73 Management of Vascular Anomalies: Hemangiomas and Malformations
Introduction
Vascular anomalies represent a heterogeneous group of lesions affecting vascular and lymphatic channels. Historically, the nomenclature used for these lesions has been dominated by inconsistent descriptive and vernacular terms (e.g., cherry, strawberry, portwine stain, capillary, and cavernous) resulting in confusion among clinicians and errors in diagnosis and treatment. In 1996, the International Society for the Study of Vascular Anomalies accepted a dichotomous classification scheme for vascular anomalies based on distinct cellular and clinical characteristics. 1 This scheme identifies lesions as vascular tumors, which are true neoplasms characterized by epithelial proliferation, or vascular malformations made of dysmorphic vessels with normal endothelial turnover ( Table 73.1 ). Careful medical history and physical examination can differentiate more than 90% of vascular anomalies into one of these categories. 2 Despite a standardized nomenclature for over 15 years, a recent review of 320 publications on vascular anomalies found 71% of publications incorrectly identified these lesions, resulting in improper treatment in over 20% of patients. 3 Since many of these lesions occur in the head and neck and not infrequently require surgical management, it is imperative that facial plastic and reconstructive surgeons are familiar with the diagnosis and treatment of these lesions.
Vascular tumors | Vascular malformations |
Infantile hemangiomas | Slow flow |
Congenital hemangiomas |
|
|
|
|
|
Kaposiform hemangioendothelioma | High flow |
Tufted angioma |
|
Pyogenic granuloma |
|
Angiosarcoma |
|
Vascular Tumors
Infantile Hemangiomas
Infantile hemangioma (IH) is the most common benign tumor of infancy. The exact cause of IH remains unknown, but several risk factors for their development have been established. Fair-skinned individuals are at higher risk with rates up to 10% among Caucasian infants. 4 Premature birth is associated with IH, and the number of hemangiomas per infant increases with younger gestational age. Females are more likely to develop IH than males (3:1), but this is less pronounced (1.8:1) among premature infants. 5 Low birth weight, especially below 1,500 g, increases the likelihood of IH independent of gestational age; every 500-g reduction in birth weight imparts a 40% increased risk of IH. 6 Advanced maternal age, multiple gestation pregnancies, and placental factors such as placenta previa, history of chorionic villous sampling, and preeclampsia are also associated with higher rates of IH. 4 , 5 IHs are more common in families with 10 to 33% of affected infants reporting a first-degree relative with a vascular anomaly and up to 12% with a known IH. 4 , 7 However, a definite genetic link or pattern of inheritance has yet to be established.
Clinical Presentation and Natural History
IHs are typically not visible at birth, but up to 30% are evident as precursor lesions with variable findings including a telangiectatic macule, pale vasoconstricted area, vascular stain, or bruised appearance. 8 Within the first weeks of life, IHs undergo proliferation and become visible as an erythematous macule or slightly raised papular lesion that is soft and somewhat warmer than the surrounding skin but does not enlarge with Valsalva or in a dependent position. The lesions then undergo a classic progression of rapid proliferative growth followed by a slower and less consistent involution. The growth pattern of IH has been extensively studied and is comprised of six phases: (1) nascent, (2) early proliferative, (3) late proliferative, (4) plateau, (5) involution, and (6) abortive. Collaboration among international clinicians in the Hemangioma Investigator Group has allowed for prospective data collection in more than 1,000 children with IHs to further characterize the growth of these lesions. 9 The period of most rapid growth occurs in the early proliferative stage and is largely complete by about 5 months of age, with tumors reaching roughly 80% of their final size at this point. Despite the increase in size during proliferation, IHs tend not to expand beyond the defined anatomical site of the original lesion. The late proliferative phase is complete by 9 months in most children with very little growth occurring after this point as the lesion enters the plateau phase. Involution begins as early as 6 months and may last for several years. Clinically, lesions become lighter in color and softer to palpation with prominent lesions taking on a “deflated” appearance with somewhat spongy, redundant tissue. Nearly 60% of IHs will involute to aesthetically and functionally acceptable endpoints, but 40% of lesions leave a remnant that may require further treatment. 2 , 10 These lesions may appear as hypopigmented or telangiectatic macules, or fibrofatty residual tissue depending on the nature of the original tumor. The threshold for what is considered “acceptable” varies with location and size. For example, a small focal lesion of the nasal tip will have a very different impact than a larger, segmental lesion of the lower back.
IHs are subclassified by depth and morphology to provide a common language for clinicians and investigators to follow when characterizing these lesions ( Table 73.2 ). Superficial IHs are limited to the superficial dermis and have the classic bright red, slightly raised appearance, whereas deep IHs involve the deep dermis and subcutaneous layers without involvement of the overlying layers, giving the skin a slightly bluish hue or even a normal appearance. Mixed IHs involve both the superficial and deep layers. Deep IHs are the most likely to be clinically confused with vascular malformations because they lack the classic surface appearance attributed to IH, but evidence of rapid growth over time will identify these lesions as IH. For this reason, deep IHs tend to be recognized an average of 1 month later than superficial or mixed IH and their growth lasts 1 month longer. 9
Growth phase | Lesion depth | Lesion morphology |
Nascent | Superficial | Localized or focal |
Early proliferative | Deep | Segmental |
Late proliferative | Mixed | Indeterminate |
Plateau |
| Multifocal |
Involution |
|
|
Abortive |
|
|
IHs are classified morphologically into: (1) localized or focal when a solitary lesion exists, (2) multifocal when multiple lesions are present, (3) segmental when a lesion or cluster of lesions corresponds to a developmental subunit or dermatome, and (4) indeterminate for lesions that cannot otherwise be classified. Focal lesions are the most common, occurring in 80% of affected patients 2 ( Fig. 73.1 ). While IHs can occur throughout the body, they most commonly affect the skin of the head and neck (50 to 60%), followed by the trunk (25%) and limbs (15%). 10 Facial lesions are disproportionally distributed in the central face along lines of embryonic fusion with 60% of lesions occurring in the periorbital, nasal, and perioral zones, which collectively make up only 20% of the facial surface area. 8 The presence of more than five multifocal cutaneous lesions increases the chances of visceral organ involvement, particularly the liver, and further evaluation should be considered. 10 Segmental IHs are the least common subtype but are the most likely associated with other abnormalities, are more difficult to treat, and have worse outcomes. 7 These lesions are typically large, plaquelike tumors that loosely follow a dermatomal distribution of the trigeminal nerve in the head and neck. Segmental lesions have an even stronger predilection for involvement of the face than localized lesions, and they are more common in nonwhite Hispanic infants at older gestational age and higher weight than localized lesions, suggesting there may be differences in pathogenesis. 7 There is nearly twice the rate of female predominance among segmental IHs (5.7–6.6:1) compared to the localized form (3:1). 8 , 11 Facial segmental IHs can occur unilaterally or bilaterally and occupy zones supplied by one or more divisions of the trigeminal nerve, most commonly the third division (V3). These lesions of the so-called beard distribution have a unique association with IHs in the airway in 27 to 40% of lesions. 11 , 12 Most commonly, this involves the subglottis, but any level of the airway may be affected, and these lesions may lead to airway obstruction requiring systemic or surgical treatment including tracheostomy. Conversely, more than 50% of patients with IH of the airway have a concomitant cutaneous IH. 2 , 12 Segmental mandibular lesions also have an association with PHACE syndrome defined by the presence of a facial IH and one or more of the following: structural brain anomalies classically involving the posterior fossa, arterial anomalies, aortic coarctation or cardiac abnormalities, and eye anomalies. PHACE syndrome occurs in 20 to 33% of patients with segmental IH, and nearly 50% of patients with airway IH, but is much less common in infants with localized IH. 7 , 12

Complications of IH occur in up to 50% of infants, prompting the need for earlier intervention, and include functional impairment, ulceration, bleeding, infection, cardiac failure, and disfigurement. Complications are more likely based on size, location, and morphology of the lesions, but appear unrelated with patient characteristics or demographics. 13 Larger lesions are more likely to develop complications, particularly ulceration, with a 5% increase in complications for every 10 cm2 increase in size. Segmental lesions are 11 times more likely to develop complications and 8 times more likely to require treatment compared to local lesions, even when controlled for size. Higher rates of complications (1.7 times) are seen among IHs located on the face compared to other body sites, and facial IHs are three times more likely to require treatment 14 ( Fig. 73.2 ). Functional impairment most often interferes with visual axis, feeding ability, or respiration. Ulceration is the most common complication occurring in 5 to 15% of infants, with the highest rates seen for lesions involving mucous membranes or at areas of friction such as the lip and anogenital areas, whereas upper eyelid lesions are the least likely to ulcerate. 14 Mixed IHs are more prone to ulceration than superficial lesions, and up to 50% of segmental lesions undergo ulceration compared to 10 to 15% of localized lesions. 8 The cause of ulceration is unknown, but lesions are most likely to ulcerate during the proliferative growth phase, with some authors speculating this rapid expansion exceeds the elastic capacity of the skin and the lesions outgrow their blood supply leading to ulceration. As many as 13% of lesions, however, ulcerate during involution. 14 Ulcerated lesions may become secondarily infected, are at higher risk for bleeding (but this is rarely severe [2%]), and have a higher tendency to result in scarring or require treatment. 15

Pathogenesis and Histopathology
Histologically, IHs are characterized as a well-circumscribed, homogeneous mass of compact capillaries lined by plump endothelial cells with surrounding fibroblasts, pericytes, and mast cells. 10 During proliferation, high mitotic activity is seen among endothelial cells and pericytes as the tumor enlarges. Involution is accompanied by an increase in apoptosis as well as an elevated number of mast cells and cluster of differentiation 8+ T-cells. 16 Endothelial cells flatten with enlargement of their lumina and the lesions become dominated by fibrofatty stroma during involution and into the abortive phase.
The exact pathogenesis of IH is not known, but dysregulation of angiogenesis likely plays a central role. Premature infants are born during a time of theoretical imbalance favoring angiogenesis which may explain the increased incidence of IH in these infants. Additionally, alterations in several cytokines important in angiogenesis have been demonstrated during various growth phases of IH. The proliferation phase is dominated by vascular endothelial growth factor (VEGF), which is a primary mitogen for both benign and malignant vascular tumors and promotes cell survival while inhibiting apoptosis. 16 Serum levels of VEGF are elevated in infants with proliferating IH compared to involuting IH and controls. 17 VEGF activates angiogenesis via the mechanistic target of rapamycin signaling pathway, and recent work has demonstrated effectiveness for topical rapamycin in cutaneous IH. 18 Also elevated during this time are basic fibroblast growth factor, insulin-like growth factor 2, matrix metalloproteinase-9, and type IV collagenase while levels of endogenous interferon are decreased. 19 During involution, levels of VEGF, basic fibroblast growth factor, and insulin-like growth factor 2 decline, while levels of regulatory cytokines such as interferon and tissue inhibitor of matrix metalloproteinase 1 increase. 16
Endothelial cells in IH have a clonal origin, but the exact source of the original progenitor cell is not clear. Striking similarities have been found between IH and placental tissue, suggesting that progenitor cells from placenta may be associated with these tumors. 20 In addition to morphologic similarities between endothelial cells of IH and placenta, IH highly expresses glucose transporter 1 (GLUT-1), which is normally restricted to locations with blood–tissue barrier function like the placenta and brain. 21 The only vascular anomaly that expresses GLUT-1 is IH, making this an important marker to histologically confirm a diagnosis of IH and distinguish from other vascular lesions. Additionally, IHs uniquely express other placental markers such as Lewis Y antigen, merosin, and Fcγ receptor II, and have similar gene expression patterns to placental tissue. 20 , 22 Endothelial and mesenchymal progenitor cells have been identified in both IH and placenta, but the exact source of these progenitor cells is not clear. One theory suggests that fetal angioblasts differentiate into a placental vascular phenotype at locations predisposed to IH formation, while another posits that embolic cells from the placenta deposit in the developing fetus and differentiate into IH. 16 These embolic cells may be more likely to deposit in the head and neck due to the increased vascularity in this region with the most susceptible locations occurring at the end arteries of the developing facial placodes, which may account for the increased prevalence of IH at sites of embryologic fusion. 8 The fact that an increased incidence of IH is seen following chorionic villous sampling, placenta previa, and preeclampsia further supports the placental role in the pathogenesis of these lesions.
Diagnostic Workup
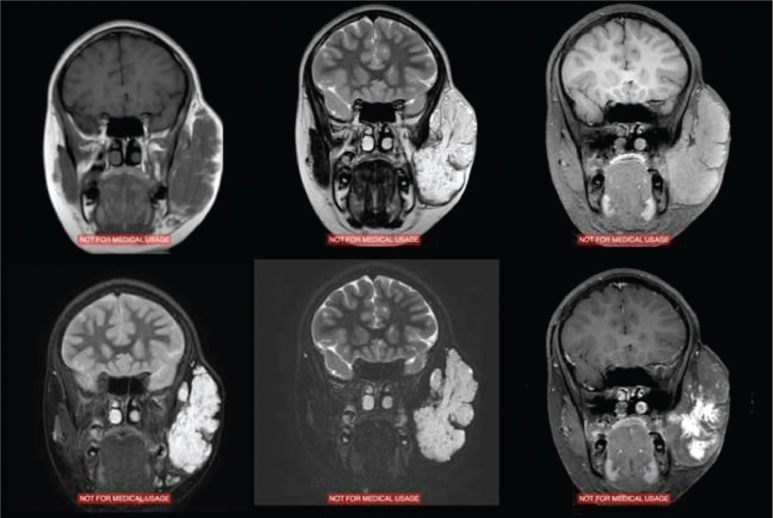
Most IHs are readily recognized by their characteristic clinical course and appearance, making further diagnostic testing rarely necessary. Imaging studies may be useful to evaluate for concomitant lesions, assess the full extent of a lesion that is not clinically visible, or occasionally lend support to an uncertain diagnosis. Ultrasonography can be helpful to examine for hepatic or abdominal IH in patients with multiple cutaneous lesions, or to evaluate the spine in patients with overlying lumbosacral lesions. Serial ultrasounds with and without color flow Doppler have been used to noninvasively monitor IH during growth or treatment when the lesion is not visible or has a significant deep component. However, clinical followup is more important than imaging. 23 Children with concern for PHACE syndrome should undergo imaging of the brain with magnetic resonance imaging (MRI) to evaluate for posterior fossa lesions, echocardiogram, and possibly angiography or magnetic resonance angiography to evaluate for aortic and cerebrovascular anomalies. When imaging is desired to determine the extent of the tumor, contrast-enhanced MRI is the modality of choice and provides excellent evaluation of soft tissue without exposing the patient to ionizing radiation. On MRI, proliferating IH appears as a distinct, lobulated, enhancing soft tissue mass that is isointense to muscle on T1 and hyperintense on T2 images, often with a visible feeding artery and draining veins and intralesional flow voids. 24 Involuting IHs are heterogeneous masses with areas of increased T1 intensity corresponding to fibrofatty tissue and less robust enhancement than proliferating lesions 25 ( Fig. 73.3 ). Again, imaging studies are rarely needed for diagnosis and treatment of uncomplicated IH.
Uncommonly, tissue biopsy may be necessary to confirm the suspected diagnosis or exclude other entities. IH can be positively identified based on characteristic histologic appearance and positive staining for GLUT-1, which is unique to IH among all other vascular anomalies. Laboratory blood tests play no role in the evaluation of patients with IH, as there is no associated coagulopathy with this condition. Some patients may have slightly elevated platelet counts and slightly decreased fibrinogen and D-dimer levels, but these still fall within the normal ranges. 26
Patients with IH and vascular anomalies should be evaluated and treated by a multidisciplinary team with knowledge of these lesions including pediatricians, ophthalmologists, radiologists, otolaryngologists, dermatologists, and facial plastic and reconstructive surgeons. Validated tools have been developed to objectively categorize the severity of IH and any associated complications, which may be helpful in stratifying patient severity, communicating with other treating clinicians, and tracking patient outcomes both clinically and in research studies. 27 , 28
Treatment
The management goal for IH is to achieve a functionally and aesthetically acceptable final result with the least amount of morbidity and lowest likelihood of complications. For some infants, this involves serial observation and reassurance during the phases of growth, while others require active treatment at various stages. At least 40% of IHs do not involute to an acceptable result and require additional treatment. Roughly half of IHs take more than 6 years to involute and 80% of these have aesthetically unacceptable results. 28 Since IHs are most common in the head and neck, the potential aesthetic consequences are quite high and nearly 50% of patients who require treatment cite disfigurement as the primary reason. 4 Treatment should be initiated prior to a child’s development of selfimage beginning at age 2.5 to 3 years, or before the social pressures of school at 5 to 6 years, to minimize the psychological effects of these lesions. Impending or active complications may mandate earlier treatment. Studies of children with IH suggest that those treated at young ages are not psychologically affected by the appearance of their tumors, despite significant distress felt by their family members over concerns for public scrutiny. 29 This argues for a paradigm shift away from the historic adage that IH should be managed with “benign neglect” because they would eventually “go away.” Since the eventual extent of involution is not predictable, intervention should be considered for any lesion whose treatment would result in an outcome as good or better than would be expected if the tumor was allowed to follow its natural history. The clinician should closely involve the family in the decisionmaking process at all stages so both parties can weigh the risks and benefits expected from treatment or continued observation.
Medical
A variety of medical treatments have been used through the years to treat IH with varying rates of success. In 2008, LéautéLabrèze and colleagues 30 serendipitously discovered the profound effects of propranolol on IH by observing dramatic improvement of a nasal IH in a child treated for obstructive hypertrophic myocardiopathy. Their initial report describes success in another 10 patients with a followup report the next year demonstrating stabilization in growth and acceleration of involution in 100% of 32 patients treated. 31 Until that time, the first-line treatment for IH was systemic corticosteroids with response rates on the order of 30 to 60% and over one-third of the patients in this report had previously failed steroid treatment. 31 Multiple additional reports followed demonstrating successful treatment of IH with propranolol at many cutaneous and visceral sites, 32 leading to widespread use of the medication with propranolol, which is evolving as the first-line medical treatment for proliferating IHs that require intervention. Despite the overwhelming positive clinical response of propranolol treatment, studies demonstrating efficacy have so far been limited to uncontrolled case studies.
Propranolol is a nonselective β-antagonist that inhibits β1 and β2 receptors with equal affinity and has known effects of decreasing heart rate and blood pressure. The exact mechanism of action is unknown for propranolol’s effect on IH, but several plausible theories have been put forth. 33 The early effects of propranolol occur within 1 to 3 days of initiating therapy and are manifested as softening and flattening of the lesions with decreases in redness. These effects most likely occur via vasoconstriction due to blockage of β2 receptors leaving α1 receptors unopposed. 33 Propranolol blocks the adrenergic stimulation of VEGF production and decreases expression of matrix metalloproteinase-9, which is thought to inhibit angiogenesis and slow proliferation. Finally, propranolol may speed involution through induction of apoptosis via the β2 receptors. Theoretically, β-agonists would have the opposite effect and possibly promote growth of IH, and some authors theorize that administration of tocolytics (β-agonists) to abort premature contractions may partially explain the increased rate of IH seen in babies born prematurely. 32
Propranolol is available as an oral suspension and is relatively well tolerated with no documented death or serious cardiovascular morbidity related directly to β-blocker use in children in over 40 years of clinical experience. 34 There are several wellknown side effects of propranolol that should be considered and discussed with parents including bradycardia, hypotension, bronchial constriction with exacerbation of underlying reactive airways, hypoglycemia especially among the premature or during times of limited oral intake or active infection, sleep disturbance, and gastrointestinal upset. Contraindications to propranolol therapy include preexisting bradycardia, hypotension, heart block or failure, asthma, or sensitivity to the drug. Protocols for pretreatment evaluation and drug initiation vary widely between clinicians with some pursuing a full cardiac workup and hospital admission to initiate therapy while others start the drug in an outpatient setting. Recently, a multispecialty consensus panel released guidelines on propranolol use in IH which are summarized herein. 35 Prior to initiating therapy, a targeted history and physical exam should be performed of the cardiovascular and pulmonary systems to assess for underlying heart failure, arrhythmia, or asthma. No definitive consensus could be reached on the need for a pretreatment electrocardiogram for all children, but it is recommended for children with baseline bradycardia, arrhythmia, or family history of congenital heart conditions or connective tissue disease in the mother. Routine echocardiogram in the absence of abnormal clinical findings is not indicated. Children with PHACE syndrome should be evaluated by a pediatric cardiologist prior to starting propranolol as there is an increased risk of ischemic stroke in these children with associated cerebrovascular abnormalities. Random glucose measurements have not been shown to predict hypoglycemia with propranolol therapy and are not indicated. The maximum effect of propranolol is seen 1 to 3 hours after a dose, so parents should be instructed to keep their child on a regular feeding regimen and avoid taking the medication during times of active infections to minimize the risk of hypoglycemia. The general dosing regimen used ranges from 1 to 3 mg/kg/day with most authors advocating for 2 mg/kg/day divided in three daily doses. This may be slowly escalated from a lower starting dose to minimize adverse effects, but these doses are below typical doses used in children for cardiovascular indications. The dose should be adjusted periodically to keep up with the child’s weight gain. Inpatient monitoring is suggested on initiation for infants ≤ 8 weeks old, or those with comorbid conditions affecting the cardiopulmonary system or increasing the risk of hypoglycemia. In older infants without these comorbidities and with good social support, initiation may be considered as an outpatient. These patients should have baseline vital signs including pulse and blood pressure and be observed in the office with repeat measurements at 1 and 2 hours after the first dose and every dose increase of > 0.5 mg/kg/day. The greatest response is seen within the first 8 weeks of therapy, and patients who demonstrate a 20% drop in heart rate within the first 2 weeks seem to have a more profound response than those whose heart rate is unchanged. 36 Treatment is generally continued through the proliferative phase and can be tapered off or discontinued after that point. Some lesions will demonstrate rebound growth and require resumption of the medication for a time. The goal is to treat with the drug beyond the time in the tumor’s natural history where it is proliferating.
Propranolol is most often started during the proliferative stage to limit IH growth and speed involution, but some authors have reported success with treatment initiated during the involution stage, likely related to the suspected effect on apoptosis. 37 Treatment started at this phase does not produce as dramatic results but does accelerate the rate of involution compared to the untreated state and may allow for more conservative surgical resections of residual deformities. Topical β-blockers have also demonstrated efficacy versus placebo for superficial lesions, 38 and atenolol (a selective β1 blocker) may have equal efficacy to propranolol with fewer side effects, but these results are still preliminary 39 ( Fig. 73.4 ).

Corticosteroids are an alternative medical therapy and represented the first-line option for treatment prior to the discovery of propranolol. They are effective only during the proliferative growth phase, but have been shown to stabilize growth or promote involution and are thought to act by decreasing VEGF-A expression through the NF-κB pathway. 40 A review of the literature revealed an average response rate of 84% of lesions when response was defined as stabilization of growth or involution, but rebound growth was seen in 36% of lesions and adverse effects occurred in 35%. 41 A dose response was seen with an average daily prednisone-equivalent dose among responders of 3 mg/kg compared to 2.1 mg/kg among nonresponders. 41 Adverse events are related to dose and duration of therapy and include irritability, behavior changes, Cushingoid appearance, altered appetite, increased susceptibility to infection, temporary growth retardation, hypertension, and hypothalamicpituitary-adrenal axis suppression. Therapy is typically started prior to 6 months of age for complicated IH, and response is often seen in the first 2 weeks of therapy. Once the lesion has stabilized, the steroids can be tapered, but rebound growth may necessitate prolonged therapy in up to one-third of infants. Most lesions require an average of 2 months of thearpy. 41 Intralesional steroid injections have been used with some success for isolated, deep, proliferating IH, especially in the periocular region, as an alternative to systemic therapy with decreased risk of side effects. 42 No direct, randomized, head-to-head comparison between corticosteroids and β-blockers has been carried out thus far, but there are two ongoing phase 2 trials (NCT01072045 and NCT00967226; ClinicalTrials.gov). A metaanalysis comparing individual studies, however, suggests superior efficacy with β-blocker treatment; 97% pooled response at 12 months compared to 69% for corticosteroid-treated lesions. 43 This clinical experience coupled with a more tolerable side effect profile has led to widespread use of propranolol as the first-line medical therapy for problematic IH.
Older therapies that demonstrated some efficacy in treating IH include interferon-α and vincristine. These were traditionally used for severe, life-threatening hemangiomas with moderate efficacy, but an unacceptably high rate of serious side effects occurred, including hematologic, hepatic, and neurotoxicity, such as spastic diplegia for interferon-α and neuropathy, hematologic toxicity, and inappropriate secretion of antidiuretic hormone for vincristine. 31 These are mentioned for historical purposes only and have no role in modern management of IH. Continued research, however, may identify promising targets for newer therapies such as rapamycin, a mechanistic target of rapamycin inhibitor, which has demonstrated efficacy for IH in culture and animal models. 18
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


