8 The Inframammary Approach and the Dual-Plane Pocket
Summary
This chapter details the state-of-the-art templated technique for inframammary breast augmentation. This technique is the third part of The Process of breast augmentation that is the single most transcendent concept for performing breast augmentation at the highest level. The steps are precise, systematic, performed atraumatically under direct vision with prospective hemostasis.
Key Points
The new inframammary fold incision can be easily planned preoperatively lies precisely in the postoperative fold.
The dissection sequence is systematic, and templated that allows a very efficient pocket dissection.
Prospective hemostasis allows the dissection to be performed precisely, under direct vision, atraumatic, and without blunt dissection.
The majority of high level breast augmentation outcome studies have been using the inframammary fold approach.
8.1 Introduction
The inframammary approach to breast augmentation is the most scientifically validated incision in the literature. Virtually every study that has published outcomes has used this approach and the best outcome data produced have used the inframammary incision. Current advances make this incision an extremely high-quality cosmetic scar, precisely in the inframammary fold (IMF) and applicable to a wide variety of breast types. This chapter details the technical pearls for optimizing the surgical aspects of the inframammary incision.
8.2 Preoperative Markings
The patient is marked in the sitting position prior to the procedure (Fig. 8‑1 ; Video 8.1).
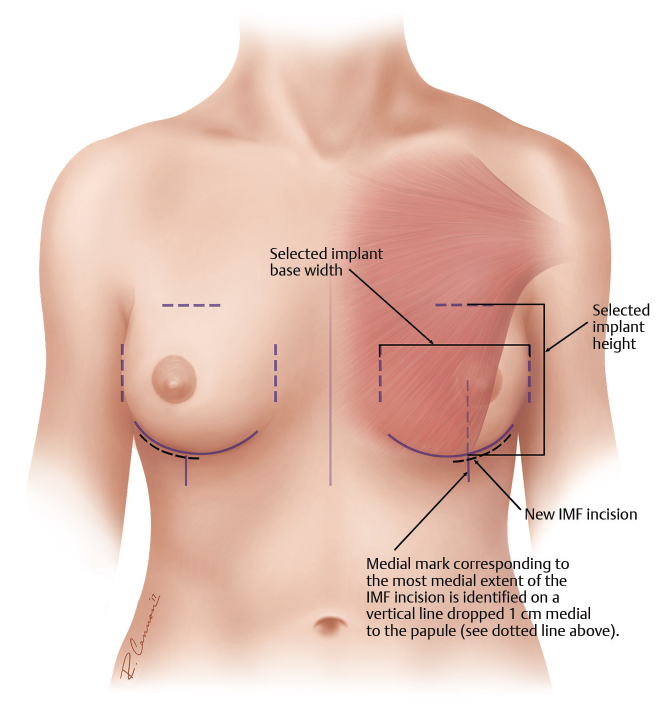
The midline and IMFs are marked for reference. The width of the pocket is marked with a caliper with a medial and lateral dot that corresponds to the width of the selected implant. The medial dot is placed at the presumed level of the medial pectoralis major m. origins and then using a caliper set to the selected implant base width, the corresponding lateral mark is placed. The height of the pocket is marked again using a caliper with a dot on the upper pole based on the height of the selected implant using the new inframammary position for the implant lower border. Finally, the exact location of the incision is marked.
8.2.1 Incision Planning
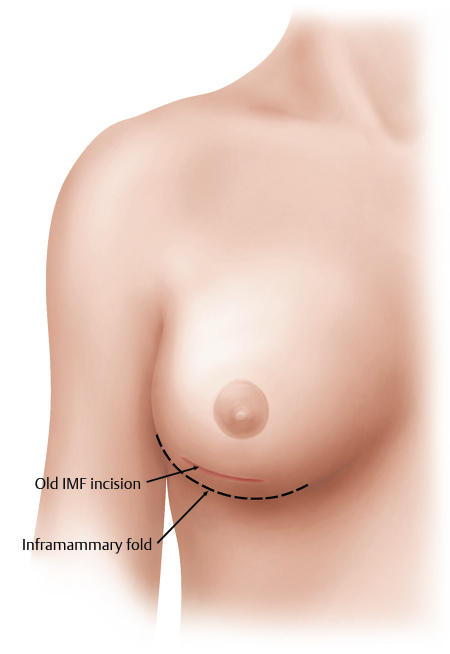
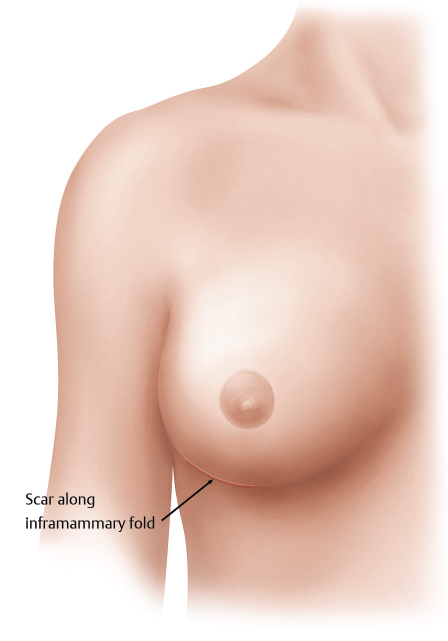
Advances in the inframammary approach to breast augmentation have led to what is termed the “new” inframammary incision. This incision is in contrast to the old inframammary incision (Fig. 8‑2), which was typically placed 1 cm above the preoperative IMF; however, this approach never yielded optimal wound healing conditions and scar placement. The “new” inframammary incision lies precisely in the postoperative inframammary crease, which may be at the same position as the preoperative IMF or may be lower than the preoperative IMF (Fig. 8‑3).
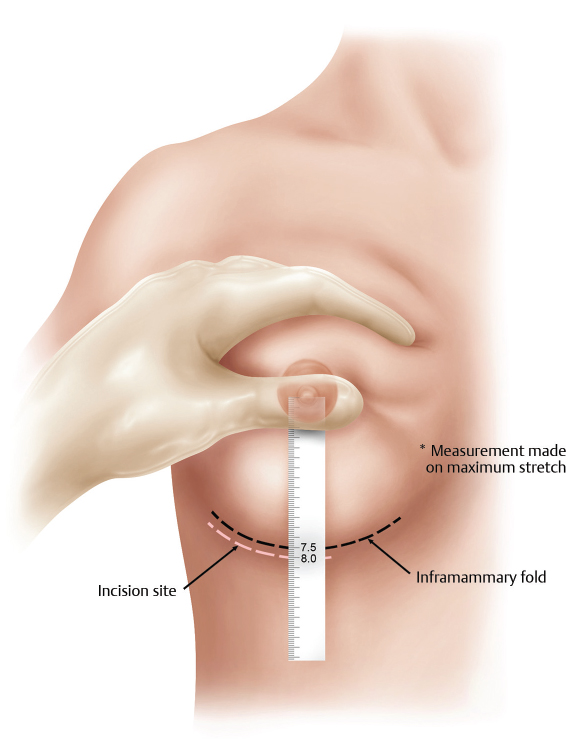
The “new” inframammary incision may be predicted by known relationships. The key relationship for incision planning is the breast base width (see Chapter 3: Tissue-Based Planning) and nipple-to-fold measurement on maximal stretch. Tissue-based planning relationships, which have been previously developed, have further refined this algorithm by using the breast width, skin stretch, and the nipple-to-fold measurement to determine implant volume that optimally fills the breast. 1 , 2 Nevertheless, these defined relationships make placing the incision precisely in the inframammary crease very reproducible. In this patient example, the breast width is 12 cm, and the nipple-to-fold measurement on stretch, as shown, is 7.5 cm.
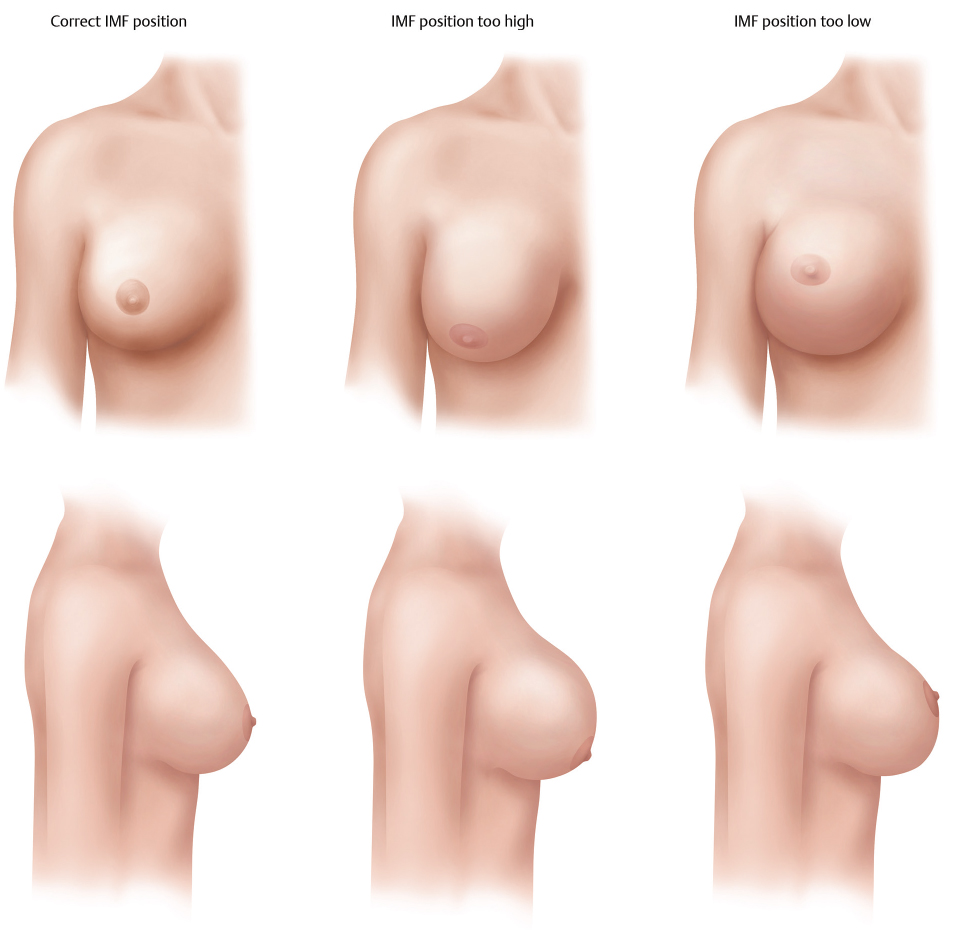
Based on the known relationships (Table 8‑1), the nipple-to-fold length immediately postoperative will be 8 cm. With the use of a plastic ruler, the nipple–IMF distance is measured under maximal stretch to determine the nipple-to-fold distance which is 7.5 cm in this example (Fig. 8‑4); therefore, the incision will be placed 5 mm below the preoperative inframammary crease, which will result in a scar precisely in the postoperative inframammary crease (Fig. 8‑5). Many surgeons do not understand this concept; however, it is essential to produce an aesthetically pleasing breast as the planned incision location also results in the final IMF position. IMF position ultimately determines breast aesthetics. Equally misunderstood is if the IMF needs to be lowered, the incision placement commits the level of the new IMF assuming the dissection is technically sound. Put another way, the IMF position passively assumes the location of the incision.
Conversely, if the IMF position is too high in an augmented breast, the breast appears to have excessive convexity in the upper pole and a downward pointing nipple (Fig. 8‑6). If the IMF position is too low, the augmented breast appears bottomed-out/inferior malposition.
8.2.2 Dissection Overview
The dissection is broken down into four primary sections (Fig. 8‑7 ; Video 8.2).
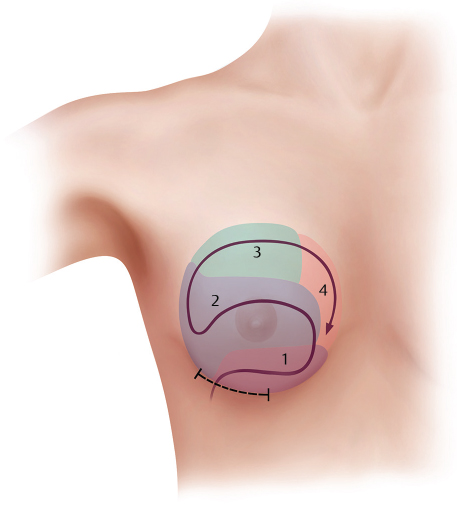
The dissection sequence will be described in its components.
8.3 Initial Dissection
8.3.1 Instruments
Five specialized instruments are recommended for this procedure. These include a double-ended breast retractor, an implant spatula, a fiberoptic non-serrated lighted retractor with smoke evacuation capability, a monopolar hand-switching electrocautery, and a good fiberoptic headlight (not depicted) (Fig. 8‑8).

8.3.2 Markings and Landmarks
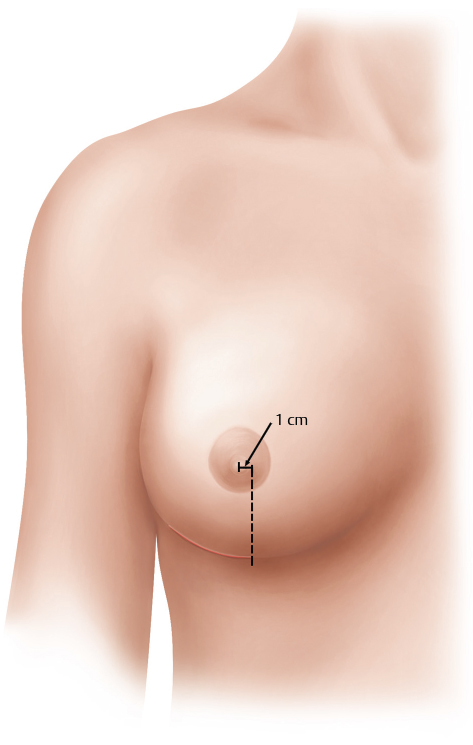
The incision is made precisely in the planned location of the postoperative IMF as described earlier (Fig. 8‑3). Generally, the most medial extent of the incision is planned from the nipple with a vertical line dropped with the patient sitting 1 cm medial to the nipple, and the incision is planned in a curvilinear fashion from that point—the length dependent on the size of the implant.
8.3.3 Incision
The length of the incision is dependent on the type and size of the implant. As the size of the implant increases the size of the incision and the same is true as the cohesivity of the implants becomes greater. The incision length should never be less than 3.75 cm for any implant type, as this is the minimum to perform a precise, atraumatic dissection under direct vision, a primary tenet of this procedure.
This also helps the surgeon avoid the temptation for blunt pocket dissection, a dated technique that results in imprecise dissection, and higher rates of complications including capsular contracture and malposition not to mention negatively affecting the overall patient experience.
8.3.4 Details of the Procedure
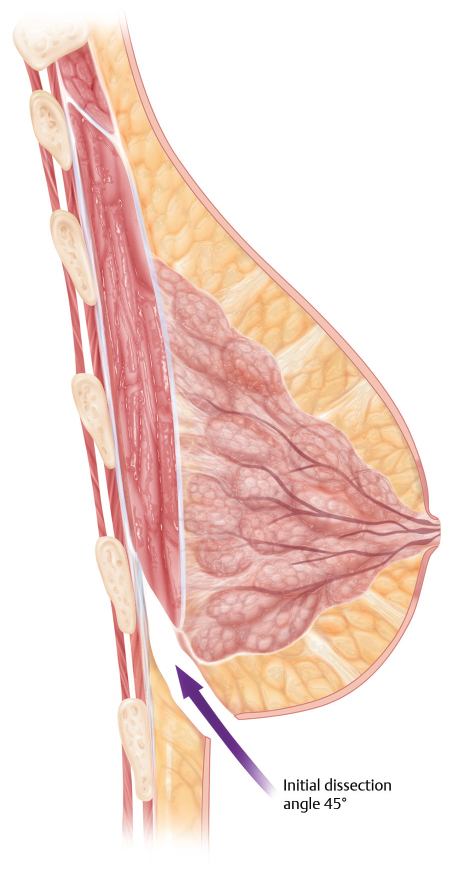
For a right-handed surgeon, standing on the patient’s right side, the skin incision is made into the mid-dermis, and initial dissection is carried through the dermis with the needle-tip electrocautery. Next, lower pole digital retraction (Fig. 8‑9) is placed on the breast allowing the initial subcutaneous dissection to proceed immediately cephalad at a vector to the medial aspect of the areola.
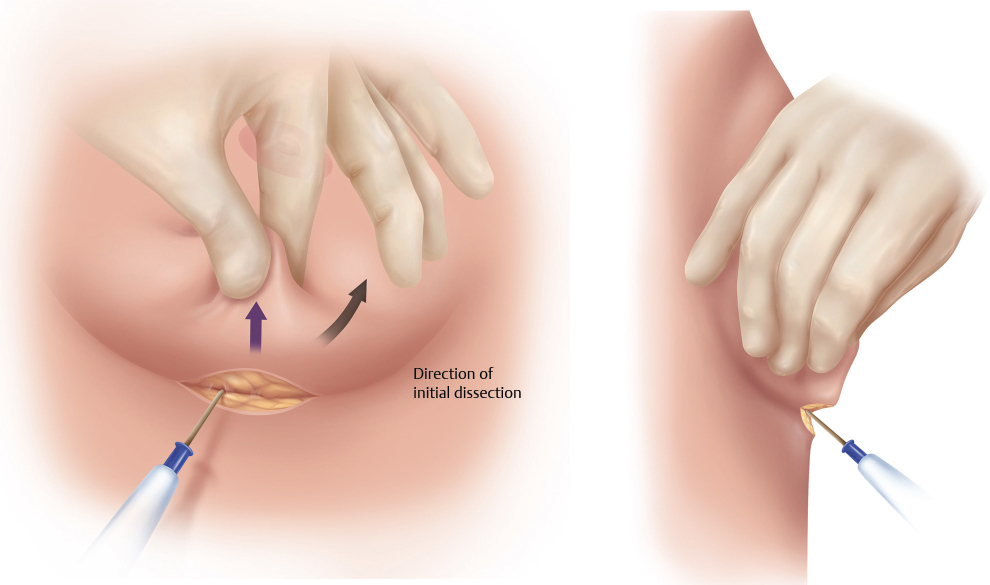
This is an important aspect of the initial procedure that avoids occult weakening of the IMF region, which can ultimately lead to postoperative deformities. Placing double hooks on the lower skin border or any other types of retraction on the lower aspect of the incision should be avoided. The dissection plane at this point is tangential away from the IMF, superiorly oriented, and deepening to the lower origins of the pectoralis major muscle 1 to 2 cm above the fold (Fig. 8‑10).
8.3.5 Pitfalls
Any type of dissection in the IMF region will result in a passive lowering of the IMF beyond its planned location; even the force of the implant in situ may overdissect this area if the IMF region is inadvertently weakened, and this underscores additional issues that arise when an implant that is too large for tissues is mis-selected. For this reason, it is extremely important to dissect immediately cephalad after the dermal incision is divided. The use of 1% lidocaine with epinephrine in the skin incision is useful to minimize any dermal bleeding, and all dermal bleeders should be cauterized before dissection is deepened to again allow optimal visualization of the pocket without blood staining.
8.3.6 Pearls
After the digital retraction, the double-arm retractor is placed to deepen the subcutaneous dissection. The double-arm retractor should be constantly repositioned every 1 to 2 seconds to provide optimal tension at the location of dissection, and this will facilitate identification of the pectoralis major muscle. Small perforating vessels will be encountered and bleeding should be controlled to avoid blood staining of the tissues. Once the pectoralis major muscle is identified, the retractors can again be repositioned, and with the anterior retraction, the pectoralis major muscle will tent anteriorly (Fig. 8‑11).
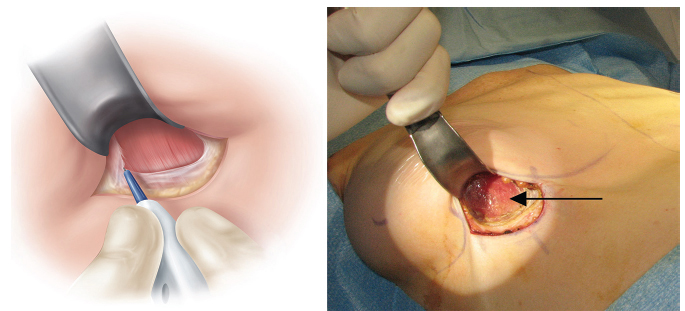
This provides a visual cue that this is the pectoralis major and not intercostal or serratus anterior muscle, and can be safely divided providing access to the subpectoral pocket. There is a misnomer that has been passed along for many years that when doing a dual-plane pocket that the dissection should be performed between the muscle and parenchyma initially, and then the subpectoral pocket. This is faulty logic, as one does not know how much to dissect between the parenchyma and muscle until the subpectoral pocket has been developed.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


