Abstract
Prominent ears and other ear deformities affect over 10% of the general population. For most patients with prominent ears, otoplasty provides consistent results. Excessively large ears or ears with undesirable contours (Stahl’s ears, underdeveloped helical rims, etc.) will require additional maneuvers.
38 Otoplasty
Key Points
Assessment of the ear should be performed in thirds and not all patients will require surgical modification of all “thirds.”
Soft tissue must be removed from deep to the concha to facilitate conchal setback.
Placement of Mustarde sutures is important to help with upper third setback and creation of an antihelical fold.
38.1 Preoperative Steps
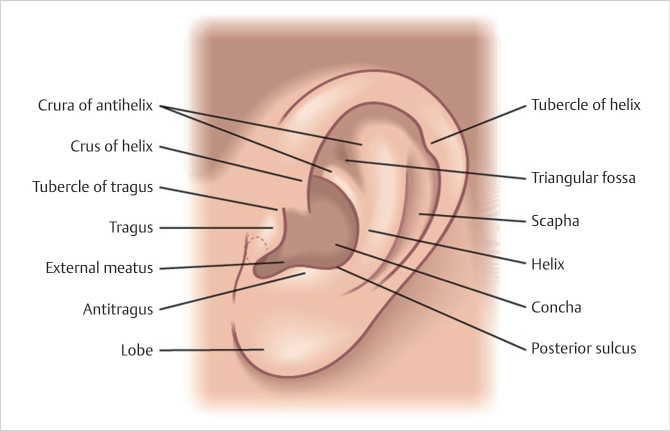
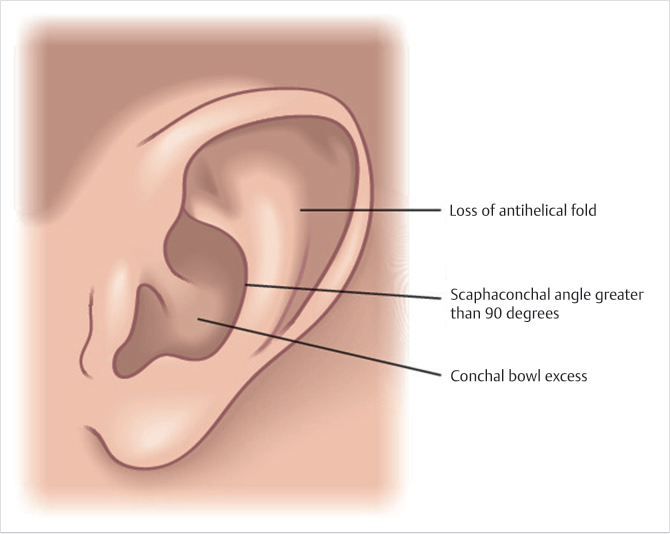
Each third of the ear is assessed for prominence (upper, middle, and lower) (Fig. 38.1 and Fig. 38.2).
Not all patients will require surgical modification of all three “thirds” of the auricle.
The procedure is performed under local anesthesia in adults and adolescents and general anesthesia in children.
38.1.1 Incision and Exposure
An incision is made in the retroauricular sulcus.
The medial surface of the auricular cartilage is exposed.
Soft tissue is removed from deep to the concha to facilitate conchal setback.
A triangle of skin is excised from the medial surface of the lobule in anticipation of lobular setback.
(Reproduced with permission from Mesa J, Buchman S, Mackay D, et al, eds. Atlas of Operative Craniofacial Surgery. 1st ed. Thieme; 2019.)
38.1.2 Combination of Small Conchal Excision and Setback
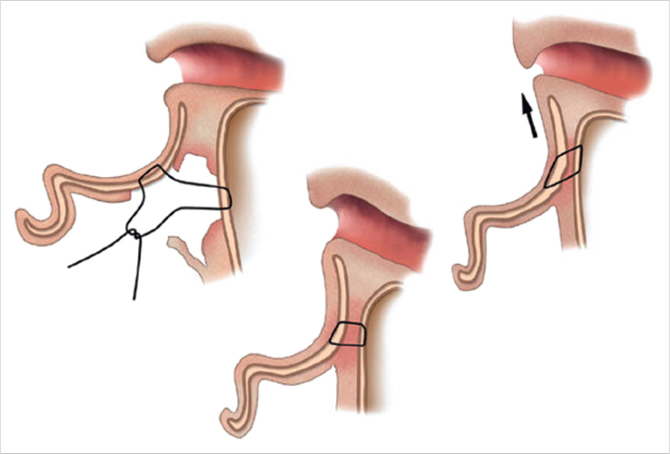
A crescent of cartilage of no more than 3 mm is excised from the concha at the junction of the floor and the posterior wall.
The conchal defect is approximated with PDS sutures.
A conchal mastoid suture of 3–0 PDS is placed (Fig. 38.3).
38.1.3 Lobule Repositioning
Soft tissue is removed from the retrolobular sulcus to expose the caudal aspect of the concha.
Three sutures of 5–0 PDS are used to not only approximate the skin but also include a bite of cartilage on the deep surface of the concha in order to correct lobular prominence.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


