Abstract
A treatment gap exists among patients who are not candidates for or prefer to not undergo traditional facelift and/or necklift. In these cases, radiofrequency skin tightening has been shown to achieve approximately 30% skin contraction through thermal injury to the dermis and tightening of underlaying fibroseptal networks. Subsequent collagen remodeling angiogenesis as well as elastin reorganization functions to visibly improve soft tissue laxity in these cases.
91 Facial Radiofrequency Skin Tightening and Fractional Radiofrequency Technology
Key Points
Radiofrequency (RF) technology has steadily gained popularity since the early 2000s with consecutive increases annually of 10% or more.
Through impedance of electromagnetic current, RF waves lead to differential heating across distinct tissue types consistent with Ohm’s law (energy = currents. Literatur × impedance × time). For example, adipose tissue is less conductive than water (higher impedance), and leads to generation of higher temperatures than muscle. Once soft tissue temperatures reach 50 °C and skin surface reaches 40 to 42 °C there is a trigger to induce neocollagenesis, angiogenesis, and elastogenesis. Through different applications of RF energy (i.e., monopolar, bipolar, multipolar, microneedling), subdermal adipose remodeling (SAR) and long-term soft tissue contraction can be safely and consistently achieved.
91.1 Preoperative Steps
A detailed medical history and physical is obtained on all patients prior to treatment. Exclusion criteria include: pregnancy, open wounds, active infection, dermatologic conditions, bleeding disorders, immunocompromised state.
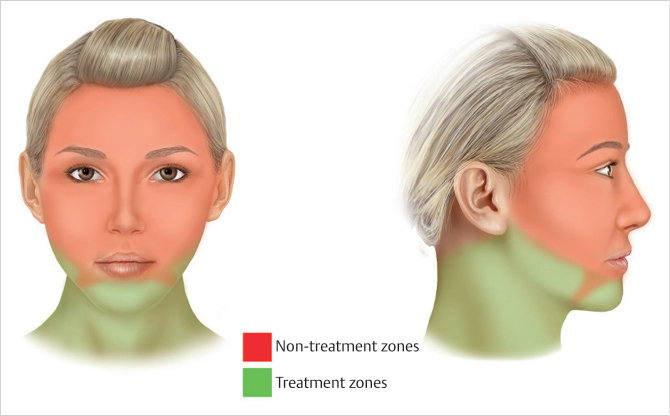
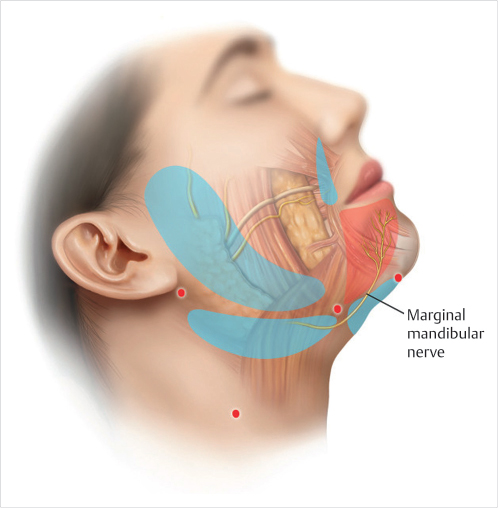
Patients are marked by first identifying the mandibular border and jowls bilaterally. The jowls are subdivided into Zone 1 (above mandibular border) and Zone 2 (below mandibular border). Areas of localized adiposity in the lower face and neck region are marked. Nontreatment zones are identified by carrying a line inferiorly perpendicular to the lip commissures (i.e., marionette lines) (Fig. 91.1). The area medial to these lines are avoided to preserve marginal mandibular innervation to the depressor anguli oris, mentalis, and depressor labii inferioris. Five access points are identified: (1) the submental midline, (2) 1 to 2 cm inferior to the mandibular parasymphyseal/body junction, and (3) post auricular (Fig. 91.2).
Depending on clinical circumstances and patient desires, cases were performed either under general or local anesthesia. In cases of local anesthesia, patients were premedicated with oxycodone (5 mg) and/or benzodiazepine (5 mg).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


