25 Proximal Median Nerve Compression
Abstract
Neuropathy can be defined generally as a disorder that results in impaired motor or sensory function of a peripheral nerve. The median nerve may become neuropathic from compression at multiple anatomic sites through its course along the upper extremity. This leads to various forms of dysfunction, including pain, motor weakness, and sensory changes.
Median nerve compression at the elbow and the proximal forearm is much less common than its more distal entrapment at the carpal tunnel and represents only 7 to 10% of median nerve neuropathies. 1 There are two distinct syndromes that make up proximal median nerve compression: pronator syndrome and anterior interosseous nerve (AIN) syndrome, each of which have distinct presentations and treatments that must be carefully delineated.
25.1 Anatomy
The median nerve is composed of fibers from the fifth, sixth, seventh, and eighth cervical and the first thoracic nerve roots. It is a collection of fibers from the anterior divisions of the upper, middle, and lower trunks and the lateral and medial cords of the brachial plexus. 2 It enters the upper arm behind the pectoralis minor and passes with relative freedom until around the elbow (► Fig. 25.1a,b). There are no branches of the median nerve in the upper arm, with the exception of a possible fascicular branch variant that innervates the pronator teres (PT). Distal to the elbow, the median nerve provides motor innervation to the PT, flexor digitorum superficialis (FDS), palmaris longus (PL), and flexor carpi radialis (FCR). The nerve gives off two main branches in the forearm: anterior interosseous nerve (AIN) and the palmar cutaneous branch of the median nerve (PCBMN). The AIN supplies the flexor pollicis longus (FPL), flexor digitorum profundus (FDP) to the index and long fingers, and pronator quadratus (PQ). The nerve also provides sensory fibers to the radioulnar, radiocarpal, carpal, and carpometacarpal joints. Distal to the wrist, the median nerve provides innervation to some of the intrinsic hand muscles 3 (Box 25.1).
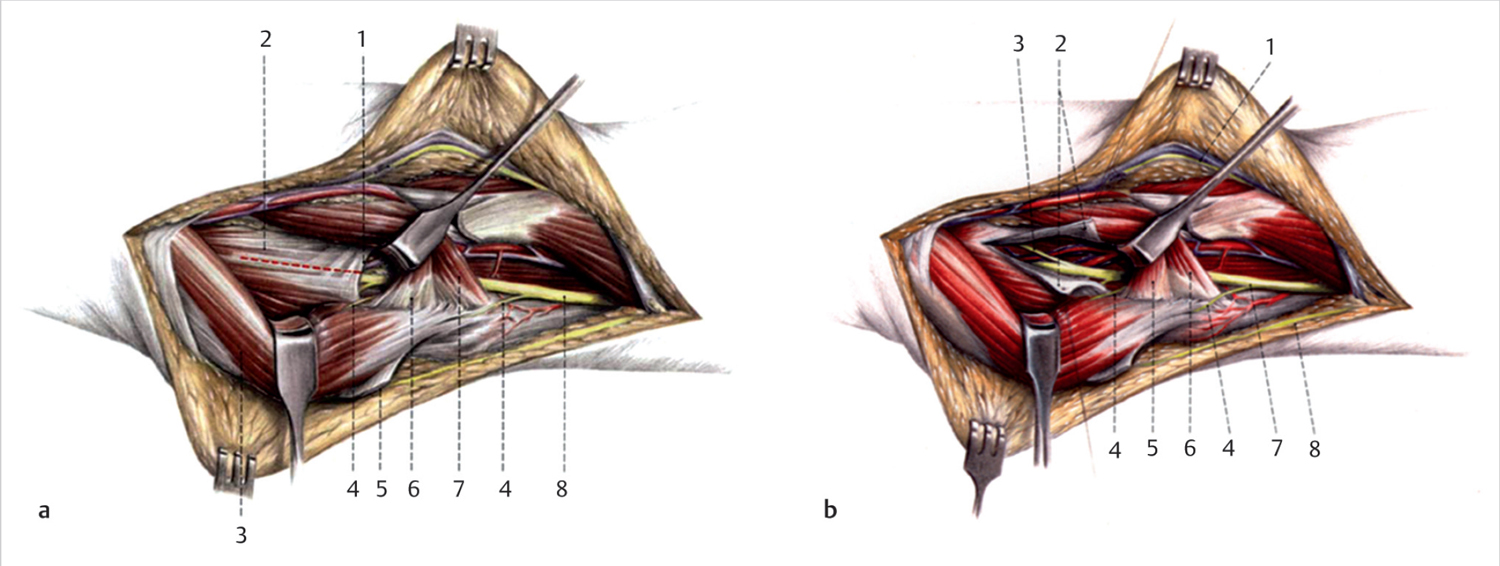
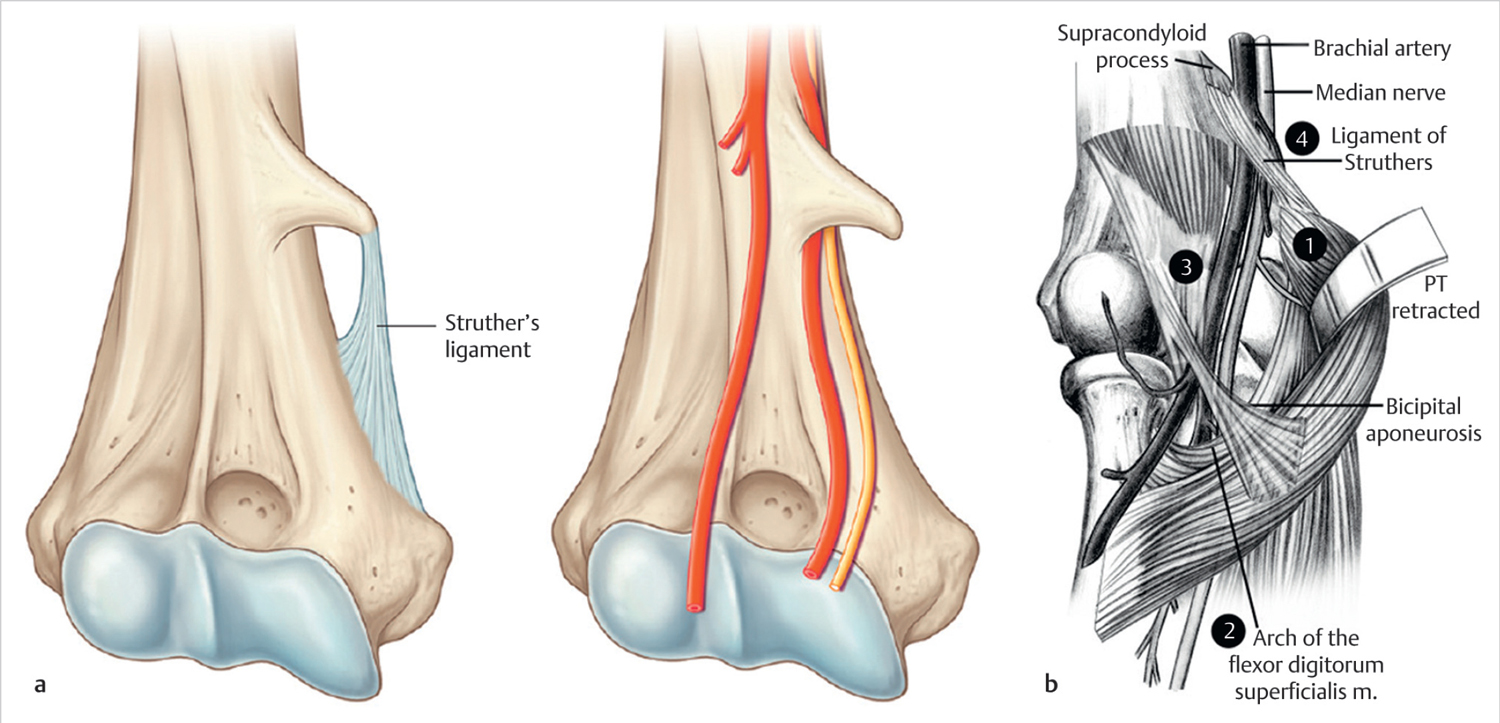
Proximal median nerve compression occurs at several distinct anatomic locations near the antecubital fossa and forearm, as the nerve traverses particular areas of constriction and/or tethering (► Fig. 25.2a,b) 4 :
Ligament of Struthers and/or supracondylar process: The ligament of Struthers overlies the median nerve as it crosses the elbow. It is thought to be a vestigial tendon and most often arises from the supracondylar process; a bony projection at the anteromedial aspect of the distal humerus approximately 5 cm proximal to the medial epicondyle. It is found in 1 to 3% of upper extremities. 5 The supracondylar process can be differentiated from an osteochondroma as the supracondylar process grows toward the joint.
Box 25.1 Median nerve innervated muscles by location
Forearm: Main branch
Flexor carpi radialis
Flexor digitorum superficialis
Palmaris longus
Pronator teres
Forearm: Anterior interosseous nerve
Flexor pollicis longus
Pronator quadratus
Flexor digitorum profundus (index and middle)
Hand
Abductor pollicis brevis
Flexor pollicis brevis (only the superficial head)
Opponens pollicis
Lumbricals (index and middle)
Lacertus fibrosus (bicipital aponeurosis): The lacertus fibrosus originates from the distal short head of the biceps tendon and is a point of static and active compression of the median nerve with biceps contraction. 6
Fascia of the PT: The median nerve passes beneath the deep/humeral head of the PT; the median nerve can be irritated by repetitive contraction of this muscle. 7 In Johnson and Spinner’s cadaveric dissection study, 20% of specimens had a fibrous arcade completely surrounding the median nerve at this location. 1
Fibrous arch formed by fascia of the FDS: The median nerve then passes deep to the proximal fibrous arch of the two heads of the FDS. Johnson and Spinner noted that 30% of median nerve constrictions occurred at this site. 1
25.1.1 Anomalous Anatomy
Additional, even rarer, sites of compression of the median nerve in the forearm include anomalous muscles or arteries: Gantzer’s muscle (an accessory head of the FPL), palmaris profundus, flexor carpi radialis brevis, or an aberrant radial artery have all been described as sites of compression. 8
25.2 Pathophysiology
The clinical findings in patients with chronic nerve compression reflect a broad spectrum of histopathologic changes. Most studies suggest a component of neural ischemia that contributes to compression neuropathies. The continuum of neural changes depends on the degree of pressure and its duration. As has been elucidated through the use of animal models, the histopathology of chronic nerve compression begins with breakdown of the blood-nerve barrier, followed by edema of the endoneurium, ultimately resulting in perineurial thickening and constriction. 9 , 10 , 11 A detailed classification of nerve injuries was first described by Seddon in 1943 12 and then expanded upon by Sunderland in 1951. 13 Under their classifications, peripheral nerve injury is subdivided into varying degrees of damage based upon the nerve structures involved. This, in turn, determines prognosis and potential treatment strategies. Compression or entrapment is just one of the basic types of nerve injury (► Table 25.1).
A nerve may be injured at multiple sites along its course and in varying gradations. It is important to recognize that one site of nerve compression may affect other sites of nerve compression. Therefore, all potential entrapment sites of nerve compression must be systematically evaluated. First introduced by Upton and McComas, 14 the double-crush phenomena states that compression of a nerve at one level will make the nerve more susceptible to damage at another level. In their clinical review of 115 patients with median or ulnar nerve compression, 81 showed evidence of a concomitant cervical root lesion. This concept of the double-crush mechanism is important in the assessment of patients with suspected proximal median nerve compression. 15 Both more proximal cervical root lesions and more distal compression at the carpal tunnel can predispose to either pronator syndrome or anterior interosseous nerve (AIN) syndrome.
25.3 Diagnosis
25.3.1 Clinical Exam
It is important for physicians who treat upper extremity disorders to be familiar with the constellation of symptoms associated with compression of the median about the elbow and forearm. A thorough differential must delve deeper than to assume that all median nerve injuries are related to carpal tunnel syndrome (CTS). To develop an effective treatment plan, it is necessary to identify and distinguish between sites of compression of the median nerve.
The diagnosis begins with a complete history. This should include common etiologies of neuropathy such as trauma to the arm, fractures, work-related repetitive use and associated medical comorbidities. Use of a pain evaluation questionnaire and diagram in the office is often helpful in identifying all symptomatic areas and other factors that may contribute to a patient’s presentation:
A patient who has AIN syndrome will often report poorly localizable pain or tenderness in the proximal forearm and antecubital fossa. This may present as an antecedent episode of pain that then resolves. This is often followed by weakness of pinch, which can manifest in difficulty with writing, buttoning, and picking up small objects. Patients may report that elbow flexion or forearm pronation worsen the symptoms. There is often no associated sensory loss with AIN syndrome. A history should differentiate this from brachial neuritis or Parsonage-Turner syndrome in which transient shoulder pain often following a viral illness precedes upper extremity weakness and paresthesia. In some cases, AIN syndrome may actually be a component of, or the end result of, Parsonage Turner syndrome.
The signs of pronator syndrome can overlap those of CTS. Both conditions are associated with pain and/or paresthesia in the hand to the radial three and one-half digits. Painful nocturnal symptoms that awaken individuals from sleep are much more common in association with CTS. 16 The classic presentation for pronator syndrome is aching forearm pain. It can be differentiated from CTS by numbness in the palm in pronator syndrome and numbness in the fingertips in CTS.
In patients with work-related symptoms, detailed consideration should be given to determine the involvement of associated activities such as those requiring repetitive, vigorous, or protracted use of the elbow or forearm. Examples of this include heavy manual labor with repetitive grasping or packaging or constant lifting and carrying or Jackhammer type activities.
The next part of the diagnosis is a thorough clinical examination with particular attention to the sensory and motor evaluation of the median nerve. The concept of increasing tension or pressure on a nerve through provocative physical examination maneuvers, such as the tests commonly used in diagnosing CTS, may be extrapolated to other sites of nerve compression in the upper extremity. This can involve direct palpation of the nerve itself or stress on a particular tendon or muscle unit. Three main provocative tests have been described to help corroborate the site of compression (► Fig. 25.3a-c):
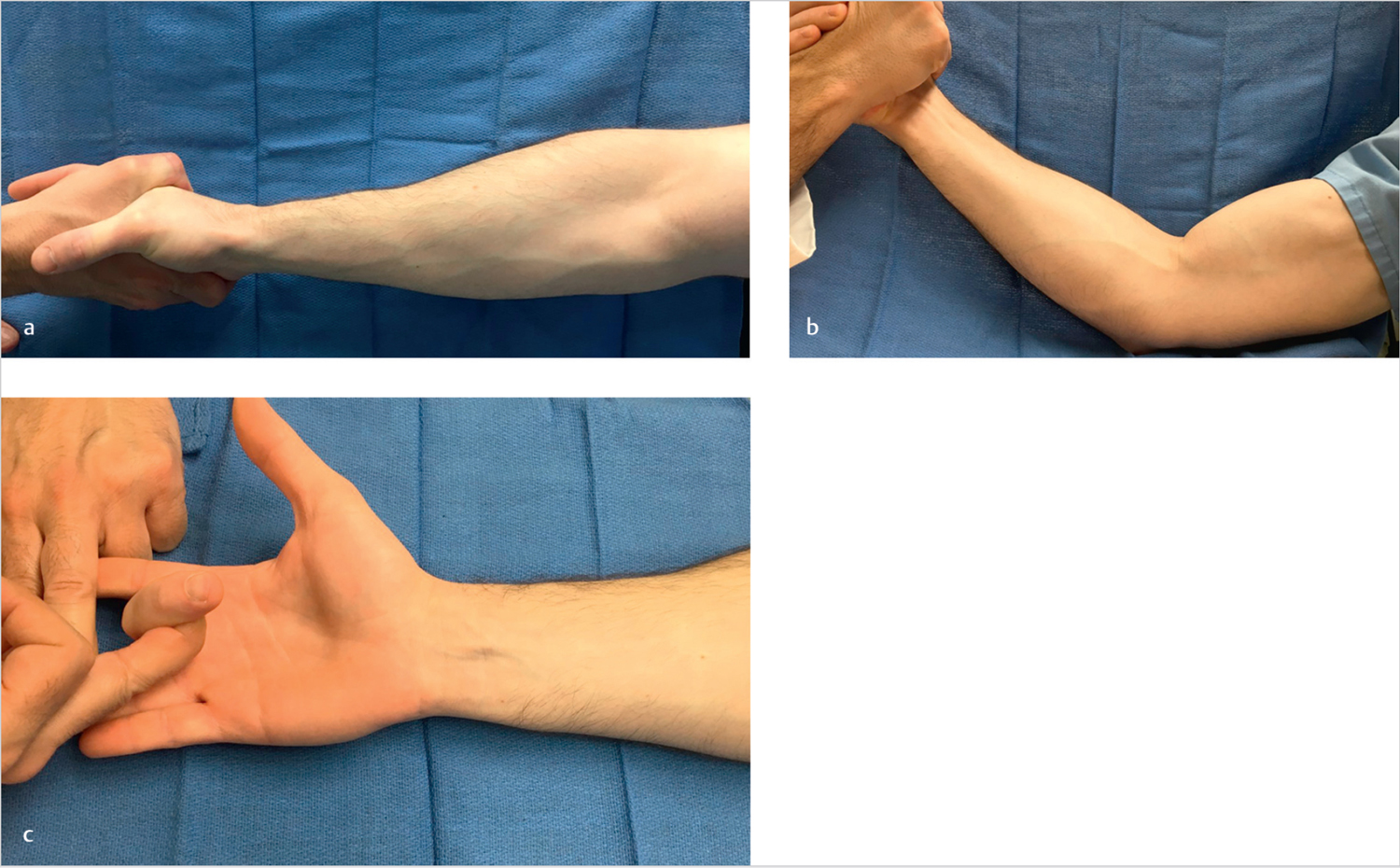
The PT muscle: Symptoms are reproduced upon resisted pronation of the forearm in neutral position with the elbow extended.
The lacertus fibrosus: Symptoms are reproduced upon resisted elbow flexion at approximately 120 flexion with the forearm in supination.
The FDS: “Proximal Phalanx (Pinning) finger flexion test.” Pain may be elicited by resisted flexion of the flexor digitorum sublimis of the long finger.
Direct compression over the median nerve at the level of the PT may reproduce some of the symptoms.
Pronator syndrome and its findings on clinical examination were first described by Seyffarth in 1951. 17 Tenderness is most localized to the origin of the PT. Weakness of the flexor pollicis longus muscle of the thumb is most pronounced. Dysesthesias are present but subtle and involve the skin overlying the thenar eminence and the palmar triangle, as this is innervated by the PCBMN. Since the PCBMN originates proximal to the transverse carpal ligament, this area is not affected in CTS and thus important in differentiating between the two pathologies. In addition, for pronator syndrome, there is no Tinel’s sign at the wrist like in CTS. The Tinel’s sign is most prominent at the main site of compression, around the proximal forearm/origin of the pronator. In CTS, several provocative tests should be performed during routine clinical examination. Phalen’s test results ranged in sensitivity from 0.46 to 0.80 and in specificity from 0.51 to 0.91; the median nerve compression test (Durkin’s) ranged in sensitivity from 0.04 to 0.79 and in specificity from 0.25 to 0.96. 18 , 19 Combining the results of these tests will aid in accurate diagnoses.
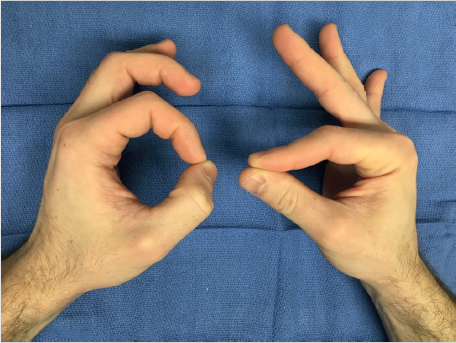
AIN syndrome was first described by Parsonage and Tumer 20 in 1948 and later by Kiloh and Nevin 21 in 1952. AIN syndrome can be partial or complete and results in paresis or paralysis of the FPL, FDP of the index, and sometimes the long finger and the PQ. This produces a characteristic pinch deformity that yields extension of the terminal joints of the thumb, index finger, and long fingers (► Fig. 25.4). Weakness or paralysis of the PQ can be demonstrated by resisted pronation of the forearm, with the elbow fully flexed to neutralize the unaffected pronator teres. With the exception of a few terminal sensory fibers, the AIN is essentially a motor nerve, and therefore, no sensory defects are found on physical examination.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


