5 Superficial Chemical Peels
Key Concepts
Enhanced superficial chemical peels are an important minimally invasive cosmetic technique that can benefit a wide range of patients and can be easily incorporated into an aesthetic practice.
The success of the enhanced superficial chemical peel can be improved with adequate patient preparation.
Performance of a series of six to eight adequately frosted trichloracetic acid (TCA) peels (15 to 25%) accomplishes a more advanced form of superficial peeling—which may be considered equivalent to medium-depth peels.
Enhanced superficial chemical peels can, in some patients, approximate the results of fractionated laser treatments.
Introduction
For centuries, man has searched for a “miracle potion” that would reverse aging, wrinkled skin. Ancient topical treatments with milk, wine, and various fruits were used in an attempt to improve the skin. By the early 20th century, “lay peelers” began using a variety of techniques and topical agents that afforded deeper skin penetration. These peels, adopted by some members of the medical community, were often a source of controversy; however, eventually they became an accepted practice. Deep chemical peels became a key procedure in the treatment of the aging face and represented an important component of a successful facial aesthetic practice after Baker and Gordon popularized the classic phenol peel in the 1960s. Since then, there has been continuing interest in resurfacing the facial skin and an evolution of peeling agents, including those for superficial peeling.
In the 1990s, lasers became popular tools to resurface the skin. Whereas some lasers treat more superficially, others, such as the carbon dioxide laser, have the potential to treat deeply. The side effects of deep carbon dioxide lasers (e.g., long-term hypopigmentation) fostered the development of fractionated beams designed to lessen tissue damage and reduce side effects. However, the separation of beams to spare segments of untreated tissue and the reduction of intensity of the fractionated light beam reduced aesthetic results.
Properly structured skin care/peeling protocols utilizing the sequential application of a novel superficial chemical peeling technique may approximate many of the fractionated laser treatments. Peels can be offered as an effective alternative to laser treatments because they are inexpensive. This chapter describes a unique technique that can provide greater improvements than those typically obtained by superficial peels. The technique of “enhanced superficial chemical peeling” has been found to produce excellent results with minimal down time and costs.
Background: Basic Science of Procedure
Chemical peeling involves the application of a chemical exfoliant that initiates a controlled wound to the epidermis and/or dermis. In general, results are dependent upon the depth of penetration. Penetration can be altered by the type of agent, the concentration of the agent, the time of contact with the skin, the potential reapplication of the agent, and the resistance of the skin. Peeling may be enhanced by pretreating the skin with an effective daily exfoliation program designed to disrupt a damaged keratin surface, allowing improved penetration of the peel. Pretreating may also stimulate regeneration from the basal layer. Effective peeling may improve surface irregularities and stimulate fibroblast activity and collagen production.
Superficial peeling agents include α-hydroxyl acids (glycolic, lactic, and pyruvic acids), salicylic acid, retinoic acid, resorcinol, and TCA (in lower concentrations). Solutions like Jessner′s solution (resorcinol, 14 g; salicylic acid, 14 g; lactic acid, 14 mL; ethanol, 100 mL) have also been formulated to peel at a superficial level.
Most superficial peels are used to improve very fine wrinkles and pigmentary changes. However, some peels are used for other indications. The lipophilic nature and anti-inflammatory properties of salicylic acid make it a popular peel for acne-prone patients.
The concentration of the peel determines whether it is considered superficial or medium. For example, TCA used in higher concentrations may be considered a medium-depth peel. The authors consider TCA peeling above 35% to be unpredictable, and it is known to be associated with scarring when used above 45%.1,2 The length of application time can also determine if a treatment is superficial or medium. Repeated single-treatment placement of high concentrations of pyruvic or glycolic acids, for example, may cause a medium-depth treatment.3
Pertinent Anatomy
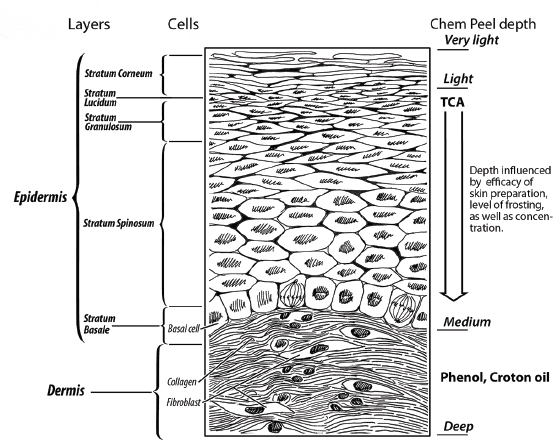
The epidermis is composed of several layers of cells that are all generated from the innermost stratum basale. The basal cells continually regenerate the layers of skin cells. The cells migrate up from the stratum basale to the stratum spinosum, stratum granulosum, stratum lucidum (usually found only on the friction-prone areas, such as the palms and soles), and to the outermost stratum corneum ( Fig. 5.1 ). Melanocytes can be found in the basal layer.
Beneath the dermal-epidermal junction lies the papillary dermis. Deep to this layer is the reticular dermis, which interdigitates with the papillary dermis above. The papillary dermis is thin, with loose collagen bundles and abundant fibrocytes. The reticular dermis, in contrast, is thicker, with dense collagen and fewer fibrocytes.
As we age, the skin regeneration process slows, the epidermis thins, and the outer stratum corneum layer becomes less organized. The rete pegs and dermal papillae become less pronounced, which results in a flattening of the dermal-epidermal junction. The dermis also thins and the collagen and elastin fibers diminish in volume and organization. The additive effects of this aging process and associated solar damage lead to characteristic findings, including irregular, wrinkled skin with keratosis and pigment changes.
Patient Selection
Perhaps the most important aspect of appropriate patient selection is in a realistic understanding of the limitations of various types of chemical peels. Many of the so-called superficial peels may disrupt the stratum corneum but have limited impact on more advanced skin-aging changes. Some of the more aggressive superficial peels (e.g., the higher concentrations of glycolic acid) may be an appropriate option for improving overall skin quality, such as rough texture and some solar damage. Photoaging to a Glogau I or II level may respond well to some types of superficial chemical peeling.
Acne may sometimes be improved with superficial chemical peels. Superficial pigmentary dyschromias, such as solar lentigines and melasma, can also be treated. However, deeper vascular abnormalities may not be addressed.
Although it has been taught that multiple superficial peels are not equivalent to medium or deep peels, in the experience of the authors a sequential application of enhanced superficial chemical peels can be effective in reducing fine rhytids. Enhanced improvement is attainable using a lower level of TCA, with adequate skin pretreatment and a series of more aggressive peels that are applied to the proper frosting level. The immediate reapplication of the peel, in the opinion of the authors, can increase the depth of treatment and improve a significant portion of superficial rhytids when used with this protocol.
A careful patient history should focus on any skin disorders, such as various forms of dermatitis, rosacea, acne, or herpes simplex virus infection. History of radiation exposure, immunosuppression, autoimmune disease, and collagen vascular disease is also important to elicit. These factors can impact wound healing. Additionally, there is the potential for chemical peeling to exacerbate an underlying skin disorder.
The physician, as with all cosmetic procedures, should understand the patient′s desire and communicate realistic expectations of the refined superficial chemical peel. The patient should also understand the importance of the role that he or she will play in the pre- and posttreatment skin-care regimen. Standardized photographic documentation, as always, may help record most conditions. However, some details may not be captured by photography, especially with slight changes due to the limits of lighting, exposure, and camera capabilities.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


