9 Skin Rejuvenation for Patients with Fitzpatrick Skin Types IV, V, and VI
Key Concepts
Avoid being overly aggressive. Progress in a stepwise fashion to a predetermined goal.
Improvement in the skin tone is most important for these patient populations.
Properly prepare the skin for more intensive treatments (e.g., 20% trichloroacetic acid peel or 30% salicylic acid peel).
Ensure the patient has realistic expectations of the outcome.
Photodocumentation is paramount; often both the provider and the patient forget where they started. Photos are taken even if the patient is only starting on a new skin care regimen.
Introduction
Skin rejuvenation involves improvement of the skin texture and tone that have deteriorated as the skin ages. Skin that has been damaged by sun, environmental exposure, and gravitational forces frequently manifests the following common changes: rhytids, telangiectasias, and dyschromias. The degree to which we see these changes depends on the Fitzpatrick skin type (see Table 6.4 ). For Fitzpatrick skin types I, II, and III, the skin becomes ravaged with rhytids, lentigines, and telangiectasias, the major signs of both photodamage and skin aging. We have an arsenal of techniques to improve these concerns, from aggressive lasers to light chemical peels. Fitzpatrick skin types I, II, and III are fairly resilient to treatments that involve marked edema, erythema, and prolonged recovery. However, for patients of Fitzpatrick skin types IV, V, and VI, the process of aging is a bit different, with fewer concerns regarding rhytids and telangiectasias and more concerns regarding dyschromias and textural changes.
Although the Fitzpatrick classification is very helpful in stratifying patient populations based on their reaction to sun exposure, placing a patient into a discrete category is not straightforward. Traditionally, olive-tone Caucasians of Mediterranean descent were considered Fitzpatrick skin type IV. At the present, due to mixing of ethnic backgrounds, we see patients of African American, Asian, and Latino descent that one can classify as a Fitzpatrick IV: light skin that rarely burns. The ability to tan or burn cannot be determined solely by asking patients about their ethnic background because there are many patients with lighter skin who are of Latino, Asian, or African descent. Regardless of how light their skin is, do not discount their ethnicity by opting for a more aggressive treatment. Their ability to produce melanin in response to injury is significant.
Patients within the Fitzpatrick IV skin type have some concerns with rhytids; the concern lessens as the skin becomes more deeply pigmented and progresses to Fitzpatrick skin type VI. Patients in the Fitzpatrick IV through VI categories are more concerned with gravitational changes, including prominent furrows and folds. Injectables such as neurotoxins and dermal fillers do a superb job in treating these concerns for these patient populations because they typically do not have the superficial rhytids associated with the folds. Because these changes tend to appear ~ 10 years later than they do in their Fitzpatrick I through III counterparts, they are more accepted as the normal process of aging.
Skin rejuvenation for Fitzpatrick skin types IV through VI typically focuses on treating dyschromias. The goal is to treat the skin and improve these conditions without causing harm to the skin in the process. Through the use of a variety of chemical peels, microdermabrasion, and at-home skin care, improvement can be realized with a methodical, graduated approach that is not overly aggressive. As such, this chapter focuses on these techniques, as well as the skin care regimens that work in concert to achieve the desired results.
Background: Basic Science of Procedure
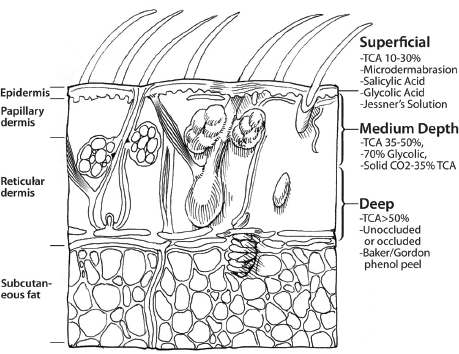
Chemical peels and microdermabrasion are designed to be chemical or mechanical exfoliative treatments that remove skin cells from the surface of the skin. The depth to which the skin cells are removed depends on the type of peel used or the aggressiveness of the microdermabrasion ( Fig. 9.1 ). Superficial peels affect the skin through the level of the epidermis; some peels and microdermabrasion are very superficial, affecting only the stratum corneum. Medium-depth chemical peels penetrate, causing injury in the papillary and upper reticular dermis.1
In the superficial category are the 20 to 40% glycolic acid peels, Jessner′s peels, 10 to 30% trichloroacetic acid peels, salicylic acid peels, and microdermabrasion. The mechanism of action is different for each peel type. The more common α-hydroxy acid peels are glycolic acid and lactic acid peels. These peels produce a keratinocyte dyscohesion that promotes the shedding of the stratum corneum and thickening of the epidermis as a whole.2 Additionally, α-hydroxy acid can promote collagen synthesis in the dermis, causing a thickening of the dermis as well. Glycolic acid peels vary based on concentration, 20 to 70%, and pH, buffered and unbuffered. The lower the pH, the more epidermal and dermal impact.3
Salicylic acid peels, also known as β-hydroxy acid peels or β peels, are safely used in two concentrations, 20% and 30%. This peel functions by breaking the intercellular lipid bonds that encompass the stratum corneum.3 As will be discussed, salicylic acid administered in high concentrations is to be avoided because it can result in salicylism. This also applies to Jessner′s solution, because one of its key ingredients is salicylic acid.
Jessner′s solution has three different components: resorcinol, lactic acid, and salicylic acid ( Table 9.1 ). The modified Jessner′s solution is our preference for all patients because there are occasional patients with resorcinol sensitivity. Additionally, the resorcinol can cause postinflammatory hyperpigmentation in this patient population.4 Alpha hydroxy acids and β-hydroxy acids affect corneocyte adhesion.4 Epidermolysis results when there is a complete detachment of the keratinocytes. From a clinical standpoint, this appears as a graying of the skin that progresses to vesiculation. Several days after the peel, these areas can appear as darkened eschar. Improperly managed, this can result in postinflammatory hyperpigmentation as well.
The mode of action of trichloroacetic acid is precipitation of epidermal proteins and resultant sloughing of the skin.3 As the concentration of the solution increases, the depth of penetration and potential for complications increase dramatically.
Microdermabrasion is a mechanical exfoliation of the skin that typically affects the stratum corneum. There exists the ability to penetrate to the level of the papillary dermis, which is ill advised in this patient population.
Pertinent Anatomy
An understanding of the anatomy of the skin is paramount to using skin treatments in a safe manner. The skin can be thought of as a layered structure. Starting with the outermost layer of the epidermis, the stratum corneum is the horny outside layer. This is the skin that sheds with very superficial skin treatments.
The epidermis is composed of four other layers, with the lowest layer being the basal layer. The melanocytes are present within the basal layer. Keratinocytes found in the basal layer connect the dermis and the epidermis. Within the dermis are blood vessels and collagen. Therefore, when performing microdermabrasion or any other resurfacing procedure, the onset of pinpoint bleeding signifies penetration into the dermal layer of the skin.
The melanocytes produce melanin. Although we all have the same number of melanocytes, the amount of melanin in the skin determines the phenotypic appearance of the skin. Patients with more melanosomes, housed in keratinocytes, produce melanin that appears darker. Furthermore, the melanocytes in those of the higher Fitzpatrick skin types are more labile and produce exaggerated amounts of melanin in response to a stimulus.3 This accounts for the increased incidence of melasma and postinflammatory hyperpigmentation in these patients.
Encouraging the skin to turn over skin cells will help to reduce the amount of excess melanin in the skin. Mechanical or chemical exfoliation hastens the normal process of cellular turnover, helping patients realize their goals sooner. The addition of a home skin care regimen that targets the reduction of melanin production with the use of products that enhance exfoliation further accelerates the process.
Patient Selection
Almost any patient is a candidate for a chemical peel or microdermabrasion. The strength of the peel or aggressiveness of the microdermabrasion treatment is the decision that needs to be made. Additionally, certain categories of peels are more appropriate for particular skin conditions.
Glycolic acid peels are commonly used peels that will enhance exfoliation without significant peeling. This α-hydroxy acid in a strength of 30% is appropriate for almost all skin types but still must be monitored closely for early neutralization in patients who are more sensitive to peels. These peels will also improve hyperpigmentation and fine lines. Buffered glycolic acid peels produce less inflammation, less tingling, and less peeling. Unbuffered solutions with a low pH tend to produce more exfoliation. Salicylic acid peels are the go-to peel for patients who are bothered by acne vulgaris. They also improve areas of hyperpigmentation, so are ideal for patients of color with postinflammatory hyperpigmentation due to acne. Modified Jessner′s peels are preferred over the traditional Jessner′s peel due to the replacement of the resorcinol with citric acid or other more universally tolerated compound. The modified Jessner′s peel is helpful for patients with acne, dyschromias, enlarged pores, and textural concerns. microdermabrasion is appropriate for the patient who has acne, textural concerns, and acne scars. Almost any patient can undergo microdermabrasion, though it is not recommended for patients with significant telangiectasias or pustular acne.
Patient selection also involves asking about medical history. Isotretinoin usage in the past year, salicylic acid or aspirin allergy, or known resorcinol sensitivity should be elucidated in addition to the usual questioning to obtain the history. Prior to the first chemical peel or microdermabrasion, patients are given a consent form to read and a printed periprocedural care form to take home and read. The periprocedural form is reviewed with patients before the procedure to ensure that they understand the required postprocedural care. The form also confirms that they have not been on isotretinoin in the past year.
Technical Aspects of the Procedures
The technical aspects of glycolic acid peels, Jessner′s and modified Jessner′s peels, salicylic acid peels, and microdermabrasion are variable based on the treatment. The overarching theme in treating patients of color is conservatism. Avoid being overly aggressive. It is better to do a series of lighter, safer treatments than it is to do one aggressive treatment. A home skin care regimen often enhances the cosmetic result.
Skin preparation is necessary prior to all skin treatments and begins with a thorough cleansing of the skin. In most instances, we use a glycolic acid cleanser with water to cleanse the entire face. In Fitzpatrick IV patients, we use a mechanical cleansing brush to enhance the peel application. In Fitzpatrick V and VI patients, this may deepen the peel to an undesired level. Next, the skin is wiped clean with water-soaked gauze and then patted dry with more gauze. Subsequently, the skin is degreased with alcohol on gauze or a cotton ball and allowed to dry. At this point, the skin is ready to proceed to the chemical peel or microdermabrasion of choice.
Glycolic Acid Peel
Glycolic acid chemical peels are the workhorse peel for many patients. They are in the family of α-hydroxy acid peels, which also include lactic acid. For Fitzpatrick V and VI patients, 30% and 40% glycolic acid peel concentrations are effective without increased risk of complications. For Fitzpatrick IV patients, a 50% glycolic acid peel concentration is the maximum strength; peels are always used in a stepwise manner. However, for some Fitzpatrick IV patients who experience a significant amount of tingling or even a gray patch, epidermolysis, with the administration of the 40% peel, a 50% peel is not recommended.
In preparation for the peel, the neutralizer and timer should be made readily available. The timer should be set for 5 minutes just prior to application of the peel. This is the maximum time that the peel will stay on the skin. Apply the peel solution in a nonoverlapping manner with uniform pressure to the skin. The solution can be obtained from a bottle or premade peel pads. The gauze or pad should not be dripping wet so as to avoid pooling in areas of dependency or running away from the intended area of application. This should be done as efficiently as possible so that the entire face has a relatively similar exposure period. The skin is monitored for markedly increased erythema and gray areas that signify epidermolysis.
Peel neutralization occurs based on symptoms of marked tingling/burning, areas of excessive erythema, or when the timer has reached 5 minutes. The peel is neutralized with a base solution, typically of sodium bicarbonate, prepared in advance so that it is ready and available prior to the application of the peel. The base solution is applied to the area to which the peel was first applied or the area that is burning the most. The solution typically foams when sprayed or applied with solution-soaked gauze to the skin; it will feel slightly warm to the patient due to the exothermic reaction. The foaming and warmth subside when the peel has been neutralized. After complete neutralization, water-moistened gauzes can be placed on the skin for a soothing effect. The skin is observed for any issues or concerns. Antioxidant and sun protection factor creams are applied prior to departure. Questions regarding any of the written postpeel instructions are answered at this point.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


