80 Subtotal Fasciectomy for Dupuytren’s Disease
Abstract
Subtotal fasciectomy is one of the most common surgical techniques for the treatment of Dupuytren’s disease. As this benign fibroproliferative disease progresses, hand function deteriorates secondary to digit contracture. Once surgery is indicated, subtotal fasciectomy involves excision of the involved pathologic tissue with preservation of the palmar skin whenever possible. Successful outcomes can be obtained with restoration of digit extension and protection of the neurovascular structures.
80.1 Key Principles
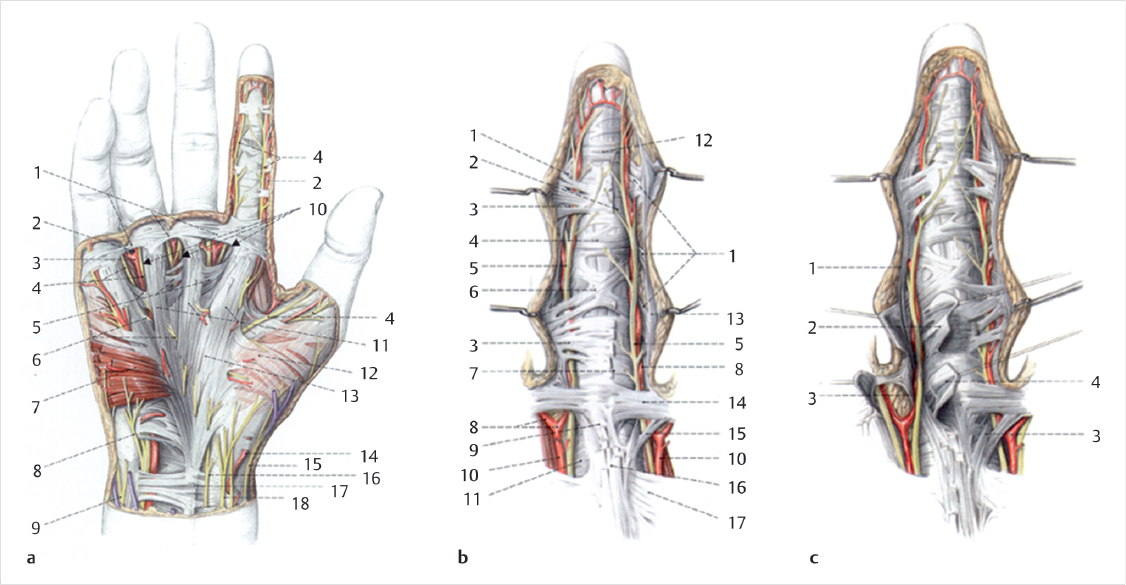
Dupuytren’s disease is a proliferative condition of the palmar fascia on the palm of the hand (► Fig. 80.1). It initially manifests itself as palmar nodules, which can then progress to cord formation and eventual digital contracture. Performing subtotal fasciectomy is based on four principles: (1) design and preservation of skin flaps; (2) identification and preservation of neurovascular units to each digit; (3) removal of diseased tissue when implicated in contracture; and (4) contracture release.
80.2 Indications
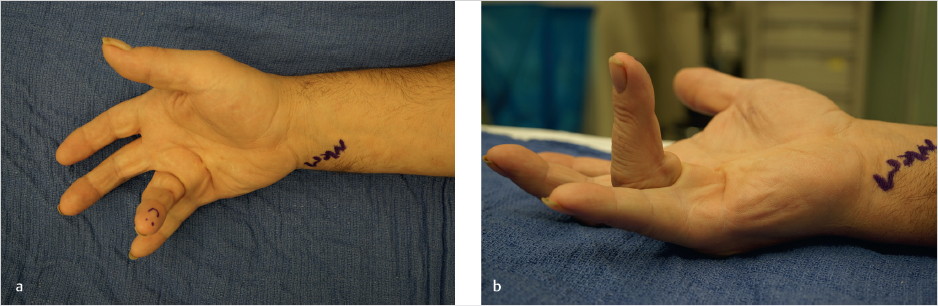
Once contracture of the metacarpal phalangeal joint (MCPJ) and/or proximal interphalangeal joint (PIPJ) becomes severe enough to interfere with the patient’s daily function, surgery becomes a viable option. As the disease progresses, opening the hand becomes difficult and grasping objects becomes awkward. The social stigma may also become aggravating to the patient. The “table top test” may be a good test for the patient to monitor his or her own disease progression. The test is positive when the patient can no longer place their palm flat on a flat surface. Flexion contracture of the MCPJ>30 degrees and PIPJ > 5 to 10 degrees has been used previously as indicators for surgical intervention. 1 However, the degree of contracture and how it interferes with function differs from patient to patient (► Fig. 80.2a,b).
80.3 Contraindications
Surgery is contraindicated in patients who are debilitated or where the general medical condition prohibits elective surgery. Furthermore, surgery is not a good option in patients with poorly controlled mental illness, or any patient that is unwilling or unable to participate in the postoperative rehabilitation protocol. Active infection in the ipsilateral extremity is also a contraindication to this elective procedure.
80.3.1 Relative Contraindication
A known injury to the affected digit with only one residual digital nerve or artery is a relative contraindication to this procedure. Injury to the remaining artery or nerve may render the digit dysvascular or insensate with a poor outcome. Additionally, a relative contraindication exists in patients with Dupuytren’s diathesis’s or with recurrent disease and severe contracture. These patients may require more extensive fasciectomy and full-thickness skin grafting. 2 , 3
80.4 Procedure
In contrast to dermofasciectomy, skin incision and flap design is paramount. Preservation of skin coverage after excision of the Dupuytren’s fascia allows for more rapid wound healing, less postoperative wound management by the patient and surgeon, and an accelerated rehabilitation. Psychologically, the patient does not need to prepare for an open wound and is better able to participate in the postoperative course.
Preservation of the palmar skin overlying the diseased tissue can be challenging as cords and nodules lie in close proximity to the dermis. As a result, separation of these layers can be difficult. Identifying the plane of dissection proximal and distal to the dis-eased tissue will aid in identifying the correct tissue plane so as not to compromise the skin flap or leave excess diseased tissue in the hand/palm. The procedure is best performed under loupe magnification.
80.4.1 Skin Incision
The design of skin flaps is surgeon dependent, but often is a variation of the classic volar Brunner incision (► Fig. 80.3a). Other options include longitudinal midline incisions with subsequent z-plasty flaps, curvilinear incisions, V-Yadvancements, or combinations ofall the above. 4 The riskofperforating the skin may occur during dissection, but so long as not excessive is usually of little consequence. These areas, when small, allow for hematoma drainage and heal without additional intervention.
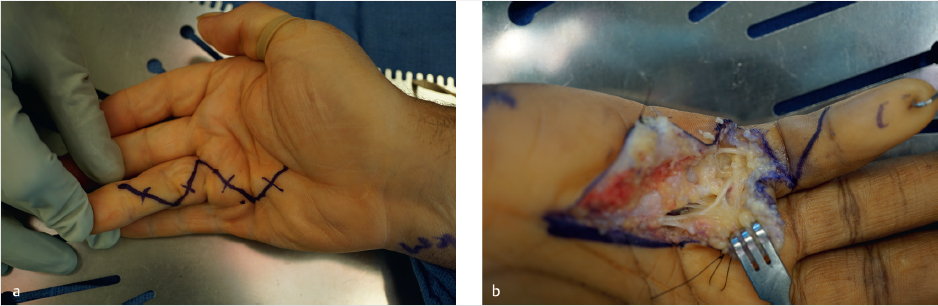
Special Consideration
Care must be taken during skin flap design in anticipation of the neurovascular bundles. Extensive identification and protection is paramount. High-risk areas are at the radial and ulnar skin creases of each digit and surrounding the cords and nodules (► Fig. 80.3b).
Related posts:
 79 Needle Aponeurotomy for Dupuytren’s Disease
79 Needle Aponeurotomy for Dupuytren’s Disease
 10 Extensor Indicis Proprius Tendon Transfer for Rupture of the Extensor Pollicis Longus Tendon
10 Extensor Indicis Proprius Tendon Transfer for Rupture of the Extensor Pollicis Longus Tendon
 15 Extensor Carpi Ulnaris Tenosynovectomy/Instability
15 Extensor Carpi Ulnaris Tenosynovectomy/Instability
 28 Open Ulnar Nerve Decompression/Subcutaneous Transposition at the Elbow
28 Open Ulnar Nerve Decompression/Subcutaneous Transposition at the Elbow
 48 Corrective Osteotomy of Metacarpal Malunion
48 Corrective Osteotomy of Metacarpal Malunion
 59 Scaphoidectomy and Four-Corner Fusion
59 Scaphoidectomy and Four-Corner Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


