81 Thumb CMC and MCP Joint Arthroscopy
Abstract
Indications for thumb carpometacarpal (CMC) and metacarpophalangeal (MCP) joint arthroscopic-assisted procedures are evolving, and the application of these minimally invasive and tissue-sparing techniques continues to expand. The most common indications of these techniques include diagnostic evaluation of small joint disorders, synovectomy and joint capsular shrinkage, joint surface resection, and the arthroscopic management of reducible intra-articular fractures. Contraindications for these techniques include active soft tissue disruption or infection, comminuted fractures of the metacarpal base, or intra-articular fractures not amenable to closed reduction. While these evolving techniques represent technically achievable tools in the surgeon’s armamentarium, the use of such techniques should be weighed against the respective risks and benefits of their open procedure alternatives.
81.1 Indications
The most commonly described applications include the diagnostic evaluation of small joint arthrosis and ligamentous injuries, synovectomy, joint capsular shrinkage, joint surface resection, intra-articular fracture reduction assistance, the reapproximation of collateral ligament avulsion injuries, septic arthritis, and the retrieval of small foreign bodies. 1 , 2 , 3 , 5 , 6 , 7 , 8
81.2 Contraindications
Contraindications for these techniques include active infection, disrupted surrounding soft tissue, comminuted fractures (e.g., Rolando-type fractures), or intra-articular fractures not amenable to closed reduction. 1 , 2 , 3 , 4
81.3 Procedural Setup
In the supine position, with the patient under general or regional anesthesia, the operative arm is fully prepped and draped in standard fashion. A sterile tourniquet is applied over the extremity and can be insufflated to improve arthroscopic visualization as necessary. The arm is positioned and secured to the wrist arthroscopy traction tower and all bony prominences are protected and padded with sterile towels (► Fig. 81.1). A finger trap is placed over the thumb and approximately 8 pounds of traction is spanned across the wrist and adjusted intraoperatively to optimize arthroscopic visualization of the joint. A 1/4-inch Coban strip wrapped around the finger trap mechanism can be helpful to improve finger trap security.

81.3.1 Establishing Portals
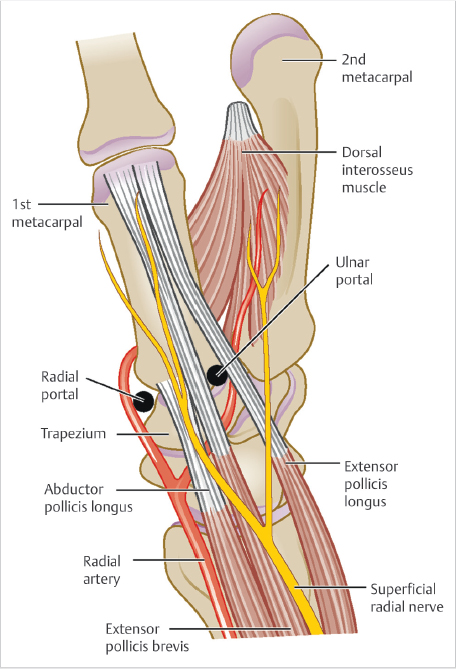
The 1-R Portal is located at the level of the thumb carpometacarpal (CMC) joint line and radial to the abductor pollicis longus (APL) tendon. The 1-U Portal is located at the same level and ulnar to the extensor pollicis brevis (EPB) tendon (► Fig. 81.2). Outlining the course of first dorsal compartment tendons traversing the CMC joint is helpful prior to establishing portals. A 22-gauge hypodermic needle is placed through the 1-R Portal, with a radial to ulnar trajectory and an approximately 25-degree distal angulation to accommodate the sad-dle-shaped surface of the CMC joint. 1 , 4 Similarly, the 1-U Portal may be established in an analogous manner based on surgeon preference. If difficulty is encountered during this step, mini-C-arm fluoroscopy may be utilized to verify the proper working level and needle position. The joint can be insufflated with approximately 1.0mL of saline prior to establishing both portals. Using a #11 blade, small 3-mm skin incisions are made. We prefer longitudinal incisions parallel to the course of the extensor tendons, thus minimizing the possibility of iatrogenic injury. A small mosquito hemostat is useful to bluntly spread and dissect down to the capsular layer, prior to entering the joint with the scope sheath and blunt trocar. A 1.9-mm 30-degree scope and 3-mm hook portal are inserted into the chosen portals, saline inflow is opened via gravity or a small joint pump, and diagnostic arthroscopy may now ensue, with the pneumatic tourniquet insufflated to 250mm Hg as needed. A 2.7-mm 30-degree scope can also be utilized to increase the visual field after working portals are established.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


