83 Arthroscopic TFCC/Ligament Debridement
Abstract
Tears of the scapholunate and lunotriquetral ligaments and the triangular fibrocartilage complex (TFCC) can be treatable pain generators in patients presenting with wrist pain. Simple arthroscopic debridement of these lesions has been suggested to yield successful outcomes with minimal surgical risk in patients without instability. Assessment with advanced imaging such as MRI or diagnostic arthroscopy can provide valuable information regarding articular pathology.
83.1 Description
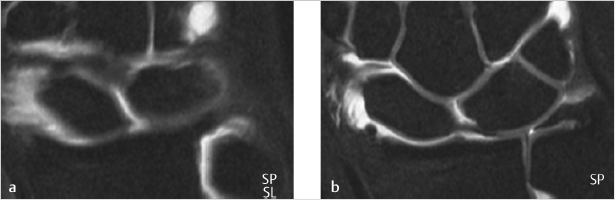
The painful wrist without carpal instability or arthritis can be a diagnostic and treatment challenge. Partial tears of the scapholunate and lunotriquetral interosseous (intercarpal, IC) ligaments and triangular fibrocartilage complex (TFCC) tears can be treatable pain generators (► Fig. 83.1). Simple arthroscopic debridement of these lesions has been suggested to yield successful outcomes with minimal surgical risk.
83.2 Key Principles
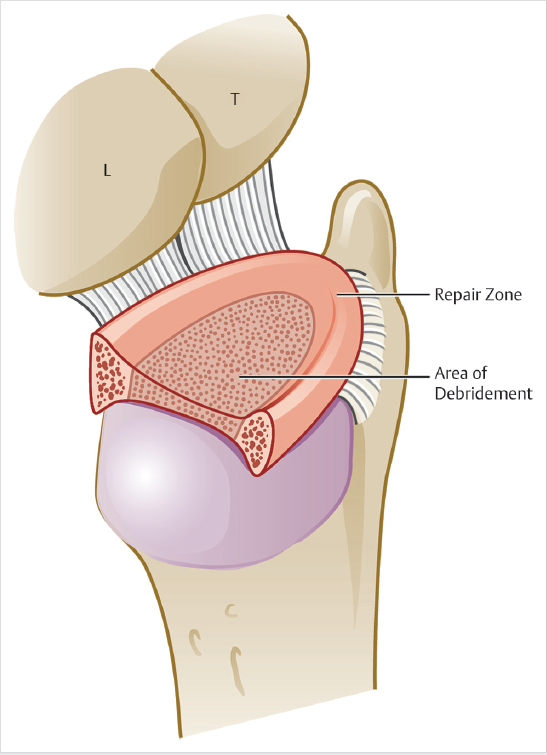
A thorough understanding of wrist anatomy is essential to enable arthroscopic evaluation of the joint for proper diagnosis and treatment decision making. Careful preoperative decision making and patient selection is critical to a successful result. For the TFCC tears that occur in the vascularized periphery are amenable to repair, whereas those in the avascular center should be debrided (► Fig. 83.2).
83.3 Expectations
The painful wrist without carpal or distal radial ulnar joint (DRUJ) instability may benefit from debridement of structures found to be degenerative on magnetic resonance imaging (MRI) or arthroscopic visualization. The surgeon must recognize when instability is present and potentially the source of pain, as debridement may not be the procedure of choice.
83.4 Indications
Commonly suggested wrist pain generators are the scapholunate (SL) and luntotriquetral (LT) ligaments as well as the TFCC. These structures can become partially disrupted after a fall or become degenerative over time. When the structures are functioning appropriately (no intercarpal or DRUJ instability present), arthroscopic debridement alone may be appropriate, although high-quality literature supporting these procedures is sparse.
83.5 Contraindications
When evidence of instability exists, debridement alone is unlikely to be beneficial. Carpal instability is demonstrated by static changes on imaging, positive provocative maneuvers on exam, or high-grade IC ligament tears seen arthroscopically. DRUJ instability is best demonstrated on physical exam. Additionally, if arthritic changes are present, simple debridement of the TFCC or IC ligaments is unproven to be beneficial.
83.6 Special Considerations
Preoperative decision making is of utmost importance. The surgeon must be aware that IC ligament and TFCC tears seen on MRI are extremely common and increase with age, and therefore should be presumed to be incidental findings. 1 , 2 The patient with a stable, but painful wrist should be managed conservatively to the maximal extent to include bracing, therapy, anti-inflammatory medications, steroid injections, and most importantly activity modification. Most patients seeking care will report dorsal wrist pain when loading the joint in extension. If that particular activity can be avoided, this may solve the problem altogether. Patients should be informed that pain relief after debridement of these structures can be unpredictable.
83.7 Special Instructions, Positioning, and Anesthesia
General anesthesia or a regional block is typically used. Supine position is preferred. A traction tower is applied with 10 to 15 lb of distraction force needed to achieve visualization of the joint (► Fig. 83.3). There are multiple commercial traction devices which can be utilized. Simple longitudinal traction is sufficient for this procedure, although some devices allow for easy rotating and repositioning of the limb which is helpful in cases requiring fluoroscopy. A small joint arthroscope (1.9 or 2.7mm) is used, along with a small probe, 3.5mm mechanical shaver, and a cautery/radiofrequency probe.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


