72 Velopharyngeal Dysfunction
Introduction
The velopharynx serves as a muscular valve between the nasopharynx and oropharynx. Normal velopharyngeal function contributes to swallowing and speech production. Velopharyngeal dysfunction encompasses a constellation of disorders in which velopharyngeal closure does not occur appropriately during swallowing or the production of oral speech. Within the spectrum of velopharyngeal dysfunction, commonly used terminology includes velopharyngeal insufficiency, velopharyngeal incompetence, and velopharyngeal mislearning. 1 , 2 Velopharyngeal insufficiency has been used to describe an anatomical or structural defect that prevents adequate velopharyngeal closure, as is often the case with patients with cleft palate. In contrast to a contributory structural anomaly, neurologic dysfunction is thought to be the basis for velopharyngeal incompetence. Neurologic dysfunction can be the result of central nervous system impairment as with stroke, or the consequence of processes such as skull base tumors with compromise of peripheral nerve function. Velopharyngeal mislearning refers to an articulation disorder in which aberrant or compensatory speech production is present, and may either occur in isolation or secondary to velopharyngeal insufficiency. 2 , 3 The significance of these distinctions is that while velopharyngeal mislearning is managed with speech therapy, velopharyngeal insufficiency often requires surgical intervention to address anatomical abnormalities. Some patients, such as those with 22q11.2 deletion syndrome, may present with a combination of these conditions.
Velopharyngeal Anatomy and Function
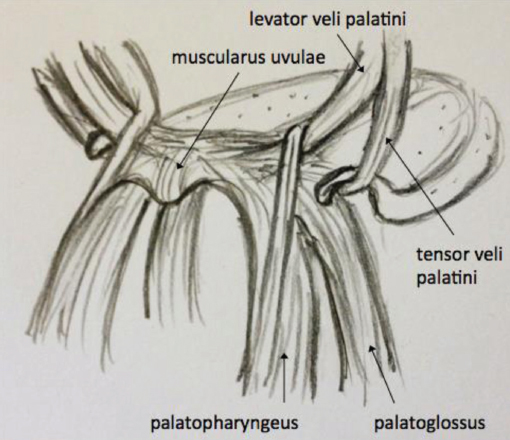
The velopharynx consists of the soft palate (also known as the velum, from the Latin word for curtain or veil) and the pharyngeal walls. These structures form a threedimensional valve controlling the passage of air, food, and liquids between the nasopharynx and the oropharynx. The underlying muscular structures contributing to the shape and function of the velopharynx are the muscles of the soft palate and the superior pharyngeal constrictor ( Table 72.1 ). The five muscles of the soft palate are the paired levator veli palatini, tensor veli palatini, palatoglossus, and palatopharyngeus muscles in addition to the midline muscularis uvulae ( Fig. 72.1 ). The levator veli palatini is the primary palatal elevator, acting as a sling to pull the soft palate in a posterior-superior direction upon contraction. 4 , 5 Contraction of the tensor veli palatini tenses the soft palate and also functions to dilate the Eustachian tube during swallowing. The muscularis uvulae runs in the parasagittal plane. Contracture provides bulk to the nasopharyngeal surface of the soft palate during velopharyngeal closure. The palatoglossus and palatopharyngeus have also been shown to affect the position of the soft palate as well as tongue and pharyngeal wall positioning during speech production. 6 The superior constrictor forms the upper lateral and posterior pharyngeal walls in a fan shape that converges along the posterior pharyngeal wall to form the pharyngeal raphe. Contraction of this muscle results in a constriction of the pharyngeal walls and may also aid in velar retraction. 7 The innervation of the velopharyngeal musculature is primarily from the pharyngeal plexus derived from the glossopharyngeal and vagus nerves. The one exception is the tensor veli palatini, which is innervated by the mandibular branch of the trigeminal nerve.
In addition to soft palate and pharynx, three additional structures contribute to the overall form and function of the velopharynx: the uvula, Passavant’s ridge, and adenoids (pharyngeal tonsils). The uvula is a midline mucosal appendage of the soft palate with contributions from the muscularis uvulae, and likely assists with velopharyngeal closure via added tissue bulk. 7 Passavant’s ridge is a transverse structure of the posterior pharyngeal wall seen during speech and swallowing. The ridge is thought to be formed by the localized contraction of the superior constrictor muscle. The vertical location of Passavant’s ridge relative to the soft palate is variable and may contribute to velopharyngeal closure in some individuals. 5 The adenoid pad, by virtue of its position in the posterior pharyngeal wall, also assists with the velopharyngeal valving mechanism. Because of this contribution, the regression of adenoid tissue in older children may result in the development of velopharyngeal insufficiency in a child with previously normal speech. 8 , 9 , 10
Closure of the velopharynx is required for the majority of English language speech sounds. An open velopharyngeal port is present only in the production of /m/, /n/, and /ng/sounds. Other sounds require varying degrees of forceful closure of the soft palate against the posterior pharyngeal wall. For example, the amount of force required to produce pressure consonants such as /s/, /z/, /k/, and /t/is higher than for vowel sounds. 7 Of note, the neurophysiologic mechanism for velopharyngeal closure during swallowing is distinct from the process of speech. Individuals who are able to obtain complete closure of the velopharyngeal port during swallowing can therefore still have marked velopharyngeal dysfunction. 11
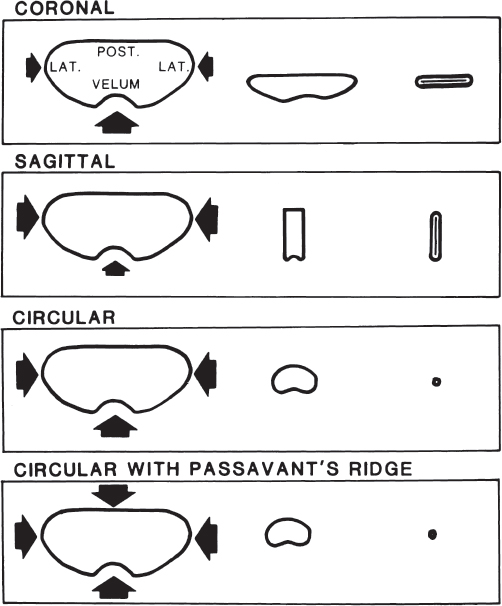
The pattern in which the velopharynx closes is variable. In 1981, Croft et al described four patterns of velopharyngeal closure. These closure patterns are (1) coronal, (2) sagittal, (3) circular, and (4) circular with Passavant’s ridge ( Fig. 72.2 ). Each demonstrates differential contributions from the velum, posterior, and lateral pharyngeal walls to the closure of the velopharynx from a “bird’s eye” view seen during a nasopharyngoscopic speech evaluation. 1 , 12 The significance of different velopharyngeal closure patterns will be further discussed in the evaluation and management sections.
Causes of Velopharyngeal Insufficiency
Congenital causes of velopharyngeal insufficiency are most commonly related to clefting of the palate and associated craniofacial anomalies. Palatal cleft phenotypes range from occult submucous cleft palate to complete bilateral cleft palate. An occult submucous cleft palate represents a diathesis of the levator veli palatini and muscularis uvulae, in the absence of a bifid uvula or a muscular diathesis appreciable on intraoral exam. A submucosal cleft palate classically consists of the triad of bifid uvula, notching of the posterior border of the hard palate, and diathesis of the soft palate musculature (creating a zona pellucida). 13 A zona pellucida is a semitranslucent area created by the nasal and oral mucosal contact in the region of the muscular diathesis. On a practical basis, most clinicians would make the diagnosis in a patient with a muscular diathesis and bifid uvula, with or without palpable notching of the hard palate. The significance of a submucosal cleft palate is that this subtle phenotype may often be overlooked, but speech therapy and/or surgical repair is often required due to the dysfunction caused by the anomalous muscular function. The remaining cleft palate phenotypes are incomplete secondary cleft palate (fullthickness clefting of the soft palate), complete secondary cleft palate (fullthickness clefting of the soft palate and hard palate to the incisive foramen), complete unilateral cleft palate, and bilateral cleft palate.
Diathesis of the muscles of the soft palate is therefore present in all palatal cleft phenotypes, accompanied by varying degrees of hard palate involvement. The aberrant orientation and deficiency of the soft palate musculature predisposes children with cleft palate to velopharyngeal dysfunction, even after palate repair. It has been reported that anywhere from 5 to 20% of patients with cleft palate will require a secondary surgery to address velopharyngeal insufficiency. 14 , 15 Of note, there exists an ongoing debate as to whether the type of palatal cleft and/or method of cleft palate repair contributes significantly to the proportion of patients with cleft palate who will later need a secondary speech surgery.
Congenital velopharyngeal insufficiency can also occur in the absence of palatal clefting. One of the more commonly recognized predisposing conditions for velopharyngeal insufficiency is 22q11.2 deletion syndrome, of which velocardiofacial syndrome (VCFS) is a phenotype. VCFS is characterized by palatal and conotruncal heart anomalies, characteristic facies, and developmental disabilities. Although palatal clefting is a known manifestation of VCFS, only 10% of patients with the 22q11.2 deletion have an overt palatal cleft, whereas approximately 70% have a palatal anomaly affecting velopharyngeal function. 16 Decreased neuromuscular function (velopharyngeal incompetence) overlies the anatomical anomalies, often complicating treatment. Studies suggest that the postoperative speech outcomes can be equivalent in VCFS and nonsyndromic patients using the same array of surgical procedures for velopharyngeal insufficiency. 17 , 18 , 19 However, more aggressive surgical techniques may need to be employed in patients with VCFS due to the limited pharyngeal wall motion typically observed. The possibility of a medially displaced carotid artery in the posterior pharyngeal wall should also always be taken into consideration due to the relatively high prevalence of internal carotid artery anomalies in this population. However, superiorly based pharyngeal flap surgery has been routinely performed in patients with VCFS with few complications, and preoperative vascular imaging is not considered mandatory. 20 , 21 Most surgeons feel that a careful exam for carotid artery pulsations during nasopharyngoscopy and intraoperatively is adequate.
Several other syndromic and nonsyndromic conditions have been associated with noncleft velopharyngeal insufficiency, but with less predictability than the aforementioned conditions. 22 Velopharyngeal dysfunction following adenoidectomy has been well documented as an acquired cause in patients with submucosal cleft palate and sometimes in otherwise healthy individuals, and in many cases may resolve with a short course of speech therapy. 23 , 24 , 25 A short palate, relatively deep nasopharynx, or hypotonic palate may all contribute to velopharyngeal insufficiency. The clinician must therefore rely on a thorough diagnostic evaluation of velopharyngeal dysfunction as the etiology of the condition may not be readily apparent.
Evaluation of Velopharyngeal Dysfunction
A complete assessment of velopharyngeal dysfunction consists of a perceptual and instrumental evaluation in conjunction with a thorough history and physical examination. Most surgeons will evaluate patients concurrently with a speech-language pathologist in order to identify patients who might benefit from surgical intervention as well as to ensure improved speech outcomes postoperatively. Valuable information to be gathered from a patient and family new to a multidisciplinary team includes number and timing of previous cleft palate or speech surgeries, any difficulties with intelligibility or communication noted at school or home, and the presence of any nasal regurgitation. Intraoral examination should note any palatal fistulae, zona pellucida, bifid uvula, aberrant carotid pulsations in the posterior pharyngeal wall, and tonsillar hypertrophy. Intraoral judgement of velar elevation can be misleading.
The perceptual speech assessment includes an evaluation of articulation and resonance. Compensatory articulation errors are common in patients with velopharyngeal insufficiency and consist of a change in the location of the sound production (e.g., substitution of a glottal stop) in order to produce a similar sound. In contrast, an obligatory distortion is an error in which the articulation placement is normal but an abnormality in the structure causes a distortion in speech, as is the case with nasal emission on consonants. 26 , 27 Types of abnormal resonance include hypernasality and hyponasality. Hypernasality is frequently observed in patients with velopharyngeal insufficiency; hyponasality is a common quality with nasal obstruction.
A number of provocative tests may be performed to further evaluate velopharyngeal function. A laryngeal mirror can be passed under the nares during phonation to test for nasal air emission, which will result in fogging of the mirror. Care must be taken to pass the mirror only after beginning phonation and removing it prior to the end of phonation to avoid falsepositives from normal nasal respiration. To help distinguish between hyper- and hyponasality, the patient’s speech can be evaluated with and without occlusion of the nares during phonation. Patients with hypernasal speech will have a significant change in resonance with nostril occlusion. 27 Set phrases may also be used to assess velopharyngeal closure, particularly those which isolate voiceless pressure consonants such as “p,” “t,” “k,” “f,” and “s,” with “s” being the most advanced sound. Representative phrases include “pick a puppy,” “bluebirds are pretty,” “red cars are fast,” and “Sissy sees the sky.” With repetition of these specific speech sounds, the evaluator can assess the ability to build up oral pressure and note inappropriate substitutions indicative of a compensatory articulation disorder. 26
A comprehensive instrumental evaluation of velopharyngeal dysfunction most commonly consists of nasometry, nasopharyngoscopy, and occasionally multiview videofluoroscopy. Nasometry is used to measure nasalance, which is a ratio of the acoustic energy produced from the nasal and oral cavities during speech. It is a commonly used indirect method of assessing velopharyngeal function in that higher nasalance percentages are associated with increased amounts of hypernasality. 28
Multiview videofluoroscopy allows for real-time evaluation of velopharyngeal function through a series of radiographic images. Barium is instilled in the nose to improve contrast visualization of the soft palate and pharyngeal walls for assessment of timing and degree of movement of these structures. 28 Videofluoroscopy is well tolerated and thought to allow for more accurate evaluation of lateral pharyngeal wall motion than nasopharyngoscopy, 29 but has the significant disadvantage of exposing the patient to ionizing radiation. Many centers will now utilize videofluoroscopy only when nasopharyngoscopy is unsuccessful.
Nasopharyngoscopy allows for direct visualization of the velopharyngeal structures during speech. Most children over 4 years of age tolerate this procedure in clinic when properly prepared and with the application of a topical anesthetic. Ideally, the endoscopy is performed with a speech-language pathologist including both video and audio recordings for subsequent review. Information that may be garnered from this evaluation includes palatal and lateral wall motion during speech with associated closure pattern, presence of Passavant’s ridge, aberrant carotid pulsations of the posterior pharyngeal wall, notching of the nasal surface of the soft palate, and estimation of velopharyngeal gap size and shape. 30 Drawbacks to this method of evaluation include occasional difficulty with patient cooperation, possible distortion of endoscopic images, and a twodimensional view with difficulty with vertical-level assessment. 31 Some surgeons may also lack access to appropriate equipment or personnel; however, nasopharyngoscopy is routinely available at cleft and craniofacial teams. In 1993, D’Antonio et al reported the results of a national survey in which 90% of respondents reported the availability of nasopharyngoscopy and agreed that the procedure was important for difficult diagnostic cases. 32 The current standards of care recommend an evaluation of dynamic palatal function prior to corrective speech surgery, as it allows for customization of the surgery.
Of note, the utility of nasopharyngoscopy and multiview videofluoroscopy is not limited to determining the need for specific type of surgical intervention. Both instrumental modalities have been used as a method of biofeedback to correct inconsistent velopharyngeal closure and improved velopharyngeal valving with targeted speech therapy alone. 33 , 34 , 35
The combined information gathered from nasopharyngoscopy and multiview videofluoroscopy has led to the description of different patterns of velopharyngeal valving. The most widely accepted classification was described by Croft et al, which includes coronal, sagittal, circular, and circular with Passavant’s ridge patterns of closure based on the relative contributions of the soft palate, lateral, and posterior pharyngeal walls during closure of the velopharynx ( Fig. 72.2 ). These closure patterns are present in both healthy subjects as well as those with velopharyngeal insufficiency. 12 The pattern of velopharyngeal valving is information used by many to determine which technique to use in the surgical correction of velopharyngeal insufficiency, and is described in the surgical treatment section. A standardized method of reporting both nasopharyngoscopy and multiview fluoroscopy findings has been proposed by a multidisciplinary international working group; the resultant scale was published by Golding-Kushner et al in 1990. 31 The Golding-Kushner scale is a rating system to quantitatively describe palatal and pharyngeal wall movement ( Table 72.2 ). This scale shows promise for achieving standardization between groups evaluating velopharyngeal dysfunction, but strong interrater and intrarater reliability is still lacking in studies utilizing this scale. 30 , 31 , 36 Future developments in the evaluation of velopharyngeal dysfunction will likely include teaching and greater utilization of a standardized scale to allow for improved outcome comparison, as well as exploration of other imaging modalities such traditional and cinematic magnetic resonance imaging. 37
Variable | Value range (subjectively scaled) |
Right lateral wall | 0–0.5 a |
Left lateral wall | 0–0.5 a |
Right palate | 0–1.0 b |
Left palate | 0–1.0 b |
Posterior pharyngeal wall | 0–1.0 c |
a 0, no movement; 0.5, movement to midline. b 0, no movement; 1.0, movement to posterior pharyngeal wall. c 0, no movement; 1.0, movement to posterior edge of soft palate. Increments are 0.1. | |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


