28 Open Ulnar Nerve Decompression/Subcutaneous Transposition at the Elbow
Abstract
Ulnar nerve compression at the elbow is the second most common, compressive, peripheral neuropathy of the upper extremity. When symptoms are recalcitrant to nonoperative treatment, surgical interventions include in situ decompression, decompression with anterior nerve transposition, and medial epicondylectomy. Despite meta-analyses and randomized control trials that have attempted to elucidate the differences between various surgical approaches, the optimal surgical technique remains controversial. We describe our surgical technique for open ulnar nerve decompression at the elbow.
28.1 Description
Many different approaches and surgical techniques have been described to treat ulnar nerve compression at the elbow. Open in situ ulnar nerve decompression was first described in the 1920s. 1 It involves step-wise decompression of the ulnar nerve at multiple anatomic sites of potential compression including the arcade of Struthers, medial intermuscular septum, cubital tunnel retinaculum, Osborne ligament, and along the superficial and deep investing fascia of the flexor carpi ulnaris. In select cases, recession of a hypertrophic or snapping medial triceps or division of an anconeus epitrochlearis may be required. Anterior transposition (both subcutaneous and submuscular) aims to prevent dynamic intraneural compression from repetitive elbow flexion. Proponents of transposition highlight that dynamic traction plays a significant role in symptom etiology in addition to static compression. Pearls and pitfalls of decompression and transposition are highlighted below.
28.2 Outcome
A recent meta-analysis 2 comparing open in situ decompression to subcutaneous or submuscular anterior transposition demonstrated no statistically significant differences in surgical outcomes between techniques; however, there was a strong trend across all included studies toward better results with either subcutaneous or submuscular transposition, with p-values approaching statistical significance. Anterior transposition may result in a higher rate of complications such as sensory loss around scar and superficial infection due to more extensive exposure frequently required for the procedure. 3 Staples et al 4 recently demonstrated that ulnar nerve transposition increases surgical morbidity due to persistent peri-olecranon paresthesia, greater narcotic consumption, and more patient-reported disability up to 8 weeks after surgery. However, in this series, most differences in surgical morbidity were transient and resolved after 8 weeks following surgery.
28.3 Indications
Progressive neurological symptoms (sensory or motor)
Persistent medial elbow pain
Symptomatic ulnar nerve subluxation and snapping
Failed conservative management
Preoperative electrodiagnostic studies are helpful in confirming the diagnosis, and grading the severity of the electrophysiological disturbance. In the setting of negative electrodiagnostic studies yet consistent history and exam findings, ulnar nerve decompression is acceptable.
28.4 Positioning and Anesthesia
Patients are positioned supine with the arm supported on a hand table. The procedure is typically performed under regional anesthesia. We supplement the regional anesthetic with local anesthesia approximately 8 cm proximal to medial epicondyle to ensure adequate anesthesia within the medial brachial and antebrachial cutaneous nerve territories. Preoperative IV antibiotics are administered according to surgeon preference. A sterile tourniquet is applied to ensure adequate proximal access. An Esmarch bandage is used for exsanguination. A sterile bump may be placed under the elbow and upper arm to allow better visualization of the medial elbow.
28.5 Operative Techniques
28.5.1 Open In Situ Ulnar Nerve Decompression
The length of the incision varies based on surgeon preference, though more than 4 to 5 cm are rarely required, based on body habitus and soft tissue compliance. The incision is centered at the medial epicondyle and retrocondylar groove (► Fig. 28.1). Full-thickness subcutaneous flaps are elevated off the underlying investing fascia of the medial arm proximal to the medial epicondyle and off the investing fascia of the common flexor origin and flexor-pronator mass distal to the medial epicondyle. Cutaneous sensory nerve branches of the medial brachial (MBCN) and medial antebrachial cutaneous nerves (MABCN) are carefully identified and neurolysed. Osborne ligament is then identified and bisected along the line of the incision. The ulnar nerve typically lies just posterior to the medial epicondyle. Proximal and distal extension of the release can be achieved with deep retractors. Proximally, as much as the Arcade of Struthers is released, while distally the muscle fascia and heads of the flexor carpi ulnaris (FCU) muscle are bisected. Following complete decompression of the ulnar nerve, the elbow should be taken through full range of motion to observe ulnar nerve excursion and to assess instability, subluxation, or snapping. Hsu and colleagues 5 demonstrated that anterior in situ release creates significantly more total subluxation of the ulnar nerve during ulnohumeral motion than posterior in situ release. When there is significant subluxation or snapping of the ulnar nerve, transposition is carried out as outlined below. Standard layered closure is performed. A sterile soft dressing and long-arm splint (depending on surgeon preference) is applied. Early motion and nerve gliding exercises are initiated during the first week.

28.5.2 Subcutaneous Ulnar Nerve Transposition and Z-Lengthening of the Flexor-Pronator Mass
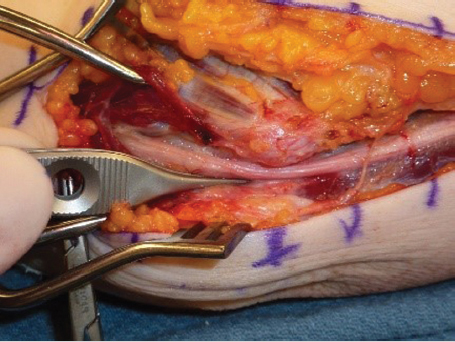
The subcutaneous transposition requires a larger incision than the in situ decompression, with about 8 to 10 cm proximal and 5 cm distal to the medial epicondyle. The ulnar nerve can be identified proximally in the arm posterior to the medial intermuscular septum. There is often an MBCN branch that innervates the posterior skin flap proximal to medial epicondyle and it may pierce the medial intermuscular septum (► Fig. 28.2). Three to five branches of the MABCN may be identified along the investing fascia of the flexor-pronator mass. The individual nerve branches can be protected with retractors or vessel loops. By keeping the incision slightly more posterior, the MABCN and its branches can sometimes be protected in the anterior skin flap.
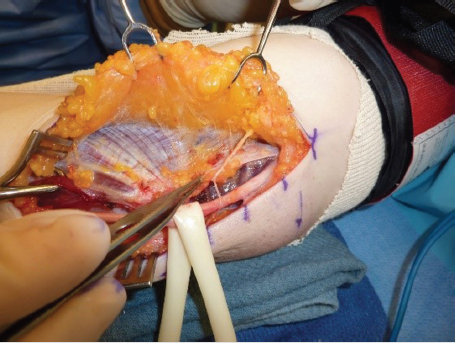
The medial epicondyle and medial intermuscular septum are identified (► Fig. 28.3). The ulnar nerve is identified along the posterior and inferior margin of the medial intermuscular septum. Retrograde neurolysis of the ulnar nerve can now be completed including generous release of the arcade of Struthers proximally. Distally, the nerve is dissected through its passage into the forearm by the two FCU heads. We attempt to leave as much of the longitudinal extrinsic blood supply and vasa vasorum with the nerve. The cubital tunnel retinaculum, Osborne ligament, and the superficial investing fascia between the humeral and ulnar heads of the FCU are released. The natural raphe between the two heads of the FCU is mobilized and the thick deep investing fascia within the two heads of the FCU that encases the ulnar nerve is released several centimeters distal to the medial epicondyle. Preservation of the anterior and posterior motor branches of the ulnar nerve at this level is paramount.
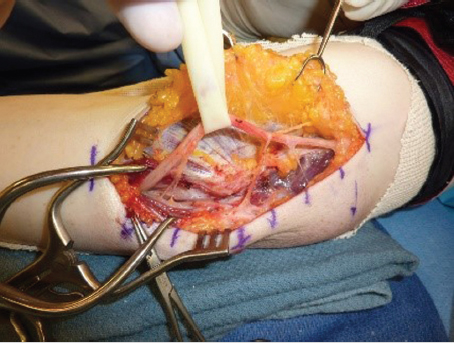
Following “top-side” neurolysis as outlined above, the medial intermuscular septum is fully excised for several centimeters. The attachments of the soft tissues onto the flexor pronator fascia are elevated anteriorly to remove any potential sites of nerve kinking once the nerve is transposed. Meticulous hemostasis is maintained and the posterior venous plexus along the posterior-inferior margin of the septum should be protected. A 360-degree neurolysis of the ulnar nerve is now completed. A Penrose drain may be used to help mobilize the ulnar nerve from its native bed (► Fig. 28.4). The longitudinal extrinsic blood supply to the ulnar nerve can be maintained with the nerve usually up to the level of the medial epicondyle. Neurolysis of the motor branches to their takeoff assists in achieving tension-free anterior transposition. The anterior position of the nerve can then be maintained in a variety of ways, from creating a tunnel by suturing the deep subcutaneous tissues onto the medial epicondylar tissues or creating a generous fascialdermal sling from the flexor pronator fascia. Standard layered closure is performed. A sterile soft dressing and long-arm splint (depending on surgeon preference) is applied.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


