8 Free Lumbar Artery Perforator Flap for Autologous Breast Reconstruction
Koenraad Van Landuyt and Steven F. Morris
The development of the deep inferior epigastric perforator (DIEP) flap provided a major boost to the popularity of autologous breast reconstructions.1,2 Unfortunately, with this increased demand there is a growing number of patients who may not be candidates for a DIEP flap because of scarring of the abdomen or, more frequently, because of a previous contralateral DIEP flap reconstruction, previous abdominoplasty, or insufficient abdominal volume. Although several methods have been developed to try to overcome a lack of volume, including harvesting additional venous outflow, bipedicled flaps, stacking of flaps, secondary lipofilling, or even adding a prosthesis, sometimes the abdomen is just not a good option as a donor site. In addition, some patients are not willing to accept the abdominal scar.
This led to the development of alternative donor sites, mostly around the gluteal area. The first of these was the traditional superior gluteal artery perforator (SGAP) flap.3,4 However, at the dawn of perforator flap surgery, the drawbacks of a shorter pedicle, a more difficult dissection, cosmetic issues with a buttock scar, and the need of patient repositioning made the SGAP flap less desirable as an option.
New alternatives needed to be developed, and surgeons turned their attention downward to the inferior gluteal artery perforator (IGAP) flap5–7; the transverse gracilis muscle (TMG) flap,8,9 either in its traditional myocutaneous form or perforator based; and lately the profunda artery perforator (PAP) flap.10,11 Others looked for alternatives superiorly by slanting the SGAP flap superiorly, or by taking it higher on the upper part of the buttock on the septal superior gluteal artery perforators,12 to try to minimize the donor-site contour deformity, which can be another disadvantage of the SGAP flap. Now that more surgeons are acquainted with, and feel comfortable performing, perforator flap dissection, the lumbar artery perforator (LAP) flap can be a valuable alternative in selected patients.
The LAP flaps were mainly introduced as local pedicled flaps to close defects in the lower back area. In 1988, Kroll and Rosenfield13 described a local flap based on lumbar artery perforators, although the perforators were unnamed at that time. Other authors clarified the use of local LAP flaps for reconstruction of the lumbosacral region.14–17
The free LAP flap was first published as a case report in 2003 by de Weerd et al,18 as an alternative free flap for autologous breast reconstruction. Though the LAP flap has gained greater acceptance, until now no major series have been published.
Anatomy
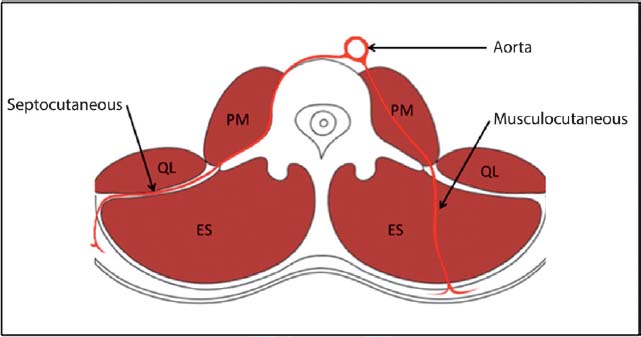
Four pairs of lumbar arteries arise from the posterior lumbar aorta. These are large 4-mm vessels that pass posteriorly to supply the posterior lumbar angiosomes including muscle, skin, and bone. The lumbar arteries then pass along the vertebrae and between the transverse processes before splitting into dorsal and abdominal branches. The dorsal branches have a variable course through the psoas major, quadratus lumborum, and erector spinae muscles or through the intermuscular septa ( Fig. 8.1 ). The lumbar arteries anastomose freely with each other and the other main source vessels in the region, including the intercostal, subcostal, iliolumbar, and deep circumflex femoral arteries. The dorsal branch also gives off a spinal branch, which enter the vertebral canal. There have been several previous reports of the vascular anatomy of the region.19–22
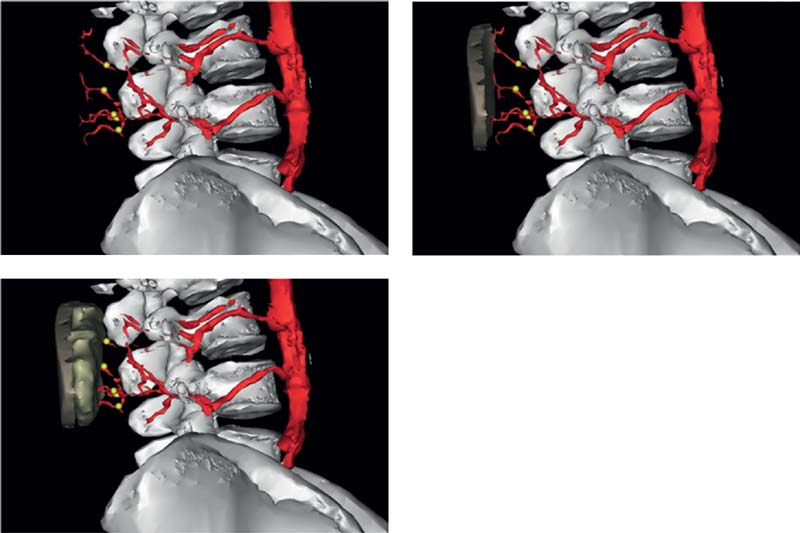
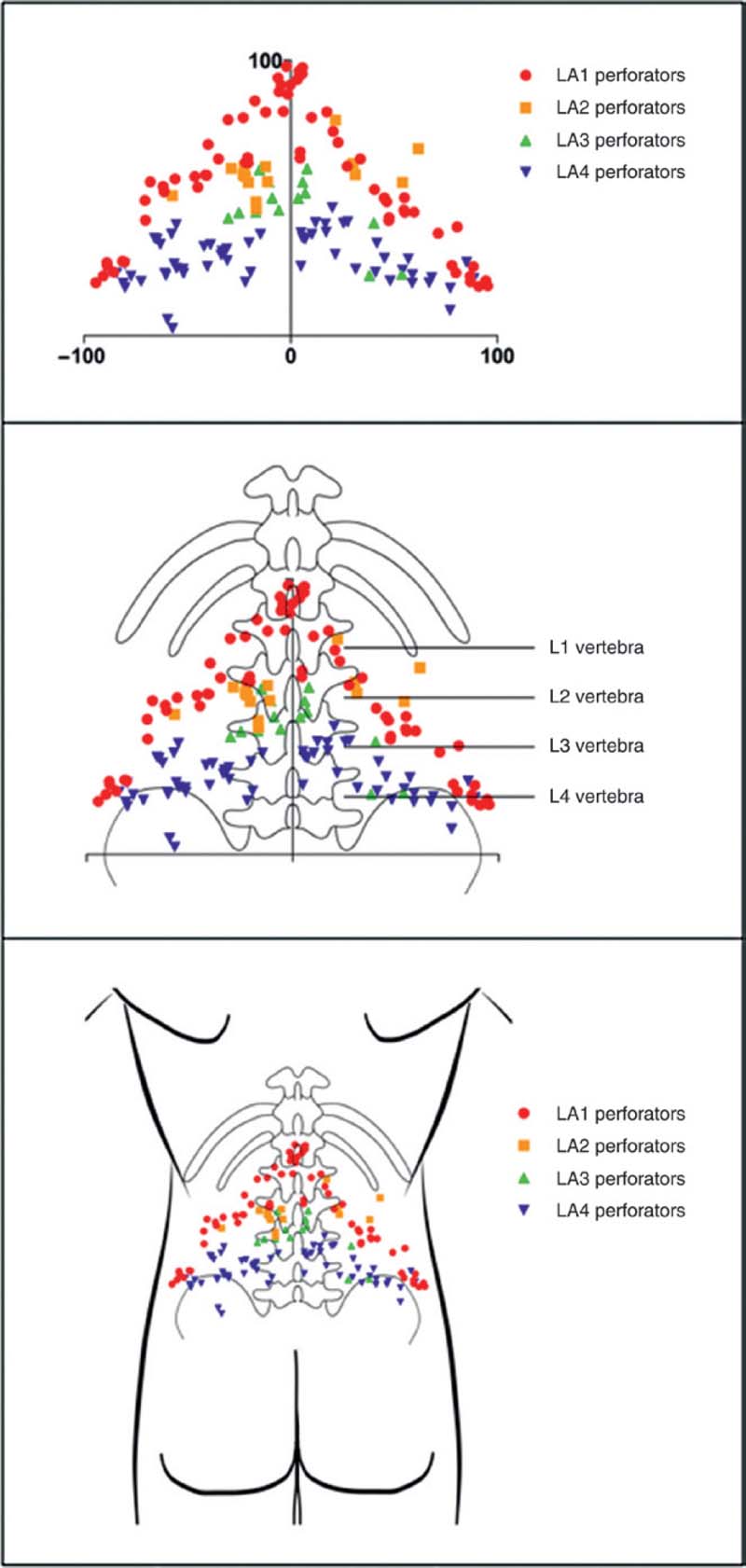
In a study of seven fresh cadavers injected with lead oxide, we performed three-dimensional (3D) angiography to capture the distribution, size, and course of the lumbar artery perforators, which arise from the paired lumbar arteries (L1, L2, L3, and L4)23 ( Fig. 8.2 ). Most pairs pass posterior to the quadratus lumborum, but some take a route through the muscle. The L1 to L3 arteries course between quadratus lumborum and the erector spinae muscles, whereas the L4 vessels generally pass anterior to quadratus lumborum. Once the lumbar arteries pass the lumbosacral fascia, they branch into smaller vessels supplying the lumbar integument. We observed that the individual perforator anatomy was quite variable, but in general the L4 perforators were often septocutaneous, whereas the L1 perforators were mostly musculocutaneous. Individual perforator anatomy was highly variable but septocutaneous perforators usually passed between the quadratus lumborum and erector spinae. Computed tomography angiography (CTA) shows the 3D course of lumbar artery perforators. More perforators arise from the L1 and L4 than from L2 and L3. Perforators measure ~1 mm in diameter where they penetrate the lumbosacral fascia ( Fig. 8.3 ).
Indications
The DIEP flap reconstruction remains the workhorse of autologous breast reconstruction, as it does in our hands. However, as mentioned above, some patients seeking autologous reconstruction are not especially good candidates for DIEP flap reconstruction. Patients who underwent a failed DIEP flap procedure or who developed a secondary tumor in the contralateral breast after a previous DIEP flap reconstruction cannot have another DIEP flap. Also, some patients are seeking preventive bilateral subcutaneous mastectomy and immediate reconstruction because of genetic or familial breast cancer predisposition.
Surgical Procedure
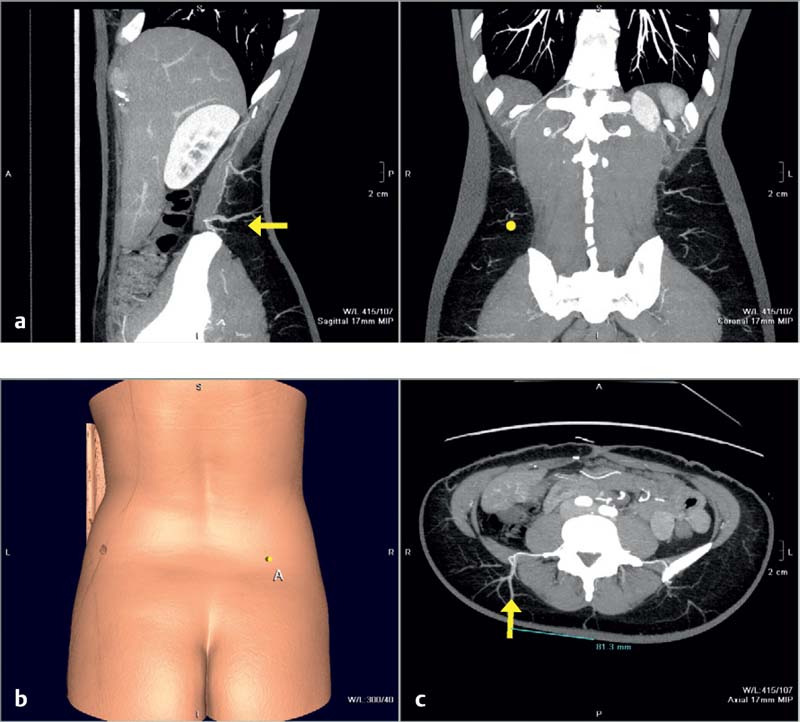
Before surgery, the size, position, and course of the lumbar perforators is checked on a preoperative computed tomography (CT) or MRA scan. The patient should be positioned face down for the scan, so that the gluteal/lumbar perforators are not compresses. The X-axis is provided either by a horizontal radiopaque marker or by the height of the iliac crest ( Fig. 8.4 ). The lowermost lumbar perforator (L4), crossing the posterior iliac crest, is usually preferred to enable positioning of the scar as low as possible.
With the patient in standing position, the skin island is marked as needed on top of the posterior iliac crest, pinching the posterior “love handles.” The skin island is marked as low as possible above the gluteal prominence, slightly slanting upward from medial to lateral, mimicking the skin excision of a posterior buttock lift; however, care should be taken not to cross the posterior midline. In a primary breast reconstruction, the skin island should be kept as small as possible to avoid problems with donor-site closure; skin islands of 8 to 10 cm can be fairly easily closed. Vertical marks enable perfect closure of the donor site ( Fig. 8.5 ). If a bilateral procedure is planned, the opposite side is marked symmetrically and covered with an OpsiteR (Smith & Nephew, Andover, MA) dressing to save the drawings until the second intervention ( Fig. 8.6 ).


Markings on the chest are also performed with the patient in the standing position, including a small incision line in the groin area for the eventual harvest of an inferior epigastric pedicle graft.
The patient is repositioned on the operation table, face down, for transfer of the CT markings of the perforator in the same position as the patient was positioned in the scanner ( Fig. 8.7 ). Markings can be adjusted slightly to include the emergence of the perforator in the design of the flap, but should be kept as low as possible to prevent a high-rising scar.

After intubation and preparation of the patient (two peripheral IV lines, bladder catheter), she is placed in the lateral decubitus position, with the torso slightly twisted and the shoulder back to enable simultaneous surgery of the donor (LAP flap) and recipient (breast, vascular graft) sites; the ipsilateral arm is fixed in 90 degrees of flexion and 90 degrees of abduction, enabling eventual positioning of the microscope over the chest ( Fig. 8.8 ). Positioning of the patient should accommodate flexing the bed at the lumbar level, facilitating the dissection; breaking is released at the time of closure.

The exact position of the perforator is identified by Doppler evaluation at this time ( Fig. 8.9 ).

Surgery starts simultaneously on both the recipient site and the donor site. At the recipient site, a subcutaneous mastectomy is performed in the usual way, taking care to identify and spare for some length the medial and lateral branches of the fourth intercostal nerve supplying the breast. If a sentinel node dissection or lymphadenectomy has to be performed, a separate incision is preferred. The mammary vessels are dissected free after partial removal of the medial fourth costal cartilage, again leaving the vessels as long as possible. The vessels are not divided yet, to avoid twisting of the pedicle.
If a vascular graft is deemed necessary, the inferior epigastric vessels are approached through a small inguinal incision. The distal part of the epigastric pedicle is dissected over a length of 5 to 6 cm, from the exit point out of the rectus abdominis muscle, up to the collateral venous confluence; it is harvested and flushed with heparinized physiological solution ( Fig. 8.10 ).

The donor-site dissection of the LAP flap starts with an incision of the skin island on its superior, anterior, and inferior border, temporarily leaving the area over the perforator. The upper incision is slightly beveled and carried on to the underlying muscle fascia.
The upper beveling serves to provide upper pole fullness and avoids shelving, a problem typically encountered with the traditional SGAP flap. The lower beveling provides volume and projection to the breast. The main bulk of the flap is harvested on the inferior side, which is beveled as necessity, scooping the fat underneath the iliac crest, leaving the layer above the superficial fascia to avoid donor-site depression after closure. A large volume of tissue can be harvested in this way; care should be taken not to overdo the volume, as this can lead to a problem of depression at the donor site, necessitating secondary corrections ( Fig. 8.11a ).
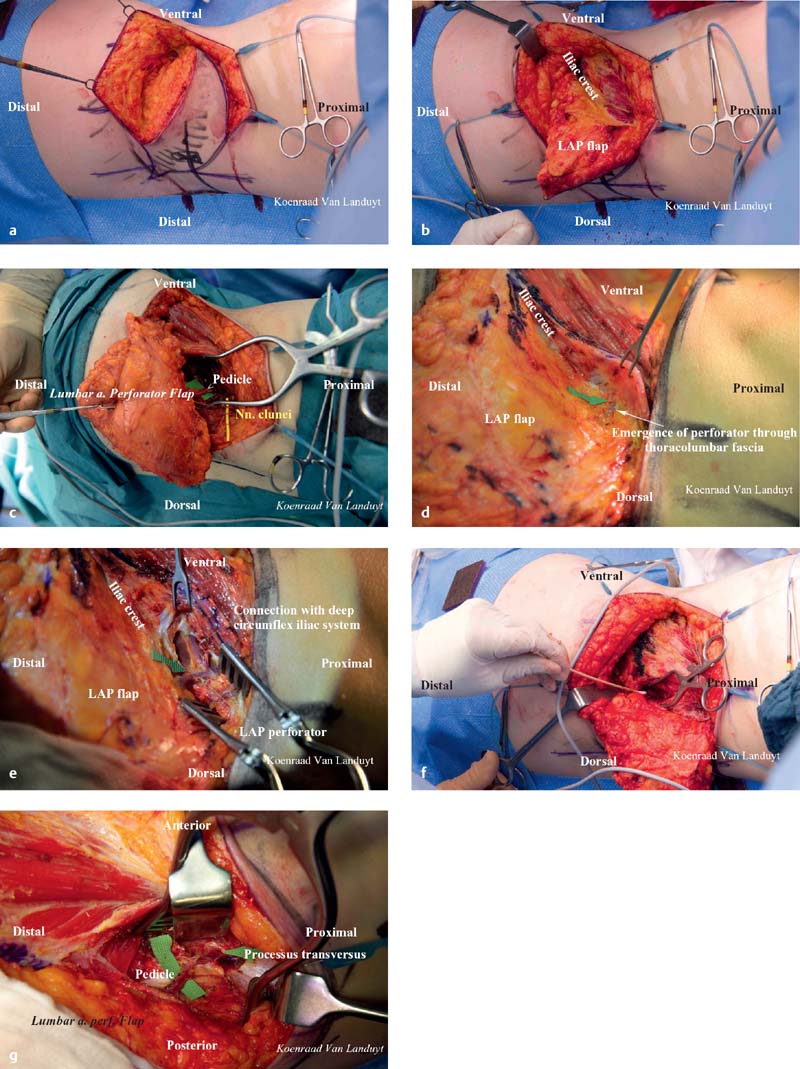
The flap is harvested from anterosuperior to posteroinferior on top of the obliquus externus muscle fascia, at first identifying the iliac crest. To limit donor-site morbidity, and especially seroma formation, one should avoid skeletonizing the iliac crest. Dissection below the iliac crest is superficial to the gluteus medius muscle, until one reaches the lateral edge of gluteus maximus. Perforators from the superior gluteal pedicle (septal perforators) can be identified here and temporarily spared as backup. The flap is allowed to fall backward in the process, which facilitates exposure.
Once the iliac crest is identified over a certain length, the upper skin and subcutaneous incision can be carried on, to enable approaching the lumbar perforators. Dissection is carried posteriorly on top of the muscle fascia. Based on the CT scan, the perforator can be anticipated close to the posterior iliac spine, or slightly higher in the space between the quadratus lumborum and spine musculature. Identifying the perforator here is the difficult part of the dissection, as the perforators tend to be compressed by the thoracolumbar fascia rendering them smaller and difficult to visualize. A hint can be the spot on top of the iliac crest where the muscle fascia of latissimus dorsi merges with the thoracolumbar fascia ( Fig. 8.11b ). Sharp incision of the thoracolumbar fascia at this point facilitates subfascial dissection.
Once the perforator is identified, it is carefully freed from the surrounding tissue, ligating connections with the superior gluteal artery perforators and the deep circumflex iliac vessels. This dissection can frequently be performed by bluntly with the aid of a cotton tip. Cluneal nerves can be identified that cross the iliac crest almost together with the perforator, but they follow a different course, running up in between the fibers of the spinal musculature ( Fig. 8.11c ). One or two of these nerves can be dissected out bluntly for a substantial length of 8 cm or more. Sensory denervation by harvesting them is limited to the flap itself and the upper part of the buttock, which seemingly does not pose a problem to the patients ( Fig. 8.11d,e ).
Blunt dissection of the perforator with a cotton tip is carried on upward and into the depth of the intermuscular septum between the quadratus lumborum and the erector spinae musculature, carefully ligating or bipolar coagulating muscular side branches ( Fig. 8.11f ). Dissection is stopped at the level of the processus transversus, regardless of the length or size of the pedicle ( Fig. 8.11g ), to avoid injuring the spinal nerves emerging from the foramen intervertebrale in front of the processus transversus. Pedicle lengths of 5 to 7 cm can be obtained with the size of the vessels equaling those of the superficial epigastric artery perforator flaps (1- to 2-mm diameter). After harvesting of the pedicle and control of hemostasis, a small resorbable hemostatic wick is left in place at the site of pedicle harvesting. The pedicle itself is flushed with heparinized solution.
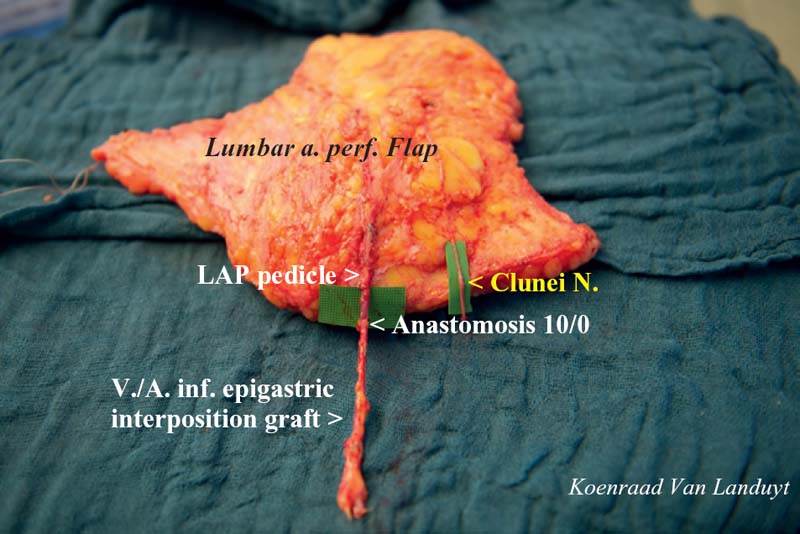
Fig. 8.12 demonstrates the LAP’s resemblance to a mastectomy specimen.

As the LAP flap donor site is prone to seroma formation, careful closure of the donor site is mandatory. To obtain a buttock lift effect, undermining is continued but only inferiorly on top of the buttock musculature. If feasible, the gap in the thoracolumbar fascia is closed with interrupted resorbable sutures. The region around the iliac crest is injected subfascially with a long-acting local anesthetic to reduce postoperative pain. Two drains are left in place, tacking sutures are applied, and the wound edges are carefully approximated, following the preoperative vertical markings. Prior to closure, the wound is rinsed with an antibiotic solution.
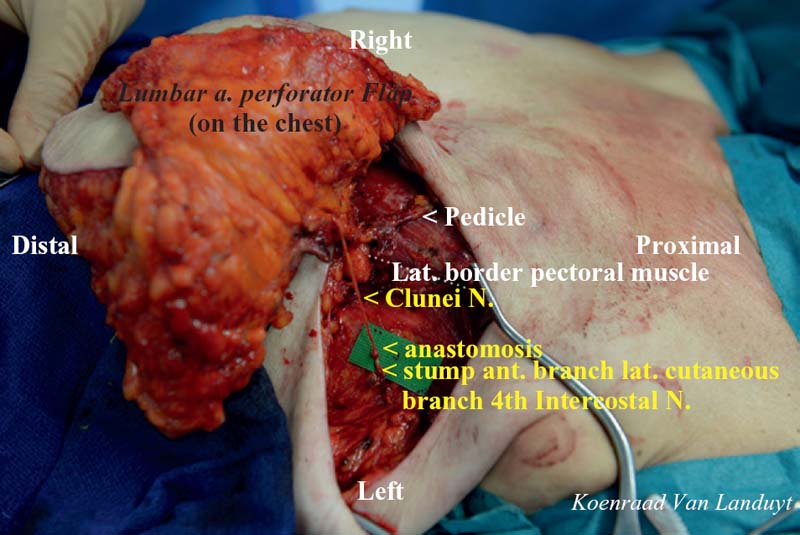
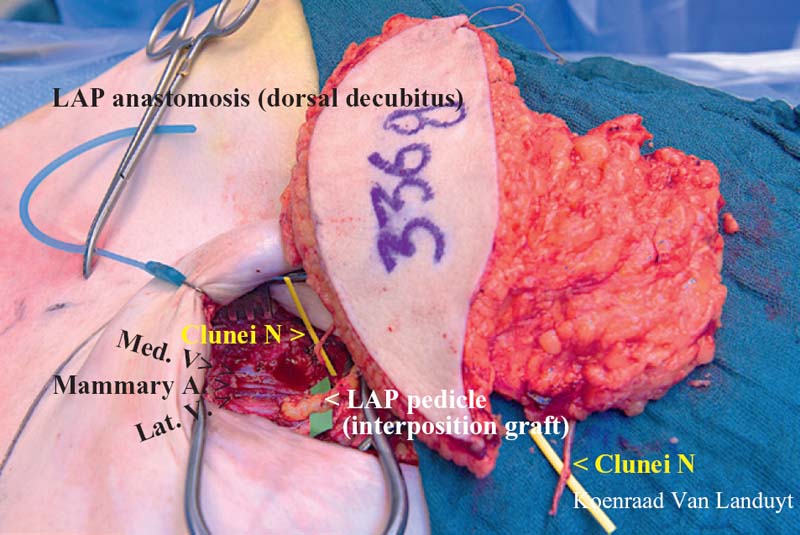
If the pedicle is deemed of sufficient length and size, direct anastomosis with the mammary vessels can be performed with the patient in the lateral decubitus position ( Fig. 8.13 ), in the meantime closing the donor-site defect. Vessel length is frequently less of an issue than vessel size incongruence. The distal end of the inferior epigastric pedicle matches the mammary vessels quite nicely most of the time. In addition, the epigastric vessels taper down rather fast in their proximal part at the edge of the rectus abdominis, matching the lumbar vessels if taken shorter, which make the epigastric pedicle a good interposition graft of ~5 to 6 cm. Nowadays, we tend to more frequently use this interposition graft as compared with our initial experience with the LAP flap, a trick we tend to use also in the occasional SGAP reconstruction to avoid vessel anastomotic incongruence. The interposition graft is anastomosed end to end, artery to artery, and vein to vein, with 10-0 sutures, on a side table in about the time it takes to close the donor site ( Fig. 8.14 ). Then the patient is placed in the supine position and an end-to-end anastomosis to the mammary vessels with 9-0 sutures is performed ( Fig. 8.15 ), and the nerve coaptation of the cluneal nerves is performed with the lateral or medial intercostal nerves ( Fig. 8.16 ). After control and careful positioning of the pedicle, the flap is shaped and inset; in cases of primary areola-sparing mastectomy, a small skin island is left in place for monitoring and for the nipple reconstruction. The flap is positioned as it is harvested, the thinner beveled upper side in the superomedial part of the breast, the thicker major inferior part of the flap in the lower part of the breast, eventually slightly folded underneath to provide for extra projection. Care should be taken to slightly overdo the medial upper filling to anticipate some secondary sagging of the flap. One drain is left in the breast.

Operative time is about 4 hours skin to skin. Including patient marking and positioning, this amounts to a total operative time of about 5 hours. If bilateral reconstruction is planned, surgery is scheduled 2 to 3 days apart. This limits hospitalization. Convalescence is one period of about 6 to 8 weeks.
Postoperatively, the patient is monitored for 1 day in the recovery unit, and kept in a semiupright position to alleviate the weight of the flap on the anastomosis, which sometimes is protected by pulling it through a short piece of silicon drain that is left in place. A Bair HuggerTM device (3M, St. Paul, MN) is applied until the patient regains normal body temperature; no specific anticoagulation is given apart from the usual postoperative low molecular weight heparin.
Drains in the gluteal area are left in place for ~ 10 days, even if the patient is usually discharged at the fifth postoperative day. Mobilization of the patient starts on the second postoperative day; at this time the bladder catheter and breast drain are usually removed. The patient should wear a lumbar/gluteal compressive garment (contour correcting underwear or lipo-panty) with additional pressure pads at the donor site for at least 6 weeks and should be scheduled for weekly ambulatory control for the first 6 weeks to solve issues of eventual seroma formation. A paper tape (MicroporeR, 3M) is applied on the incision for ~3 months to control scar formation.
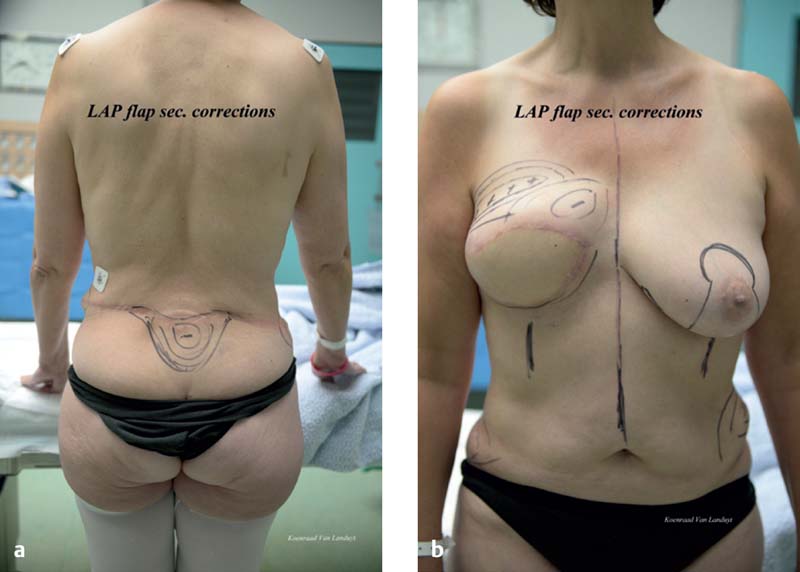
Secondary corrections are performed 3 to 6 months after the initial surgery including the usual nipple reconstruction, symmetrization of the breasts, and scar corrections. As to the donor site, symmetrization is also performed at this time by liposuction/lipofilling if necessary ( Fig. 8.17 ).
Related posts:
 2 Starting a Perforator Flap Breast Program
2 Starting a Perforator Flap Breast Program
 4 Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
4 Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
 10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
 9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
 13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
 11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


