50 Tissue Expansion in Facial Reconstruction
Introduction
Large and complex defects of the face, head, and neck are challenging for the reconstructive surgeon. Traditional local and regional skin flaps should always be the first choice as they usually offer optimal aesthetic results with minimal morbidity. Occasionally, skin grafts may be employed but typically they offer distinctly inferior cosmetic results due to poor tissue match and have unique problems. Microvascular free tissue transfers, which can transfer large volumes of tissue reliably, are now routine for extensive and complex defects of the head and neck. Although free flaps are quite reliable, they come from distant areas in the body, and as such, the tissue match and ultimate aesthetic result is often poor. In addition, free flaps are often insensate and nonfunctional. When available local or regional tissue is inadequate, and if microvascular transfer is a poor option, then adjunctive techniques such as tissue expansion may be advantageous. Tissue expansion may allow a surgeon to develop enlarged local flaps, which have the advantage of possessing similar characteristics to the adjacent defect. Tissue expansion has also been used to enhance regional or microvascular flaps prior to transfer and to aid donor site repair. The decision to employ tissue expansion should be made carefully as complications from this technique are not unusual and the patient will be subjected to certain hardships during the tissue expansion process. This chapter summarizes the physiology, surgical techniques, applications, and complications of tissue expansion in the realm of reconstructive surgery of the head and neck.
History
Surgical tissue expansion at its most basic is simply an application of a natural physiologic process. The classic example of tissue expansion in nature is pregnancy where the uterus and abdominal tissues undergo dramatic and gradual expansion. Some cultures have employed primitive forms of tissue expansion for decoration, enhancement, and occasionally mutilation of facial and body structures such as the ear lobes and nostrils. Neumann 1 reported the first use of tissue expansion with a subcutaneous balloon in 1957, but it was not until the works of Austed 2 and Radovan 3 were published separately in the 1970s and 1980s that tissue expansion became a widely accepted technique. These authors’ works established the foundation for the basic understanding of the physiology of tissue expansion as well as the clinical applications of the techniques. In the following decades, numerous reports of clinical 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 and experimental 13 , 14 , 15 , 16 , 17 , 18 experience with tissue expansion have demonstrated the safety and efficacy of the techniques.
Tissue Responses to Expansion
Human tissues exhibit dynamic effects when exposed to sustained pressure and expansion. The histologic and biochemical changes that occur during tissue expansion have been studied extensively in both animal models and in humans. Different tissues respond variably to the forces of expansion, and the speed and duration of expansion have a significant impact on the tissue response. Not surprisingly, many tissues do not tolerate rapid or extreme expansion as well as controlled, gradual expansion.
A distinction must be made between the similarly named but physiologically distinct techniques of conventional, longterm tissue expansion and rapid intraoperative expansion (ITE). Sustained and progressive tissue expansion over the course of weeks and months results in significant physiologic and histologic changes in the skin and subcutaneous tissues. In contrast, ITE, which occurs over minutes, produces principally mechanical changes within the skin or it may represent an enhanced undermining and recruitment of surrounding tissues. 19 , 20 , 21 The differences between these techniques are discussed further in this chapter.
Long-Term Tissue Expansion
Extensive biologic and morphologic changes occur in tissues that are subjected to prolonged and progressive tissue expansion. Even though the surface area of the expanded skin is ever increasing during expansion, the overlying epidermis does not thin and has even been found to slightly thicken. 13 , 14 , 22 Studies have shown that the mitotic activity of the expanded skin is increased, 23 and this enhanced mitotic rate helps to maintain and enhance the epidermal height while the normal stratified epithelial appearance is preserved. These changes within the epidermis appear to be temporary and the microscopic appearance of the skin returns to normal within a year or two after the conclusion of the expansion. Clinically, the most common noticeable skin changes are increased dryness, erythema, and occasionally hyperpigmentation.
The dermis, meanwhile, does not tolerate chronic expansion as well. Typically, the dermis thins dramatically (30 to 50%), particularly when expansion is accelerated. 14 , 24 Increased metabolic activity has been observed in many of the cell populations that reside within the dermis. Fibroblast activity is increased and collagen synthesis is enhanced. Meanwhile, the physical arrangement of the collagen fibers is altered and elastic fibers become fragmented. Increased pigmentation may occur during expansion as a result of temporarily enhanced melanin production. Hair follicles become less dense due to the fact that the surface area of the epidermis increases while the actual number of hair follicles remains the same. The thickness of the basal layer has been seen to increase and additional myofibroblasts are found within the expanded tissues. This enhanced myofibroblast population is largely responsible for the contracture that may occur in expanded flaps after removal of the tissue expander and this should be kept in mind for surgical planning. The histologic changes seen within the dermis and associated appendages account for the common clinical characteristics of expanded tissues including stiffness, striae, erythroderma, alopecia, and diminished sensation. 25
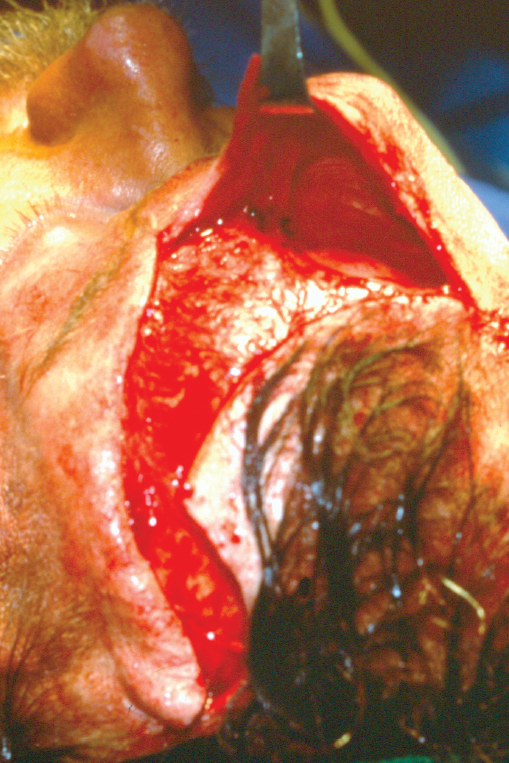
The expansion process also affects the structures located within the subcutaneous tissues. Adipose tissue is very intolerant of expansion and thins dramatically, losing up to 50% of its initial thickness. The fat cells become flattened, lose their fat content, and may be replaced with fibrous tissue. However, some of this loss of adipose volume may be regained after the expansion is completed. Vascular changes during expansion are quite dramatic as chronic tissue expansion is a strong stimulus for vascular proliferation. 26 This enhanced vascularity is one of the benefits of expansion as the enhanced blood supply of the tissue allows for the creation of vigorous, extensive local flaps, which are also more resistant to infection. 27 This can be particularly helpful in instances where the vascularity of the tissue is already compromised such as following radiation therapy, in smokers, and in patients with diabetes. During expansion there is a proliferation of capillaries and, ultimately, the venules and arterials, and lengthening of vascular structures occurs. 28 Clinical experience has shown that expanded flaps do have an enhanced survival rate similar to delayed flaps. 29 A dense fibrous capsule forms around the expander balloon, which contains high concentrations of fibroblasts but is also highly vascular ( Fig. 50.1 ). The capsule is lined with macrophages surrounded by fibroblasts that are actively producing collagen. The capsule may contribute to the enhanced vascularity of expanded flaps, but it also contributes to the contracture and shrinkage of the flap after the expander has been removed and the flap inset. This subsequent contracture may cause the flap to become thickened and aesthetically undesirable for certain reconstructions that require thin and pliable flaps as in the case of forehead flaps for nasal reconstruction 30 ( Fig. 50.2 ). If desired, this capsule may be excised cautiously, and in most instances this will not significantly compromise the vascularity of the flap. 31 A recent report describes a novel approach that actually utilized the expander capsule as a source for soft tissue graft and flap for correction of soft tissue deficiencies in scar revision cases, thereby turning a liability of the capsule into a benefit. 32

Muscular tissue does not tolerate expansion nearly as well as vascular tissue. Muscle thinning, necrosis, atrophy, and clinical weakness have all been observed. 33 In the face, this would be most concerning if expansion were to weaken the frontalis or other muscles of facial expression. Neural tissue is rather tolerant of expansion and gradual lengthening of nerves can be accomplished without necrosis. Experimental studies have shown that peripheral nerves can be lengthened up to 32% with longterm expansion but perhaps with some diminished function. 34 The facial nerve has been studied during rapid expansion by Martini et al, 35 who found the facial nerve of a cat to be significantly lengthened with intraoperative expansion. However, 40% of the expanded nerves failed to regenerate, likely due to mechanical axonal disruption or from compromised vascularity. Therefore, it is probably prudent to place expanders in the face and neck superficial to the facial nerve and superficial musculoaponeurotic system (SMAS) in the cheek or platysma in the neck to minimize potential injury to the facial nerve.
Rapid Intraoperative Expansion
Rapid ITE is a technique that has been championed by Sasaki as an extension of his experiences with conventional, longterm tissue expansion. 36 In practice, ITE involves a rapid, cyclical stretching of the skin performed during the same operative session in which one elevates and mobilizes tissue flaps. Initially, it was recognized that one could temporarily overinflate a longterm tissue expander balloon immediately prior to its removal, thereby gaining some apparent additional flap length. This concept was then applied on its own without any preceding chronic expansion. Sasaki has reported his experience with almost 300 cases in which he felt that an additional 1 to 3 cm of flap length is gained with this technique. The rapid nature of ITE obviously does not allow the physiologic or metabolic changes seen in longterm tissue expansion to occur. Rather, the increase in skin flap length is thought to arise principally from mechanical “creep” and maximization of the skin’s natural extensibility. Mechanical creep results from the combination of the displacement of interstitial fluid and ground substance, fragmentation of elastin, collagen fiber realignment, and adjacent tissue displacement into the expanded field. 24 Recent studies have also suggested that ITE may result in the induction of several genes that may be involved in cell growth regulation. 37 Rapid ITE remains a controversial technique and debate has largely centered on whether there are true expansion effects or whether ITE represents principally enhanced undermining, tissue recruitment, and redraping. 19 , 37 , 38 , 39 , 40 Recent reports in the literature, however, have continued to support ITE as a viable technique. 36 , 41 , 42 , 43
External Tissue Expansion
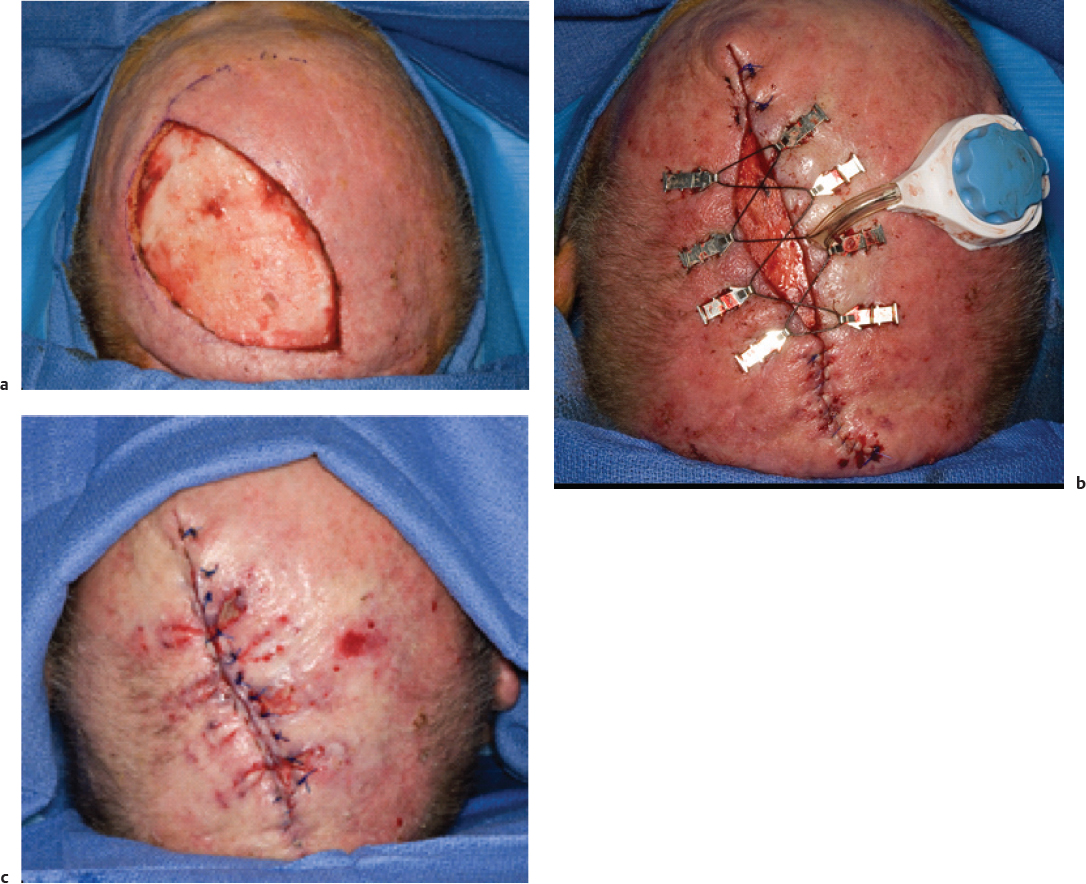
There have been recent reports of the use of external tissue expansion devices. These devices come in the form of adhesive and elastic tapes 44 , 45 or a mechanical tensioning device. 46 Both of these devices are applied for 1–14 days depending on the defect or surgical goal. As such, the principle benefit is derived from mechanical creep as described previously as there is not enough time for the physiological changes seen in prolonged expansion to occur. The external adhesive devices (DynaClose; Canica Design Inc.) have proven useful in the primary closure of forearm free flap donor sites when applied to the donor site 1 week prior to flap harvest. 44 , 45 The external tensioning device (Derma Close RC; Wound Care Technologies Inc.) has proven useful in the management of large scalp defects with reduction in wound size from 50 to 99% after 6 to 14 days of external expansion 46 ( Fig. 50.3 ). Further clinical studies will be needed to determine whether these devices may have other applications in facial reconstruction.
Indications for Tissue Expansion
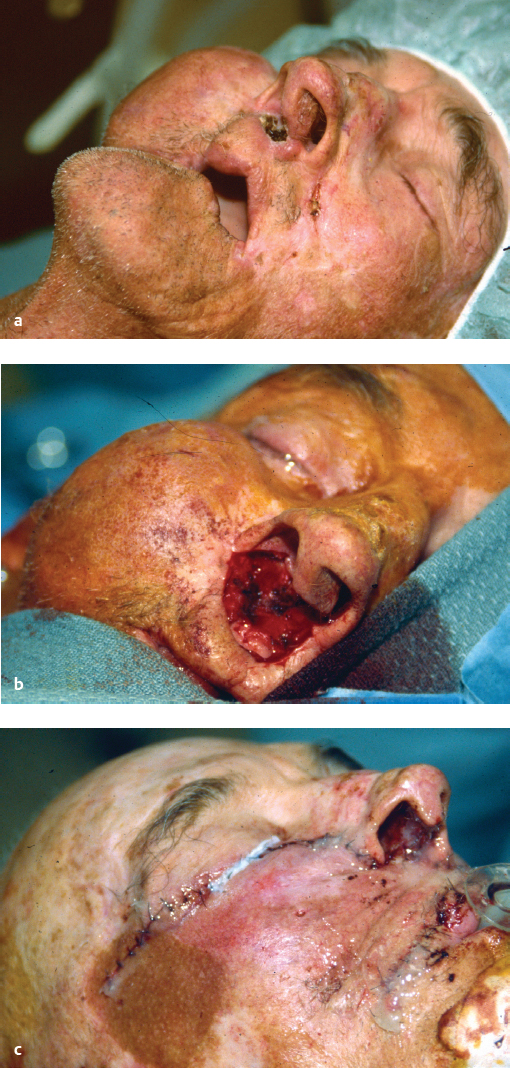
Tissue expansion is theoretically possible anywhere within the head and neck. Clinical experience, however, has shown that some areas are better suited to expansion because of thick overlying skin and a robust blood supply. Tissue expansion works best in locations where there is a solid bony support under the expander balloon device. For example, the scalp 47 , 48 and forehead 49 ( Fig. 50.4 ) are optimal locations for longterm expansion. Staged repair of extensive scalp defects ( Fig. 50.5 ) and hair replacement 50 , 51 , 52 are excellent opportunities to employ tissue expansion. Some surgeons have also advocated tissue expanders in auricular or microtia reconstruction. 53 , 54 , 55 , 56 However, as discussed previously with forehead flaps, the potential for contracture of an expanded flap as well as thickening of the tissue from the expander capsule may limit the application of expanded flaps used for ear and nose reconstruction. In these cases, a thin and pliable soft tissue coverage is essential to allow the underlying cartilaginous framework to show through. Expansion may also be used for large defects in the cheek secondary to skin cancer ( Fig. 50.6 ) or congenital lesions such as hairy nevi 57 , 58 , 59 ( Fig. 50.7 ). The surgeon should remember, however, that the cheek skin may not tolerate expansion well because the skin is relatively thin and there is potential for damage to the facial nerve and musculature. When an expander is employed in the cheek, it may be necessary to inflate the expander with smaller volumes of fluid over an extended period of time to minimize complications such as wound necrosis or expander exposure. Similarly, tissue expansion in the neck may be limited by the thin skin and underlying neurovascular structures. Tissue expansion may be particularly helpful in previously irradiated areas because of the enhancement of the vascularity, which is provided by the expansion. 60 However, one should be particularly cautious in these patients as their tissues will be more fragile and are potentially more prone to breakdown leading to exposure or extrusion of the expander (see Fig. 50.11 ). Romo and colleagues 61 have described a series of patients in whom a small tissue expander was placed intranasally to provide additional tissue for the successful repair of large septal perforations. Several reports have appeared in the literature describing the application of tissue expansion in regional or distant free flaps prior to their elevation and transfer to head and neck defects. 62 , 63 , 64 , 65 , 66 Preexpansion of flaps may lessen donor site morbidity as well as provide more tissue for transfer that has an enhanced blood supply. Whenever possible, the reconstructive surgeon should try to anticipate the size of the defect prior to its resection and plan the expansion accordingly. If one is faced with a large defect that will optimally be repaired with an expanded flap, consideration could be given to a temporary coverage with a skin graft while the expansion is underway. Once the expansion is completed, the skin graft can be excised and replaced with the expanded flap.



Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


