64 Craniofacial Approaches to the Anterior Skull Base
Introduction
Craniofacial surgical approaches developed by Obwegeser, Tessier, and many other pioneers are designed to address the anatomically complex junction between intracranial and extracranial compartments. The anterior cranial fossa lies in close proximity to both the orbit and the paranasal sinuses. Likewise, the middle cranial fossa is intimately related to the pterygomaxillary space, the infratemporal fossa, and the temporomandibular joint (TMJ). Surgical access to these regions is required for removal of a variety of benign and malignant neoplasms as well as for correction of traumatic or congenital anomalies. Traditional approaches to the anterior skull base have required transfacial incisions and removal of vital neurovascular and support structures, which have been associated with significant postoperative morbidity. Over the past four decades, craniofacial approaches have been refined with three goals in mind: (1) maximal exposure for direct access to the skull base, (2) preservation or anatomical reconstruction of vital structures, and (3) aesthetically acceptable incisions with avoidance of unnecessary facial scars. More recently, transnasal endoscopic approaches to the skull base have been pioneered to achieve these goals. These approaches have not supplanted open craniofacial approaches, and the open and endoscopic techniques can often be used together to optimize exposure and provide the best reconstruction.
Collaboration among surgical specialists in otolaryngology–head and neck surgery, facial plastic and reconstructive surgery, neurosurgery, and craniomaxillofacial surgery has led to the development of skull base surgical teams. Many of the approaches and fixation methods used today developed out of experience gained in treating patients with frontobasal trauma or congenital craniofacial anomalies. 1 , 2 Significant reductions in morbidity and mortality have been achieved with advances in reconstruction of skull base defects, which help prevent postoperative cerebrospinal fluid leak. Many reports have documented decreased incidence of complications associated with craniofacial approaches to the anterior skull base. 3 , 4 , 5
As in any surgical specialty, a thorough understanding of anatomy and physiology is crucial to the success of craniofacial surgery. This chapter will discuss some of the pertinent anatomy for craniofacial approaches. However, a detailed discussion of the complex anatomy of the skull base is beyond the scope of this chapter. 6 The purpose of this chapter is to outline surgical approaches to the anterior skull base, infratemporal fossa, pterygomaxillary space, and orbit. These approaches are used in the treatment of patients with tumors, trauma, or congenital anomalies.
Subcranial Approach to the Anterior Skull Base
Traditional craniofacial resection of anterior skull base lesions requires frontal craniotomy to provide access to the skull base superiorly, along with transfacial incisions to approach the skull base inferiorly. This combined superior and inferior approach allows for improved control of tumor margins. The limits of transfacial approaches, however, include the frequent need for frontal lobe retraction, anosmia, and the potential for obvious facial scar formation. The subcranial approach, also referred to as the transglabellar or subfrontal approach, was initially described by Raveh et al for treatment of skull base trauma. 7 By disarticulating the frontonasoorbital complex, access is gained to the nasal cavity, paranasal sinuses, medial and superior orbit, and floor of the anterior cranial fossa without the need for transfacial incisions or frontal lobe retraction. The utility of this approach in management of skull base tumors lies in the broad anterior and inferior exposure of the skull base. This broad exposure allows precise control of tumor margins and reconstruction of the skull base defect.
Incisions and Soft Tissue Anatomy
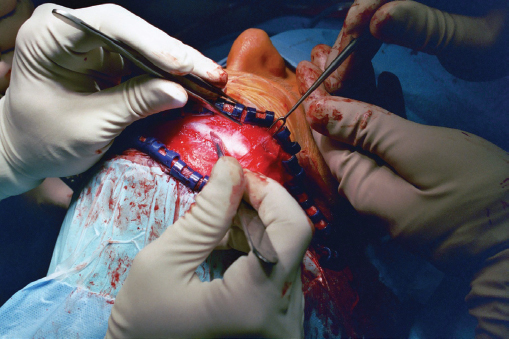
Appropriate prophylactic antibiotics for clean contaminated neurosurgical procedures should be administered at induction and as required throughout the operation. The head should be prepped as usual for craniotomy. The hair should be parted and banded in sections, or a small strip of hair should be shaved around the incision. The subcranial approach is begun by completing a bicoronal incision that extends from the preauricular crease anterior to the tragus, up to the root of the helix, then superiorly over the vertex to the root of the helix and preauricular crease on the contralateral side. 8 The incision should be 3 to 4 cm posterior to the hairline with care taken to avoid the receding temporal hair line in men. The incision is carried down through skin, subcutaneous tissue, and the occipitofrontalis/galeal layer to the level of the subgaleal loose areolar tissue ( Fig. 64.1 ). The coronal flap is then sharply elevated in a subgaleal fashion being careful to leave the pericranium as thick as possible with loose areolar tissue. Elevation proceeds in this manner to within 2 cm of the superior orbital rims.
As dissection proceeds laterally over the temporal region, the surgeon must be careful to protect the frontal branch of the facial nerve as well as the superficial temporal artery and vein, which may be necessary for vascular supply of regional or free tissue reconstruction. The fascial layers overlying the temporalis muscle have been given many names making communication concerning these layers difficult. The temporoparietal fascia is the superior extension of the superficial musculoaponeurotic system of the midface. The temporoparietal fascia is continuous with the occipitofrontalis/galeal layer superiorly. The superficial temporal artery and vein lie within the temporoparietal fascia. The frontal branch of the facial nerve is adherent to the undersurface of the temporoparietal fascia as it crosses over the zygomatic arch.
The deep temporal fascia is continuous with the pericranium superiorly above the temporal line. Below the temporal line, overlying the temporalis muscle, the deep temporal fascia is thick. Further inferiorly, at about the level of the superior orbital rim, the deep temporal fascia splits to form the superficial layer of the deep temporal fascia and the deep layer of the deep temporal fascia. The superficial layer of the deep temporal fascia continues inferiorly to fuse with the anterior periosteum over the zygomatic arch. The deep layer of the deep temporal fascia continues inferiorly to fuse with the medial surface of the zygomatic arch. Between the two layers of the deep temporal fascia is a small fat pad called the superficial temporal fat pad.
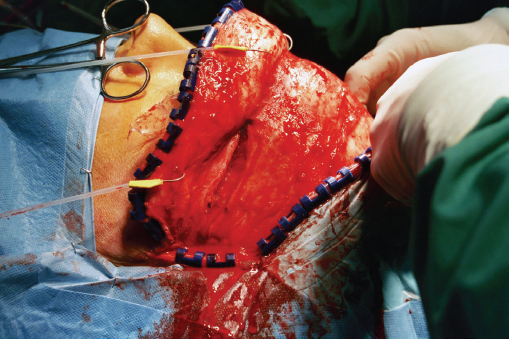
As the coronal flap is elevated inferiorly toward the zygomatic arch, the dissection should be deep to the temporoparietal fascia and superficial to the deep temporal fascia. This is continuous with the subgaleal dissection medially and attention is paid to proceeding on a wide surgical front to maximize exposure. Once the flap is elevated to within 2 cm of the zygoma, a horizontal incision from the lateral orbital rim to the root of the helix should be made through the superficial layer of the deep temporal fascia ( Fig. 64.2 ). Dissecting below this layer to the zygoma will help protect the frontal branch of the facial nerve. The zygoma can then be dissected in a subperiosteal plane from lateral to medial where the dissection can be connected to the subperiosteal plane along the lateral orbital rim.
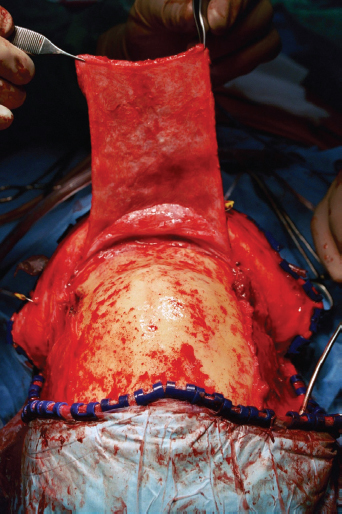
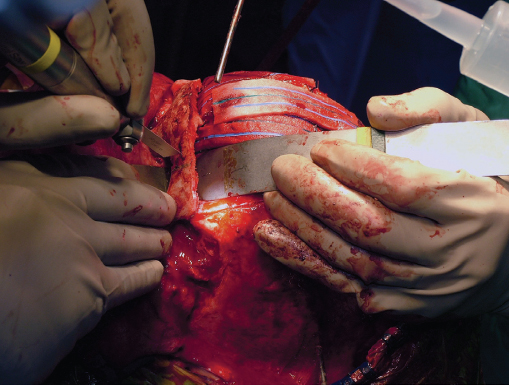
Attention is then turned to elevation of the pericranial flap. Typically, the pericranial flap is bipedicled based on the supraorbital arteries and extends 15 cm cephalic to the supraorbital rims. The flap can be designed to extend posterior from the temporal line on each side to the vertex of the skull ( Fig. 64.3 ). After incising the periosteum with either the knife or electrocautery, the pericranial flap is carefully elevated using a wide periosteal elevator. As the pericranium is elevated up to the superior orbital rims, the supraorbital neurovascular bundles must be identified and protected. In the majority of patients, these will lie within a supraorbital notch found along the medial aspect of the supraorbital rim. In a minority of patients, the supraorbital neurovascular bundle will lie within a true foramen ( Fig. 64.4 ). If this is the case, a small osteotome can be used to notch out the foramen allowing anterior displacement of the neurovascular bundle ( Fig. 64.5 ).
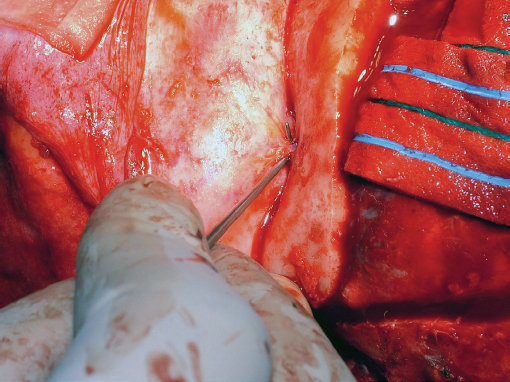

To facilitate maximum exposure, the periorbita is dissected free from the orbital roof posteriorly 3 to 4 cm. This is done safely knowing that the orbital depth from the rim to the optic strut is 45 to 55 mm. Care is taken not to disrupt the periorbita, as this will expose orbital fat and make visualization more difficult. In addition, in instances of periorbita disruption, the trochlea may be less likely to reattach independently during postoperative healing. 9 Also, the superior branch of the oculomotor nerve (cranial nerve III) can be injured with disruption of the periorbita and cause postoperative levator dysfunction. Medially, the subperiosteal dissection continues down the medial orbital wall. The frontoethmoid suture marks the level of the cribriform plate and transmits the anterior and posterior ethmoid arteries through their respective foramen. The anterior ethmoid artery is found roughly 24 mm from the anterior lacrimal crest. The posterior ethmoid artery is 12 mm behind the anterior ethmoid artery. The optic nerve is then another 6 mm behind the posterior ethmoid artery. The anterior ethmoid artery is ligated using either bipolar electrocautery or small clips. Centrally, the periosteum and soft tissue over the glabella and nasal dorsum are elevated all the way down to the bony cartilaginous junction. With the soft tissue elevation now complete, attention is turned to the bony anatomy.
Osteotomies and Bony Anatomy
Intracranial exposure begins with a wide bifrontal craniotomy performed by the neurosurgical service. Typically, the craniotomy is designed to extend from temporal line to temporal line just superior to the aerated frontal sinus. The bone cuts then gently curve posteromedially to meet in the midline ∼10 cm cephalic to the glabella. The frontal bone flap is then turned with careful attention to preservation of dura and the superior sagittal sinus.
The dura of the anterior cranial fossa is then carefully elevated beginning anterosuperiorly with elevation off the frontal bone making up the posterior wall of the frontal sinus. Anterolaterally the dura is elevated off the frontal bone making up the superior orbital rim and orbital roof bilaterally. Centrally, dissection is carried posterior to the level of the foramen cecum, just anterior to the crista galli and the cribriform plate.
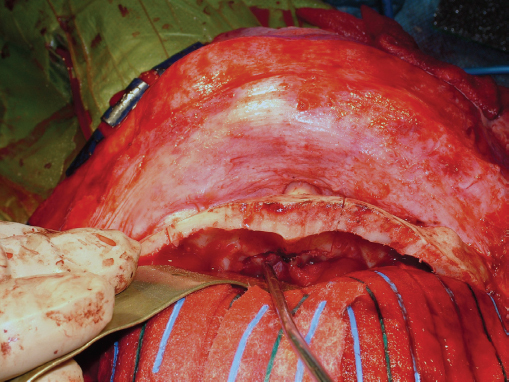
Depending on the location of the lesion, osteotomies are then planned for removal of the frontonasoorbital complex. The frontal lobes and orbital contents are protected with malleable retractors. Using an oscillating saw, sagittal cuts are made through the superior orbital rim and orbital roof to a depth of ∼2 cm bilaterally ( Fig. 64.6 ). Cuts are made outside of the frontal sinus in order to prevent delayed mucocele formation. Using a sidecutting bur, cuts are then extended medially along the orbital roof and extended to meet in the midline at the foramen cecum ( Fig. 64.7 ).
The roof of the orbit meets the medial orbital wall at the frontoethmoid suture. Inferior to the frontoethmoid suture, the lamina papyracea of the ethmoid bone constitutes the medial orbital wall. Anteriorly, the lacrimal bone constitutes a small portion of the medial orbital wall and is seen as the posterior lacrimal crest lying posterior to the lacrimal fossa. Anterior to the lacrimal fossa is the frontal process of the maxilla, and it is seen as the anterior lacrimal crest. This bony prominence marks the insertion of the medial canthal tendon. Using the sidecutting bur, an osteotomy is brought forward from the medial extent of the orbital roof osteotomy along the medial orbital wall to extend anterior to the anterior lacrimal crest and thus avoid disrupting the insertion of the medial canthal tendon ( Fig. 64.8 ).
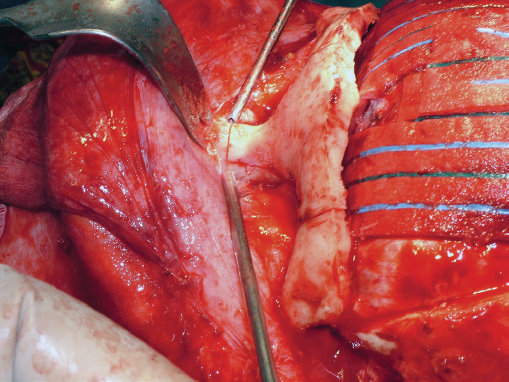
Anterior to the frontal process of the maxilla lie the paired nasal bones with the upper lateral cartilages of the nose attached to their caudal ends. Continuing with the sidecutting bur, the osteotomy is continued caudally along the lateral aspect of the nasal bones to within 2 to 3 mm of the bony cartilaginous junction. Here, a transverse osteotomy is performed using a thin oscillating saw ( Fig. 64.8 ).
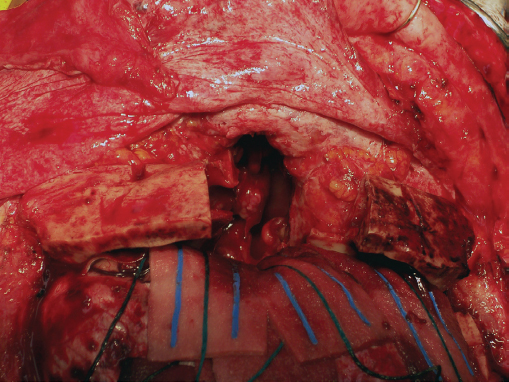
Finally, the frontonasoorbital complex is disarticulated from the bony nasal septum using a sharply curved osteotome placed directly through the previously cut bone at the level of the foramen cecum. With removal of the frontonasoorbital complex, the nasal vault, ethmoid sinus, and medial and superior orbit are easily visualized ( Fig. 64.9 ). The floor of the anterior fossa is composed of the ethmoid bone making up the cribriform plate. Depending on the site of the lesion, the olfactory apparatus can be sectioned off of the cribriform plate either unilaterally or bilaterally. If done unilaterally, olfaction can possibly be preserved on the contralateral side.
Posterior to the cribriform plate is the planum sphenoidale of the sphenoid bone, which extends further posteriorly terminating at the anterior clinoid processes. From here the optic nerves can be appreciated as well as the optic chiasm. If needed, the sphenoid sinus can be opened allowing direct visualization of the internal carotid arteries in the lateral wall of the sphenoid.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


