82 Diagnostic Wrist Arthroscopy
Abstract
Wrist arthroscopy is the reference standard in diagnosing and evaluating suspected intra-articular wrist disorders after a comprehensive history and physical examination. Its role continues to expand as an adjunct procedure to treat several disorders.
82.1 Key Principles
A comprehensive evaluation and documentation of the radiocarpal and midcarpal joints is essential. Arthroscopy should proceed in a systematic and uniform approach to avoid missing pathology and to review captured images in a predictable sequence. Preoperative evaluation, including the specific location of pain and mechanism of injury, if any, will help differentiate symptomatic pathology from asymptomatic, degenerative conditions. Particular attention should be made in preserving articular cartilage by avoiding abrasion and thermal injury.
82.2 Expectations
Patients should be informed of the unique risks of this procedure including structural injury, failure to identify pathology, and any possible interventions including the need for immobilization. In cases of an uncertain diagnosis, the patient and the surgeon should be prepared for open surgery. An option for a staged procedure should be offered to and discussed with the patient preoperatively in the event that the findings indicate a subsequent procedure should be performed.
82.3 Indications
Wrist arthroscopy may be performed to diagnose and evaluate suspected intra-articular wrist disorders after a comprehensive history and physical exam. In general, the following procedures may be performed arthroscopically:
Synovectomy
Loose body excision
Ganglion cyst resection
Triangular fibrocartilage complex (TFCC) tear debridement or repair
Scapholunate interosseous ligament (SLIL) assessment and debridement
Lunotriquetral interosseous ligament (LTIL) assessment and debridement
Evaluation and treatment of midcarpal joint disorders
Capsular shrinkage/contracture release
Arthroscopic resection of distal ulna, radial styloid, and carpal bones
Arthroscopic-assisted reduction and fixation of fractures
82.4 Contraindications
Radiographic evidence of significant radiocarpal arthritis
82.5 Special Considerations
Most arthroscopic procedures are performed through dorsal portals in relation to the extensor compartments. Because of their remoteness from the radial artery and radial nerve branches, the 3–4 and 4–5 portals are considered the safest. 1 , 2 The superficial branch of the radial nerve and radial artery are found to be on average 16 mm and 26 mm, respectively, from the 3–4 portal. As such, these portals are established first. The greatest risk of neurovascular injury is in creation of the 1–2 portal. Here, the superficial radial nerve and radial artery both pass within 3 mm of the portal. The dorsal sensory branch of the ulnar nerve is found 4.5 mm from the 6 U portal and 8.3 mm from the 6 R portal. 1 Volar portals are less commonly used because of greater dissection and neurovascular risks but they provide visualization of the dorsal capsule and volar interosseous ligaments as needed. Finally, avoid thermal injury by using short pulses of the radiofrequency cautery rather than prolonged use. A small joint arthroscope (1.9 or 2.7 mm) is typically used.
82.6 Special Instructions, Positioning, and Anesthesia
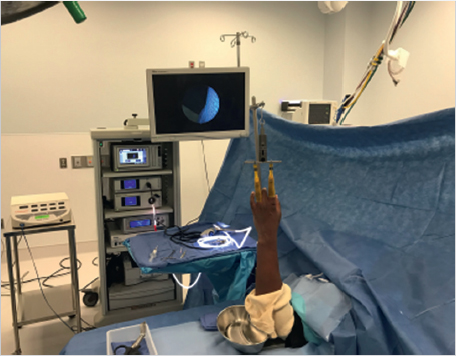
Supine, with the involved arm on a hand table (► Fig. 82.1)
Tourniquet on the upper arm although inflation is often not required
Fingers in traction tower with the elbow and forearm padded
General anesthesia or regional block with sedation
82.6.1 Tips, Pearls, and Lessons Learned Positioning and Wrist Distraction
Avoid exsanguination of the limb to better visualize dorsal veins during portal placement. Finger traps should be applied with consideration to the effects of radial and ulnar deviation. In general, application of large-sized finger traps to the index and ring fingers provides uniform distraction across the radiocarpal joint. Ten to fifteen lb of traction is required to introduce the camera and instruments. If the traction tower is unstable on the hand table, place sterile towels or a metal tray cover under the tower base to stabilize it. Slight wrist flexion distracts the dorsal wrist permitting easier instrumentation.
82.6.2 Portal Placement
The standard portals are detailed in ► Table 82.1 and ► Fig. 82.2. The radiocarpal joint is insufflated with normal saline using a 22G needle through the 3–4 portal, bearing in mind the normal radial volar tilt of 11°. Shallow vertical incisions through the skin and blunt capsulotomy with a mosquito clamp decrease the risk of tendon injury. The EPL tendon is particularly at risk at the 3–4 portal. A blunt trocar is inserted, the obturator is removed, and a 2.7-mm 30°-angled arthroscope is inserted. An outflow portal is created using an 18G needle placed into the 6U portal under arthroscopic visualization. To avoid high-pressure ejection of fluid from the portal, attach an IV extension tube to the outflow needle to guide fluid directly into a kidney basin. The 4–5 portal may be created at this time under arthroscopic visualization to introduce aprobe.

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


