Abstract
Prominent ears and other ear deformities are quite common. Understanding the underlying anatomy and associated anatomical anomalies causing ear deformities will help guide surgical technique. Otoplasty procedures aim to restore an abnormal appearing ear into a natural appearing ear without evidence of surgical intervention.
39 Otoplasty with Anterior Scoring
Key Points
A thorough understanding of the anatomy of the normal and prominent ears is key to correct and precise analysis of ear deformities.
Otoplasty techniques aim to correct ear deformities without evidence of surgical intervention.
39.1 Anatomy
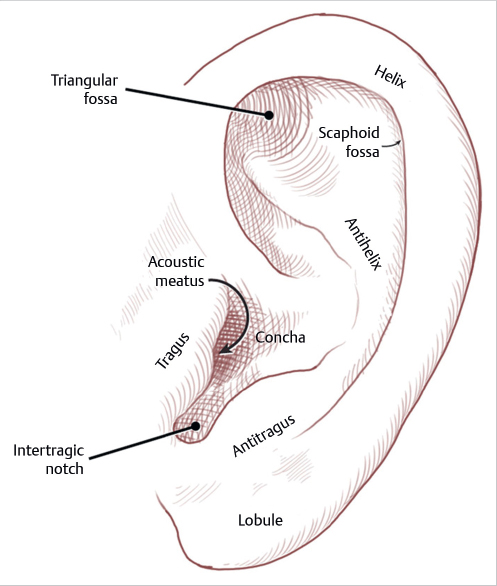
The ear is a composite of cartilage and skin with five key elements—concha, helix, antihelix, tragus, and lobule. Additional structures are antitragus, intertragic notch, and Darwin’s tubercle (Fig. 39.1).
The cartilage of a neonatal ear is softer and more malleable whereas the cartilage become stiffer and more calcified as aging advances.
The ear is 85% of its adult size by the age of 3 years and reaches its mature size in boys in 7 years and in girls in 6 years.
Ear length matures in boys in 13 years and in girls in 12 years.
The vascular supply to the ear is from branches of the external carotid artery, primarily the posterior auricular and the superficial temporal arteries.
Innervation of the ear is supplied by the anterior and posterior branches of the great auricular nerve, the auriculotemporal nerve, and branches of the vagus and glossopharyngeal nerves.
39.2 Anatomy of the Prominent Ear
Conchal hypertrophy or excess.
Inadequate antihelical fold.
Conchoscaphal angle greater than 90 degrees.
Combination of conchal hypertrophy and underdeveloped antihelical fold.
Cranial abnormalities.
Lobular protrusion.
Anterolateral displacement of the tail of the helix.
39.3 Goals of Otoplasty
All upper third ear protrusion must be corrected.
The helix of both ears should be seen beyond the antihelix from the front view.
The helix should have a smooth and regular line throughout.
The postauricular sulcus should not be markedly decreased or distorted.
The helix to mastoid distance should fall in the normal range of 10 to 12 mm in the upper third, 16 to 18 mm in the middle third, and 20 to 22 mm in the lower third.
The position of the lateral ear border of the head should match within 3 mm at any point between the two ears.
Production of a smooth, rounded, and well-defined antihelical fold.
A conchoscaphal angle of 90 degrees.
Conchal reduction or reduction of the conchomastoidal angle.
Lateral projection of the helical rim beyond the lobule.
39.4 Preoperative Steps
Age 6 or 7 years is appropriate for surgical correction given that the ear is nearly fully developed.
Assess the degree of antihelical folding.
Assess the depth of the conchal bowl.
Determine the plane of the lobule and deformity.
Determine the angle between the helical rim and the mastoid plane.
Assess the quality and spring of the auricular cartilage.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


