn because of the hydrocarbons present in the gasoline causing epidermal and dermal damage. These hydrocarbons may be absorbed, causing systemic effects including central nervous system (CNS) impairment, pulmonary hemorrhage and edema, pneumonitis, cardiac dysrhythmia, and liver and kidney dysfunction. In patients who are exposed to gasoline, all gasoline-soaked garments should be removed and the gasoline copiously irrigated with water, as with other chemical injuries.
Respiratory complications
Inhalation injury is one of the criteria for referral to a burn center, and the physician must have a high index of suspicion concerning inhalation injury and carbon monoxide poisoning based on the circumstances surrounding the burn injury because there may be little to no exterior sign of injury. , The sequelae of both of these complications may not be present initially and may develop over time. Of note, airway obstruction may occur after burns of the oropharynx, face, or neck as the tissues of the upper airway become edematous. Therefore observation is warranted if there is any suspicion of inhalation injury. Any patient involved in an enclosed fire needs to be admitted and observed because of the increased presence of toxic chemicals released in the fumes of burning furniture or appliances.
Associated trauma
Because of the often accidental nature of burn injuries, there is frequently concomitant trauma at the time of presentation. Assessment should be made whether the associated trauma or the burn injury is of greater threat to the patient’s morbidity or mortality, with the decision of the need for direct admission or stabilization and referral to a burn center made at the discretion of the treating physician.
Comorbid disorders
A comprehensive medical history of the burned patient should be performed to identify those with preexisting medical conditions that would complicate the ability to properly care for the patient in a community setting or have an impact on recovery, morbidity, and mortality.
The stress of the burn may exacerbate previous medical conditions such as diabetes mellitus, asthma, or coronary artery disease.
Social circumstances
Proper outpatient management of burns requires that there are sufficient resources available to care for the wound and provide for proper follow-up care. Resources include family members or visiting nurses, who can assist with dressing changes, and access to medical care, proper rehabilitation, and psychosocial services. Should these resources be unavailable to the patient in the community setting, referral to a burn center should be considered.
Of serious concern when considering the social circumstances surrounding the patient is the possibility that the injury was nonaccidental. If there is any suspicion that the injury to the patient was intentional, admission to the hospital and notification of the proper agencies is warranted for their protection ( Figs. 5.5 and 5.6 ).
Nonaccidental burn. Note the area that is not burned on this child. She was held down in a tub of hot water. The area of the buttocks that is not burned was in contact with the bottom of the tub and the heat had dissipated, thus not burning the child.
Nonaccidental burn. This burn was caused by a clothes iron; note the triangular shape.
Hospital resources
Available resources should be taken into account in the decision-making process. All pediatric burn patients should be referred for treatment at burn centers with qualified personnel and equipment to treat children.
Management of minor burns
Cooling the burn
First aid for burn wounds should begin with removing clothing from the burned area and subsequently cooling the wound with cool, running tap water or saline. The burn wound should be cooled as close to the time of injury as possible because damage continues while the tissue remains above 44°C. A study by Rajan et al. has shown that even cooling initiated 60 minutes after burn injury will still have a beneficial effect on burn wound outcomes. Excessive cooling, such as through the use of ice, may actually result in a deeper wound when compared with uncooled burn wounds in an animal model.
Cooling is also important in the first aid of thermal injuries because cooling stabilizes mast cells in the skin, resulting in decreased histamine release and subsequent reduced edema of the burn wound. The application of cool, moist compresses can also be effective in relieving the pain associated with partial-thickness burns. Whereas patients with large surface area involvement may experience hypothermia if too aggressively cooled, patients who are eligible to be treated as an outpatient, with a smaller TBSA, should have little risk of this occurring. It is still prudent to monitor the patient’s core temperature during active cooling.
A limit to the surface area that is cooled is arbitrary, but a practical limit is about 10% of the TBSA. A study concluded that 20 minutes was the optimal time to cool a burn. In a human model, cooling for 20 minutes was shown to salvage 25.2% of the dermal thickness of burn injury compared with burns that were not cooled.
Pain control
First-line treatment for pain in the emergency setting is usually narcotics. IV doses of morphine can be given incrementally to titrate for the desired effect. Other pain relief options include acetaminophen with codeine, oxycodone, or similar analgesics that can be used individually or in combination. However, because of growing concerns about the overuse of opioids and the risk of addiction and overdose, the physician may consider the use of medications such as acetaminophen or nonsteroidal antiinflammatory drugs, especially in smaller burns that are more appropriate for outpatient management. The use of anticonvulsants like gabapentin and pregabalin can help modulate the pain response and make the patient more comfortable. Partial-thickness wounds are the most painful burn wounds because the injury leaves the wound without the epidermis. The pain is severe initially, but will partially subside in the ensuing hours. During dressing changes or physical activity when the wound is manipulated, pain will again be exacerbated. Wounds with eschar will not be painful, unless the eschar is removed or separated, exposing the viable tissue beneath. Therefore additional analgesia may be required during physical activity and dressing changes. Should oral medication be unable to control the patient’s pain, the patient should be admitted for adequate pain management. Additional information on management of pain in the burn patient is discussed in later chapters.
Blisters
There is no clear consensus on the management of blisters; therefore treatment depends on the experience of the burn care team. Options for blister management include leaving the blister intact, removing the blistered skin during the initial wound care, removing the blister at a later time, or aspirating the fluid from the blister. Laboratory studies suggest that blister fluid may have detrimental effects via suppression of immunologic responses and inhibited fibrinolysis. Others advocate that the blister can be left intact to serve as a biological wound dressing, with spontaneous resorption of the blister fluid beginning within 1 week. The devitalized skin from a ruptured blister can also be left in place in a similar fashion to serve as a biological dressing. If blisters are open or are removed, it is generally recommended to cover the injury with a type of protective dressing. The authors remove blisters that are deemed likely to rupture on their own and leave others intact, covering them with an antimicrobial dressing.
Cleansing the wound
For thermal injuries, cleansing of the burn wound should be performed using room temperature to tepid (100°F) sterile water or normal saline with a mild soap. In injuries involving tar or asphalt, cooling should be performed, and the solidified tar or asphalt should be removed through the use of a solvent. Solvents with affinity for the substance to be removed should be used. One such product is Medi-Sol Adhesive Remover, a nontoxic, nonirritating, citrus-based category I medical device solvent approved by the US Food and Drug Administration (FDA) that has been shown to be effective in the removal of both tar and asphalt. Other options include polysorbates (a class of emulsifiers), which can be used on their own or in conjunction with topical antibiotics, and topical antibiotics in petroleum jelly. However these options may require multiple applications to be effective. , The authors prefer the use of mineral oil because it is inexpensive and works well without causing additional skin irritation.
Topical agents
Antibacterial agents are used to prevent burn wound infections. Prophylactic use of topical agents such as these have not shown benefit in preventing infections or septicemia versus other dressing options, such as petrolatum-impregnated gauze , ; however, the authors recommend that these substances be used when the physician has suspicion that an infection is present. Should topical antimicrobial agents be warranted, there are several options available. A popular agent used in the treatment of burn wounds is 1% silver sulfadiazine, which has antiseptic properties due to the presence of silver but also results in delayed wound healing. , This delay in wound healing has been shown to be alleviated through coadministration of nystatin or aloe vera in an animal model. Use of silver sulfadiazine should be discontinued once reepithelialization is noted because it impairs epithelialization. If the wound is covered with eschar, however, silver sulfadiazine may be used with few side effects. Care must be taken that the patient is not allergic to sulfa products or that the patient is not pregnant, nursing, or an infant under 2 months old because of the risk of kernicterus.
Combinations of antibiotics in ointments have been of increasing interest because there have been no noted effects on wound healing in these medications. Examples include triple antibiotic ointment (containing neomycin, bacitracin zinc, and polymyxin B sulfate) and Polysporin (containing polymyxin B sulfate and bacitracin zinc), both of which have coverage against gram-positive cocci and some aerobic gram-negative bacilli. When using these compounds, small superficial pustules may form on uninjured or healed skin due to yeast. Discontinuation of the compound will clear these pustules. When compared with petrolatum-impregnated gauze alone, the addition of a topical antibiotic ointment may decrease odors. For partial-thickness facial burns, bacitracin can be applied several times a day without a secondary dressing, making it less likely the patient will attract unwanted attention from strangers.
Dressing the wound
There are few comparative studies concerning available wound dressing options; therefore individual preference and comfort will be the determining factors in which option is selected. Wound dressings primarily serve to protect the wound from the outside environment, decrease pain, absorb drainage, and provide a moist environment to promote wound healing. Whatever dressing is used, as long as these qualities are met, the wound should properly heal. As Ambroise Paré said, “ Je le pansai, Dieu le guérit ” (“I treated him, but God healed him”).
Management of first-degree wounds may include the use of emollients or light dressings if needed. Follow-up care should monitor how the wound is healing.
Second-degree wounds can be managed with daily washing of the wound, along with the use of emollients and dressings that are changed daily. Alternatively, they can be covered with a biologic dressing (discussed later), a silver impregnated dressing, alginate dressing, or a 3% bismuth tribromophenate and USP petrolatum gauze (Xeroform gauze). These allow for longer intervals between outpatient visits and are helpful in areas that require long travel times for patients to be seen in the outpatient setting. As with first-degree wounds, follow-up care of second-degree burns should monitor the progression of wound healing. Third-degree wounds, if small, will heal by epithelial ingrowth and contraction. However, most will require referral for surgical intervention.
Patients should be seen at follow-up within several days to examine the progression of wound healing. The follow-up visit also serves to confirm the patient’s compliance with wound care instructions and provides the opportunity to ensure the proper resources are available to the patient to provide an adequate environment for proper healing. Should any concerns arise, changes to the treatment plan including types of dressing or frequency of visits may be needed to optimize care. Otherwise, weekly intervals of follow-up visits provide adequate wound observation.
Synthetic wound dressings
Synthetic wound dressings are popular in the treatment of superficial, partial-thickness burn wounds because they reduce pain, reduce healing time, and cost less than their biologic alternatives. There are many products in this category, with the following discussion representing a small selection of what is available. Choice of dressing is at the discretion of the provider based on personal preference and experience.
Mepitel
Mepitel is a wound contact dressing that adheres to dry skin but not to the wound bed. After application, it can be left in place for up to 2 weeks. Secondary dressings may be placed on top of the Mepitel. These secondary dressings may then be changed when necessary, leaving the Mepitel in place and not disturbing the wound bed. In a comparison with silver sulfadiazine, Mepitel has been shown to decrease healing times and number of dressing changes in pediatric burn patients.
Mepilex AG
Mepilex AG is a synthetic wound dressing commonly used in the treatment of partial-thickness burn wounds. It is composed of three layers, with a silicone layer facing the wound, an absorbent polyurethane foam layer, and a protective waterproof film to keep the wound environment moist while allowing gases to permeate the dressing. The foam layer in this dressing contains silver sulfate, providing antimicrobial action. After cleansing of the wound, the dressing is cut to size and applied to the burn wound, followed by wrapping with gauze and elastic bandages to hold the dressing in place. Follow-up visits for dressing changes can be scheduled for every 3 to 7 days. In a recent randomized study comparing Mepilex AG with silver sulfadiazine, it was shown that a significantly higher number of burn wounds treated with Mepilex AG had healed after 1 week, although overall healing rates were similar. In the same study, patients with Mepilex AG reported less pain associated with dressing changes. Currently the authors are seeing positive results with Mepilex dressing and oral pain medications in the emergency department setting for non-major burns.
Acticoat
Acticoat is a dressing composed of three layers, with an inner layer of rayon/polyester and outer layers of polyethylene coated with elemental silver. This silver is ionized into its bactericidal form when the dressing is moistened. The dressing can be left in place longer, requiring dressing changes every 3 to 7 days depending on which form of Acticoat is chosen. The dressing must be kept moist to be active. Studies suggest that Acticoat may reduce healing time when compared with silver sulfadiazine. ,
Therabond 3D
TheraBond 3D is a woven, silver-impregnated fabric with a perforated wound contact surface. The dressing is designed to allow fluid and exudate from the wound to be transferred through the dressing to an absorbent, secondary dressing. This dressing can be left in place for up to 14 days.
Silverlon
Silverlon is a silver-nylon dressing that has been used extensively in the treatment of burn wounds in the military. Similar to other listed wound dressings, Silverlon may be left in place for 3 to 7 days between dressing changes.
Suprathel
Suprathel is a synthetic burn wound dressing consisting of a thin, porous membrane composed of polylactic acid. The porous nature of the membrane prevents the accumulation of excess wound exudate. When applied to the wound surface, Suprathel becomes translucent, allowing for the wound to be visually inspected for healing and infection without removal of the dressing. The dressing is applied to the burn wound after debridement and is left in place without changing because it will detach on its own as reepithelialization occurs. Petroleum gauze is placed on top of the Suprathel, which is then held in place by gauze and elastic bandages. During follow-up visits, everything except the Suprathel and petroleum gauze may be removed and changed to allow inspection of the wound. In a comparison between Suprathel and Mepilex AG, Suprathel was shown to be a safe alternative dressing with similar healing time; however, it has significant advantages, such as reduced pain and decreased wound bed disturbance because of the ability to leave the dressing in place, as well as improved scar quality. These results are similar to those reported in comparison with other wound dressings. In comparison to porcine xenograft, Suprathel has shown lower necessity for skin grafts, lower infection rate, and without significant difference in healing time.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


