65 Mandible Fractures
Introduction
Mandible fractures occur both as isolated injuries and in conjunction with maxillofacial fractures or multisystem trauma. Patients presenting with mandible fractures require initial evaluation by the emergency department physician and in some cases activation of the trauma team following current Advanced Trauma Life Support protocols. 1 The identification of a fractured mandible during the initial emergency department workup should lead to a request for a facial trauma consultation. Fine cut (1 mm or less) computed tomography (CT) scanning is the current standard for confirming or identifying fractures. Panoramic tomography (e.g., Panorex [Panoramic Corporation]) is also useful but is less sensitive than CT, 2 , 3 especially in the region of the symphysis. The most common fracture site in the mandible is controversial and largely dependent on mechanism of injury. Assault victims will often have angle fractures resulting from a lateral blow. Falls are associated with a higher incidence of condylar and subcondylar fractures. 4 , 5 The mandible’s anatomical architecture as a ring of bone increases the likelihood of multiple fractures. Fractures of the mandibular angle and the contralateral body or parasymphysis are the most common combination. 6 It is crucial to maintain a high level of suspicion for multiple fractures to develop an effective treatment plan. The surgeon’s prompt evaluation of mandible fractures is indicated once life-threatening injuries have been addressed and the patient is stabilized. Establishing baseline occlusion prior to rigid fixation is paramount for successful repair. Most displaced fractures are treated with maxillomandibular fixation and/or open reduction and internal fixation (ORIF) via transcutaneous and transoral approaches. Surgical intervention should restore preinjury occlusion and appearance.
Anatomy
Skeletal Anatomy and Dentition
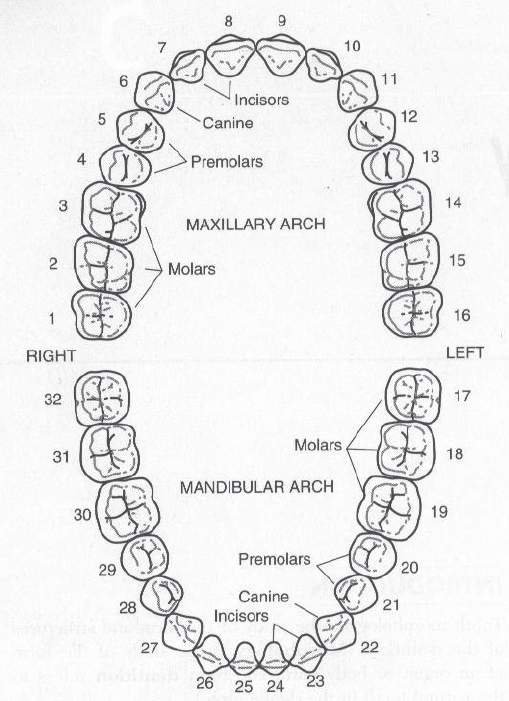
The mandible is the only mobile bone in the facial skeleton and is essential for mastication. During development, the two hemimandibles fuse at a vertical midline symphysis by age 2, creating a single bony arch. The adult mandible consists of a cortex 2 to 4 mm thick that surrounds medullary bone. The alveolar processes of the horizontal body house the lower dentition including two central incisors, two lateral incisors, two first premolars, two second premolars, and three sets of molars. Fig. 65.1 demonstrates standard numbering of the adult maxillary and mandibular dentition.
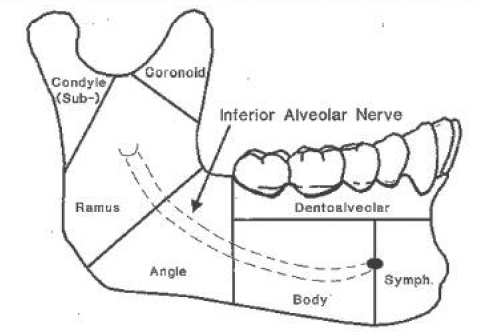
The anatomical subunits of the adult mandible as used for fracture classification are shown in Fig. 65.2 . Anteriorly, the symphysis joins the two mandibular bodies. Each horizontal mandibular body transitions laterally to a vertical ramus through the angle region. Proximally the ramus terminates at coronoid and condylar processes separated by the sigmoid notch. The coronoid process extends anteriorly and is deep to the zygomatic arch. The condylar process is positioned posteriorly and articulates with the mandibular fossa of the temporal bone, forming the temporomandibular joint.
Inferior Alveolar Nerve
The inferior alveolar nerve innervates the mandibular teeth and is a branch of the mandibular nerve (V3). Entering the mandibular foramen on the lingual surface of the ramus, it courses within the inferior alveolar canal. This canal initially runs inferiorly and anteriorly, passing in close proximity to the root of the third molar. The nerve and canal then continue anteriorly just inferior to the level of the mental foramen where the inferior alveolar nerve will ascend and exit the mandible, becoming the mental nerve. The mental foramen is located on the buccal surface of the horizontal mandibular body usually at or slightly anterior to the second premolar. After exiting the mental foramen, the mental nerve divides under the depressor anguli oris into three main branches innervating the chin, lower lip, and gingiva. 7
Muscle Attachments
Several muscle attachments on the mandible are relevant to fracture physiology and repair. Lateral surface attachments include the mentalis and masseter. The mentalis muscle originates anteriorly at the incisive fossa just lateral to the symphysis and located below the incisors. The mentalis inserts on the skin of the chin. The masseter muscles originate from the inferior medial border of the zygoma and insert along the lateral surface of the mandibular ramus and coronoid process. Medial surface attachments include the temporalis, medial pterygoid, and lateral pterygoid muscles. The temporalis originates in the temporal fossa and inserts on the medial surface of the coronoid process. Medial and lateral pterygoid muscles originate from the medial and lateral surfaces of the lateral pterygoid plate, respectively. The lateral pterygoid inserts on the condyle; the medial pterygoid inserts on the medial surface of the ramus inferior to the mandibular foramen. 8
Demographics and Etiology
Mandible fractures most often result from interpersonal violence and motor vehicle accidents. Falls, athletic injuries, work-related injuries, neoplasms, and iatrogenic injury are other causes. 9 Though mandible fractures occur at any age, they most often present in males during their third decade of life. 9
The most common fracture site in the mandible is controversial and largely dependent on mechanism of injury. Assault victims will often have angle fractures resulting from a lateral blow. Falls and auto accidents result in more condylar, body, and subcondylar fractures. 4 , 5 , 9 Multiple fractures are present in the majority of cases, but single fracture sites also occur. 9 The mandible’s anatomical architecture as a ring of bone increases the likelihood of multiple fractures, and fractures involving the mandibular angle and the contralateral body or parasymphysis are the most common combination. 6
Most mandible fractures are technically classified as open fractures, occurring between teeth and resulting in a gingival tear. Less than 1% of fractures occur in edentulous patients, and most involve the mandibular body. 10
Evaluation
All trauma patients should initially be stabilized and evaluated according to Advanced Trauma Life Support protocol by an emergency department physician or the trauma team. 1 Mandible fractures are likely in patients with the following signs and symptoms: jaw pain and/or swelling, limited jaw movement, gingival bleeding or hematoma, displaced teeth, and absent or altered sensation to the teeth and lower lip. When suspected, a fine cut (1 mm or less) maxillofacial CT including the entire mandible has become the gold standard to screen for and identify mandible fractures. Panoramic tomography (e.g., Panorex) is also useful but is less sensitive than CT. 2 , 3 Identification of fractures on a CT scan or radiograph is often the impetus for consulting the facial trauma surgeon. Full assessment of a mandible fracture requires that the facial trauma surgeon carefully examine axial, coronal, and sagittal cuts of the affected area. High-definition threedimensional reconstructions of the mandible have also become increasingly available at many institutions. The authors find threedimensional images extremely useful in understanding fracture fragment orientation and formulating a treatment plan; however, the surgeon must be aware that subtle fractures may not be visible on these images due to volume averaging.
Availability of high-quality CT scans should not preclude the facial trauma specialist from obtaining a detailed history and performing a thorough physical examination. The historian should inquire about mechanism of injury, baseline versus current occlusion, lip sensation, prior injuries, prior surgery, and other medical problems.
The physical exam begins with assessment of the cranial nerve function with particular focus on lower lip sensation. Anesthesia or dysesthesia in the distribution of the mental nerve is common with body and angle fractures on the affected side. It is imperative that any neural deficits be documented preoperatively. The mandible is palpated carefully to identify sites of tenderness, stepoffs, and fracture mobility. 11 Exam findings must be consistent with fracture sites seen on imaging. A lack of clinical findings for a radiographic fracture line may suggest an old fracture; such fractures may be stable and require no intervention. Evaluation of maximal mouth opening is essential. Limitations are usually secondary to muscle spasm and pain. In these patients, jaw range of motion often normalizes with administration of anesthetic agents. In the rare patient, however, a physical (i.e., bony) limitation is possible that may preclude transoral access for airway management. For this reason, surgical planning should include a discussion of the patient’s mouth opening with the anesthesiologist. Instability or pain in the maxilla with manipulation suggests concurrent midfacial fractures that complicate treatment and restoration of occlusion. Additionally, nasotracheal intubation may not be feasible in patients with extensive midface fractures necessitating tracheotomy placement.
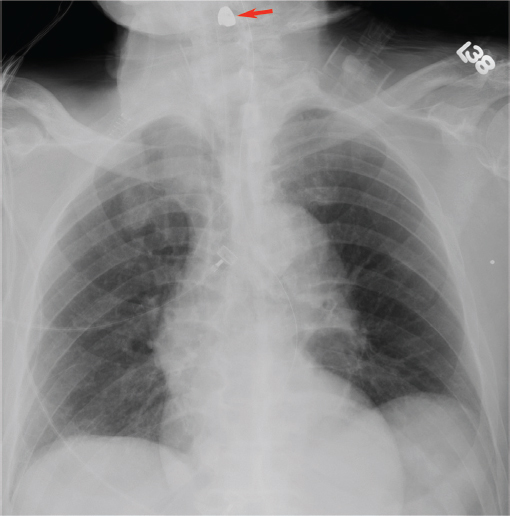
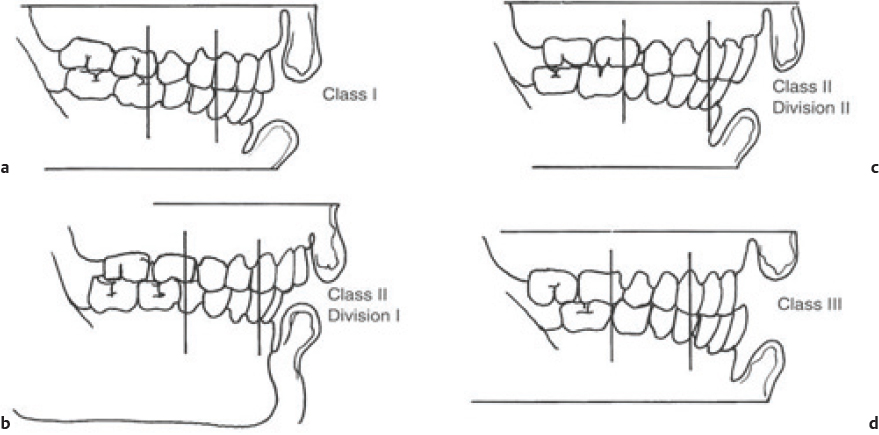
Preoperative occlusal evaluation should be performed by having the patient bite down into his or her best fit occlusion. Careful examination of the dentition will identify loose or avulsed teeth. If teeth are missing, chest imaging should be performed to ensure that they have not become airway foreign bodies ( Fig. 65.3 ). Fig. 65.4 demonstrates variants of adult occlusion. Ideal occlusion or Angle’s Class I occlusion occurs when the mesialbuccal cusp of the maxillary first molar rests in the buccal groove of the mandibular first molar ( Fig. 65.4a). Class II occlusion occurs when the mesialbuccal cusp rests anterior to the buccal groove. There are two divisions of Class II occlusion. In the first division ( Fig. 65.4b ), the incisors demonstrate an overjet. In the second division, the incisors are palatally tilted to compensate for the abnormal occlusion; this results in a more normal appearing dental relationship anteriorly ( Fig. 65.4c ). Class III occlusion occurs when the mesialbuccal cusp rests posterior to the buccal groove ( Fig. 65.4d ). 12 Wear facets on the teeth may offer hints to the preinjury occlusion in patients with poor dentition or longstanding malocclusion. An anterior open bite suggests possible subcondylar fracture(s). Grasping and attempting to manipulate the fractured mandible segment may assist in assessing instability of the fractured segment. Bilateral fractures may result in an unstable central mandible fragment that when posteriorly displaced results in tongue prolapse and airway obstruction. Anterior traction on the tongue with a heavy suture or towel clamp can restore and maintain the airway acutely while deciding on more definitive airway management such as intubation or tracheotomy. 13
Indications for Surgical Management
Minimally displaced or nondisplaced mandible fractures that are not causing excessive pain and do not affect occlusion may be treated with watchful waiting and soft diet for 6 weeks. However, these cases are in the minority, and most mandible fractures require intervention to control pain and to maximize the patient’s chances of returning to preinjury appearance and functional status. Modern approaches are safe and aesthetically acceptable when performed properly. Most mandible fractures do not require immediate intervention and can be repaired within a few days of the injury. More urgency is required for highly unstable fractures, airway compromise, or patients with intolerable pain. When appropriate, delaying repair for 48 to 72 hours may allow swelling to decrease and facilitate improved surgical exposure. Delayed repair also allows adequate time for the cervical spine to be cleared of injuries as indicated prior to proceeding with mandible repair. The freedom to flex, extend, and turn the head is useful when attempting to reduce and repair displaced fractures in the angle, ramus, and subcondylar regions.
Condylar and Subcondylar Fractures
Intracapsular fractures of the condylar head are typically treated in a closed fashion that includes physical therapy to minimize the risk of postoperative temporomandibular joint complications. This will restore normal function in the majority of cases. Late complications including temporomandibular joint pain and dysfunction are possible.
The treatment of subcondylar fractures, occurring between the ramus and condylar head, is more controversial. Closed treatment with mandibulomaxillary fixation (MMF) to reestablish occlusion has historically been acceptable for most subcondylar fractures. Closed treatment will usually restore acceptable function for unilateral non- or minimally displaced fractures. 14 Even displaced unilateral fractures in patients with good posterior dentition can be treated closed with good functional outcomes because the teeth assist in maintaining appropriate vertical height. 15 However, these patients may have to accept permanent deviation of the mandible toward the side of the fracture during mouth opening and mandibular protrusion due to altered biomechanics. 15 ORIF theoretically offers the advantages of superior anatomical reduction, function, and facial symmetry. The following are considered absolute indications for ORIF for treatment of subcondylar fractures:
Inability to achieve adequate occlusion 16
Dislocation into middle cranial fossa or external auditory canal 16
Open fracture with gross contamination 16
Associated comminuted maxillary fractures 15
Relative indications for ORIF include:
Displaced fractures
Bilateral fractures
Edentulous, atrophic mandible
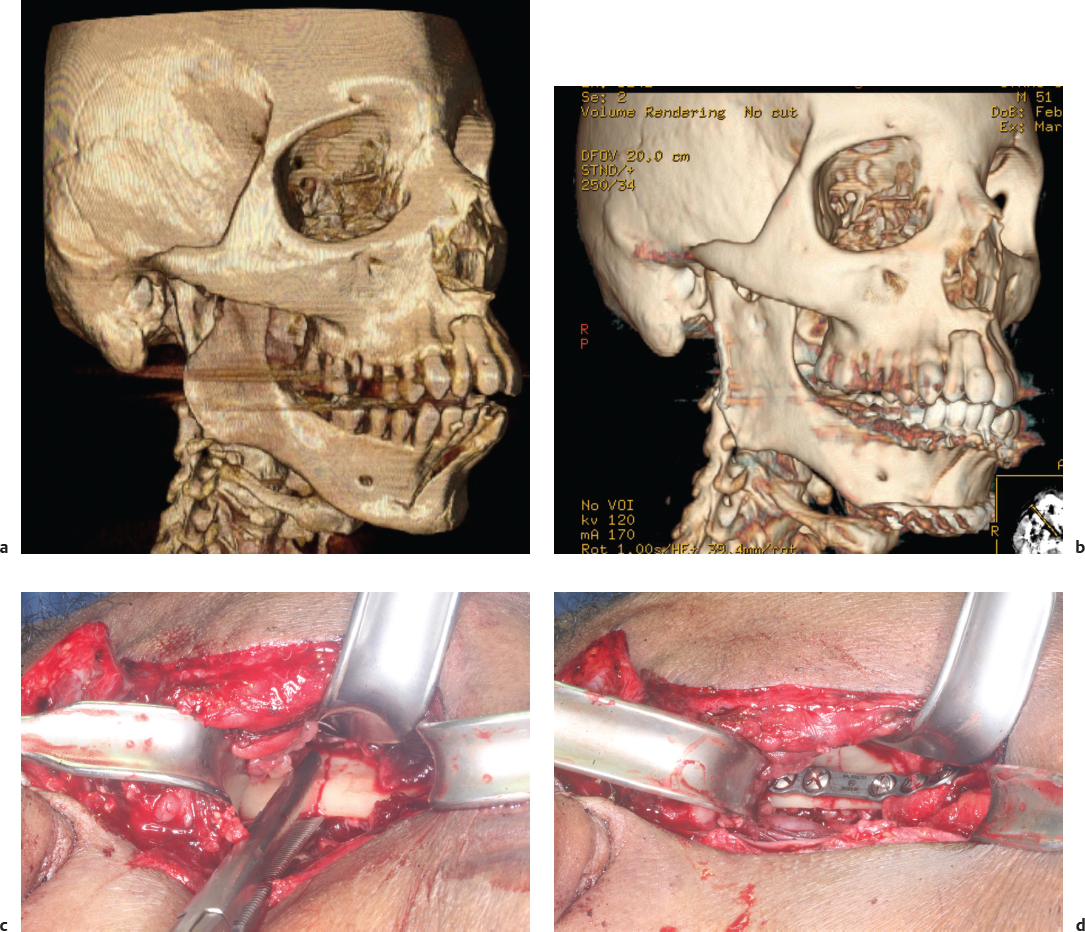
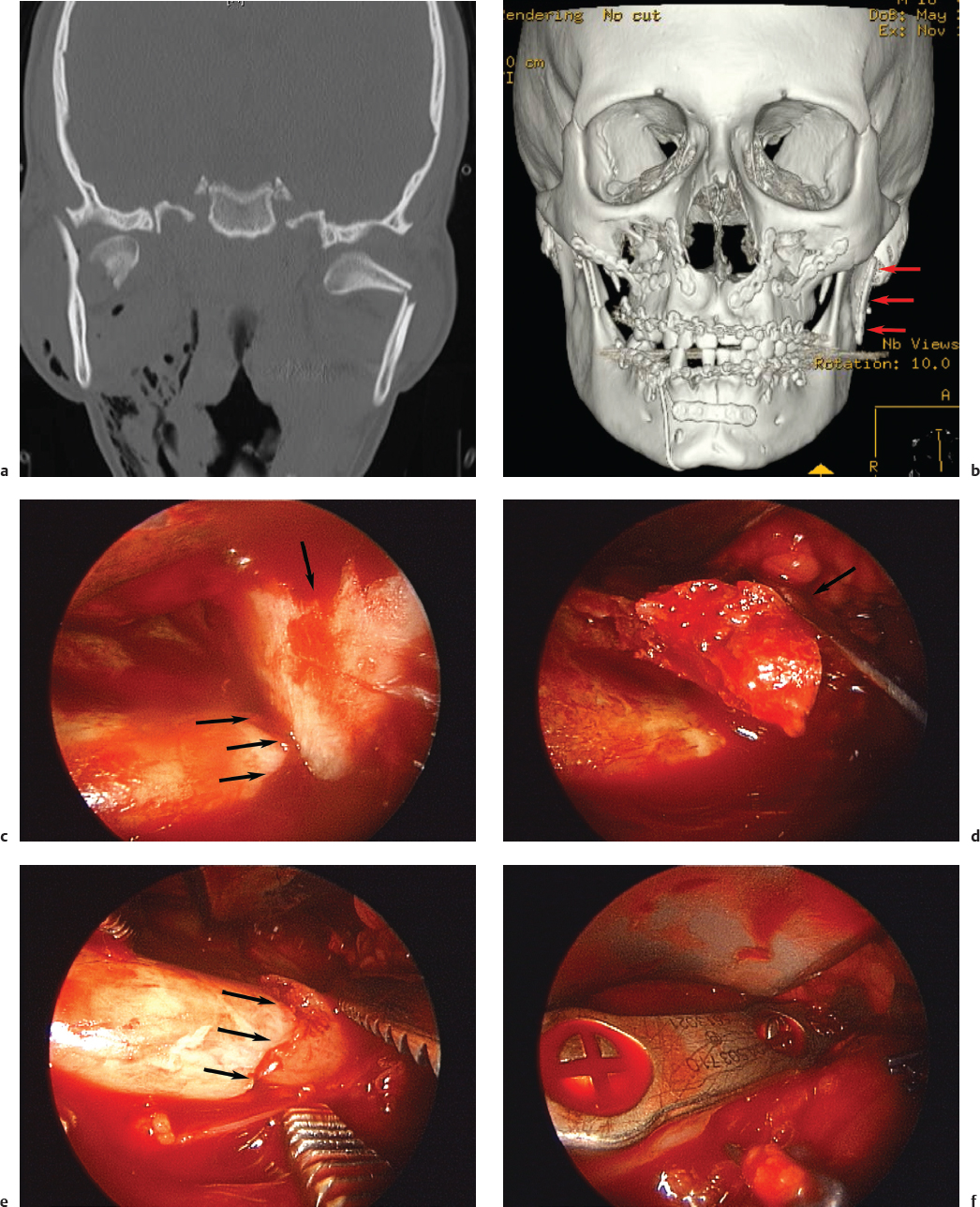
ORIF may prevent vertical height loss, facial asymmetry, malocclusion, deviation on mouth opening, and chronic temporomandibular joint pain in select patients; however, the surgeon must weigh the merits of ORIF against increased risks of facial nerve injury and visible facial scarring ( Fig. 65.5 ). 17 Endoscopic repair of subcondylar fractures is an alternative to traditional open approaches for surgeons trained in this technique. Endoscopy eliminates the need for a significant external incision and decreases the risk of facial nerve injury while still allowing for open reduction and plating of the fracture ( Fig. 65.6 ). Unfortunately, the equipment and surgical expertise required to effectively execute endoscopic repairs are not always available. 15
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


