8 Deep Chemical Peels
Key Concepts
New is not necessarily better.
A tool is just that … a tool.
If the only “tool” one knows how to use is a hammer, everything begins to resemble a nail.
The nature of machines is to malfunction… at the worst possible time.
The more complex the machine, the more apt it is to malfunction.
Introduction
Often referred to in nonphysician circles as a “non-surgical facelift,” chemical exfoliation remains the gold standard for treating advanced wrinkling and solar elastosis of the face. Creative ways to apply peeling solutions and modifications in formulations and concentrations do not change the fact that the materials cause a separation of the upper layer of skin, which peels or sheds within a few days. The amount of peeling or shedding is directly related to the depth of injury, a factor that is dependent on the kinds—and caustic nature—of chemicals used.
Although other methods of exfoliation are effective in removing superficial signs of aging and sun-damaged skin, in the author′s experience, level II and III peeling with the original Baker-Gordon peel formula ( Table 8.1 ) has proven to stand the test of time; therefore, the author has seen no reason to modify the formula. It has also been the author′s experience that the depth of injury depends upon several factors, only one of which is related to the chemicals chosen and the formulation of such chemicals with other agents. Penetration can also be affected by adjusting the mechanical act of degreasing the skin that is to be peeled, the number of times that a peeling solution is applied to the treated area, the amount of solution applied with each application, and how well a patient complies with good wound healing principles and instructions following the procedure. Using the same formulation (Baker-Gordon formula), it is possible to do a level II or level III peel on the same patient; it all depends on the factors mentioned in the preceding sentence.
In short, chemical peeling is both an art and a science. There is no one-size-fits-all formulation or application method for all skin types. The treatment plan for each patient must be individualized. Even on the same face, skin thickness varies, requiring more—or less—aggressive treatment. In this regard, the outcomes of treatment are very much determined by the skills and experience of the surgeon as well as patient compliance.
Background: Basic Science of Procedure
With all peels, dermabrasion, and laser resurfacing techniques, outer layers of the skin are removed. However, only with more penetrating (levels II and III) procedures are new collagen and elastic fibers produced in the deeper layers of the skin. As a result, some tightening of facial tissues occurs (more with level III peels than with level II peels), but, in either case, not to the extent that can be achieved with conventional facelifting and eyelid-lifting techniques.
As a rule, light (level I) peels do not produce long-term improvement in the quality and texture of the skin but may be used as adjuncts to the methods herein described for continued maintenance.
Neither a facelift, eyelid surgery (blepharoplasty), nor a brow lift will remove wrinkles that have been etched into weather-beaten skin, transverse creases of the forehead, “crow′s feet” around the eyes, or vertical wrinkles of the upper and lower lips. A good principle to remember is: surgery improves sags and bulges, whereas resurfacing improves wrinkles. And, with respect to skin resurfacing techniques, it has been the author′s experience that dermabrasion is the treatment of choice for acne scarring or for the second and third stages of surgical scar revisions that required excision and wound resuturing. The author has had extensive experience in laser skin resurfacing and has found it to be helpful but not as effective in treating deeper facial rhytids with chemical peeling, nor in treating acne scarring as with wire brush dermabrasion.
To assist the profession in clearing some of the confusion regarding depth of treatment, the author developed a classification system (based on depth of injury) that applies to peels, dermabrasion, and laser resurfacing:
Level I—Superficial (Spa peels, commercially available topicals such as glycolic and salicylic acid peels, etc.). Level I peels are temporary skin polishers and do not effectively rejuvenate wrinkled, scarred, or cancer-prone skin, no matter how often they are repeated.
Level II—Medium Depth (TCA-based or modified phenol-based peels). Level II peels are more effective than level I peels in that more layers of damaged and wrinkled skin are removed. Healing time generally requires about a week. Level II procedures are generally recommended for patients less than 50 years old or those with minimal to moderate sun damage and wrinkling.
Level III—Deep (Wire brush abrasion and Baker-Gordon phenol-based, croton oil peels). Level III peels are the most effective methods of removing severely sun damaged, blotchy skin and deeper wrinkles. Healing time is longer—generally 2 weeks or more. However, results are long-lasting and often dramatic.
Patient Selection
As mentioned in a previous paragraph, different areas of the face require different types of treatment. In full-face resurfacing, the author often combines level II and level III peeling. Level II peeling is effective in treating eyelid rhytids and in blending from treated into nontreated regions (i.e., from the skin overlying the mandible into the shadow line below or into the hairline). And, using the Baker-Gordon formula, it is not necessary to change formulations from one region to the other. Simply modifying the technique of application provides transition from level II to level III. An experienced surgeon will know how to vary the depth of the treatment to meet the patient′s specific needs.
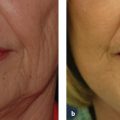
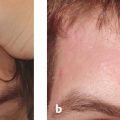
The author′s Facial Rejuvenation Classification System allows surgeons to quantify the condition of each patient′s skin, eyelids, and face ( Tables 8.2 ; Table 8.3 ).1 Abbreviations have been assigned to each of the regions and structures of the face. A score of 0 through 5 is then assigned to each abbreviation, with 0 being the ideal and 5 being the most advanced signs of aging. Once the condition of each region is determined, it is a matter of choosing the most appropriate technique of either surgery and skin resurfacing or both and performing the procedure(s) in a precise and reliable manner. Fig. 8.1a–d demonstrates how the McCollough Facial Rejuvenation Classification was applied in one patient′s total facial rejuvenation.
Anyone performing facial exfoliation must understand and remind patients—in advance of treatment—of the length of time required for healing, especially for level II and III resurfacing procedures. Regardless of the source of injury (peeling, dermabrasion, laser), unless it takes a minimum of 2 weeks to heal, results will generally fall short of the doctor′s and patient′s expectations. In that regard, “no downtime equals no long-term improvement.”
Relative contraindications for phenol-based chemexfoliation include active herpes infections, unrealistic expectations, unreliable patient, the skin of the neck, and diseased state of any organ system that breaks down—or is sensitive to—phenol (liver, kidney, and heart). In the end, the decision to perform chemical peeling lies with the surgeon, who must weigh the potential risks against the benefits of any procedure.

Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


