71 Hemifacial Microsomia and Distraction Osteogenesis
Introduction
Hemifacial microsomia (HFM) is a congenital, nonheritable condition affecting the first and second pharyngeal arches, with dysmorphology and underdevelopment of requisite craniofacial structures. 1 , 2 , 3 , 4 A number of names have been designated to describe this process and associated constellation of findings. 5 , 6 Bilateral craniofacial or bifacial microsomia is used when both sides are involved. This primarily unilateral birth defect can affect the skeletal, nerve, and soft tissues related to the first and second branchial arches with various gradations. Furthermore, broadspectrum HFM can lead to ocular, renal, cardiac, and spinal aberrations. 7 , 8 Gorlin et al and Peterson-Falzone provide an extensive overview of the wide range of anomalies witnessed in HFM. 2 , 9
Pathogenesis
At an incidence of 1 in 5,600 live births, HFM remains the second most common congenital craniofacial anomaly after cleft lip and palate. 10 , 11 Various theories have persisted in the literature for explaining the pathogenesis of HFM. Almost all of these implicate the disruption of the normal development structures derived from the first and second pharyngeal arches. Stark and Saunders espoused that mesodermal aberration, or deficiency, contributes to the development of HFM. 12 Poswillo created a mouse model with vascular disruption and concomitant triazene administration leading to an expanding hematoma and, ultimately, phenotypic features of HFM. 13 The resultant damage from this and subsequent hematomas produces a wide spectrum of asymmetric malformations similar to the diversity of aberrations witnessed in HFM. 14 The superficial similarities including external/middle ear aberrations, vertebral anomalies, and cardiovascular inflow disruption between HFM and retinoic acid syndrome (RAS) have led some to apply the factors implicated in RAS for HFM; that is, the interruption of the neural crest development may be responsible for HFM. 15 , 16
Classification
The diverse number of abnormalities, each with its own degree of deformity as described, has spurred a multitude of classification schemes. Early attempts to classify HFM formulated around the auricular and mandibular aberrations graded by Meruman and Pruzansky, respectively. 17 Converse espoused that a classification scheme would be difficult, if at all feasible, due to the heterogeneity of HFM, stressing the importance of evaluating each case on an individual basis.
Yet, classifications do exist based on phenotypic features, namely the mandible and temporomandibular joint (TMJ), as mentioned above. Two classifications capturing these characteristics along with other salient features of HFM are the SAT and OMENS. 5 The SAT classification focuses only on three aspects of HFM: skeletal, auricle, and soft tissue. It denotes five degrees of skeletal deformity (S1 to S5), four degrees of auricle deformity (A0 to A3), and three degrees of soft tissue deformity (T1 to T3). Yet, it neglects to encompass other features of this syndrome, including the facial nerve.
The optimal classification system should comprehensively characterize the broad pathology encountered in HFM in a succinct and objective manner facilitating a standardized evaluation of a HFM patient. Vento et al’s OMENS classification 18 , 19 (later modified slightly) that builds on and often fully incorporates the classification systems by Meurman, Pruzansky, Kaban, and Murray appears currently to be the best to achieve this. 17 , 20 , 21 , 22 Specifically, it expands on the SAT classification to characterize the following: orbit, mandible, ear, facial nerve, and skeletal. Each entity receives a score from 1 to 3 based on severity with 0 being normal. While the OMENS has been criticized by Cohen for neglecting extracraniofacial abnormalities, 23 its modification by Hogan et al in 1995 that places a “+” denoting a noncraniofacial manifestation addresses this shortcoming. 19 Despite modified OMENS not defining the degree of vertical dystopia and size of the orbit with radiologic findings and neglecting middle ear and preauricular deficits, it still serves as a comprehensive and robust classification that can evaluate a HFM patient in a standardized fashion facilitating surgical treatment. Given this background, the characteristics will be presented in concordance with the OMENS+ classification.
Characteristics
Orbit
The deformity of the orbit relates to the bony abnormalities affecting size and position with vertical dystopia often present ( Fig. 71.1 ). The latter can be either superior or inferior as compared to the unaffected orbit and an integral component of the classification scheme. 24 , 25 The constellation of ocular anomalies include epibulbar dermoids, microphthalmos, colobomas, and ocular motility dysfunction. 26 Bony abnormities include diminutive orbital rim with accompanied retrusion of the lateral and inferior orbital rims.

Mandible
HFM manifests in varying degrees leading to multiple classification systems with the mandibular deformity central to these schemata. 27 In 1969, Pruzansky classified the mandible according to three different types based on plain X-rays 21 that later Kaban et al modified with respect to the condyle and TMJ relationship. 18
In type I, while all parts of the affected mandible and attached muscles exist, they are hypoplastic to a certain degree. The glenoid fossa tends to be missing with compromise of translatory joint movement and concomitant preservation of rotational movement. During jaw opening, the mandible shits to the affected side. Types IIa and IIb can be differentiated by the involvement of the condyle with it displaced anteriorly and medially in the former and absent in the latter. Furthermore, the lateral pterygoid muscle tends to be missing in type IIb with profound jaw and facial asymmetry. In type III, the proximal ramus-condylar unit is absent (missing TMJ), and the masticatory muscles tend to be severely hypoplastic ( Fig. 71.2 ). Though the Pruzansky/Kaban mandibular classification focuses on the proximal mandible, we have recently shown that the dentate segment (distal mandible) is also proportionally affected (diminished). 28
Ear
While mandibular hypoplasia tends to be the hallmark of HFM, ear abnormalities are almost as frequently witnessed ranging from 67 to 100% in HFM individuals. 15 , 29 The auricular abnormalities in HFM exist over a wide range from an ear tag to vestigial appendage of the ear ( Fig. 71.3 ). 30 While the deformity of the ear corresponds with that of the mandible, it does not directly correlate with hearing function. 31 , 32 The ear on the affected side tends to be inferiorly positioned with middle ear components often impaired or absent. Often, these patients can present with conductive hearing loss as well as sensorineural hearing loss, particularly when the external auditory canal is absent. 33 The Meurman classification has been incorporated in the OMENS gradation consisting of the following 34 :

Grade I: Normal shape; all components of the ear are present but deficient.
Grade II: There is only a vertical remnant of cartilage and skin.
Grade III: Only a lobule is present; some patients have anotia.
Neurologic
Complete or partial paralysis of facial nerve on the ipsilateral affected side can be observed in 10 to 20% of HFM patients. 10 , 35 Specifically, the marginal mandibular branch of the facial nerve tends to be implicated. The course of the facial nerve may be aberrant and the surgeon must recognize this when proceeding with temporomandibular reconstruction. 4 Hypoplasia or paralysis of the tensor veli palatini occurs, leading to soft palate deviation to the opposite side. 4 , 10 Studies demonstrate that in HFM velopharyngeal insufficiency is present in 55% of patients, of whom 7 to 15% have cleft lip or palate. 36 , 37
Soft Tissue
Macrostomia proves to be a common finding in HFM, particularly in patients with Goldenhar’s syndrome. The soft tissue deficiency parallels the severity of HFM deformity, with temporalis muscle, muscles of mastication, parotid tissue, and overlying subcutaneous tissue involved. Fan et al examined 198 patients with HFM finding 23% of patients with cleft of oral commissure (macrostomia, or Tessier no. 7 cleft) and 10% of patients with cleft lip and palate. 38 Other studies have confirmed the association of the Tessier no. 7 cleft with HFM. 10 , 39 Yet, the recent Woods et al retrospective examination of their patients at the Australian Craniofacial Unit with Tessier no. 7 clefts without ear or major mandibular deformations has led the authors to conclude that Tessier no. 7 clefts are part of a rare clefting phenomenon distinctly different from HFM. 40 Tongue hypoplasia has historically been deemed an uncommon finding in HFM. However, recent reports demonstrate that this finding may be underestimated. 41 After performing a retrospective review of 20 years, the authors demonstrated a relatively low incidence of tongue dysmorphology (4.8%). However, in the same study, the authors performed a thorough prospective study to evaluate patients for tongue dysmorphology in the context of HFM and found that 43.6% had some degree of tongue dysmorphology. In the same study, tongue dysmorphology correlated with the degree of hard and soft tissue deformity. 41 Overall, it appears that tongue dysmorphology is frequently overlooked.
Treatment
The treatment for HFM is multidisciplinary and is best approached through a coordinated effort of multiple specialists. Each patient will have specific needs to be addressed, which can include issues with hearing, speech and language, breathing, social concerns, ocular deformities, and others. The craniofacial team should include medical professionals from multiple disciplines. Specific components will need to be addressed, including the zygomatic and orbital regions, the maxillomandibular region, soft tissues, and internal and external ear. 42
Timing
The timing of treatment in HFM is individualized based upon the patient’s regions of involvement. Factors to consider when deciding on optimal time include the patient’s functional needs/desires, age, and the level of growth and development. A treatment timing algorithm is shown in Table 71.1 .
Initial studies on HFM presented concerns that the primary deformities of HFM may lead to further secondary deformities. The initially hypoplastic mandible was thought to interfere with the normal downward growth of the maxilla, and thereby cause a secondary distortion of the midface, 20 , 29 and initial reports also believed that HFM may be progressive in nature. Therefore, treatment of HFM demonstrated an advocacy toward early intervention to prevent growth-related deformities. 18 , 19 However, there is not a consensus regarding the progression of facial asymmetry in HFM. 17 , 30 , 32 Authors have demonstrated that the facial proportions of HFM patients are maintained throughout growth even when not treated. These same proportions may return to their original asymmetry, even after distraction osteogenesis for patients with vertically severe type I and II mandibles, 43 if occlusal appliances or orthodontic intervention are not performed in concert. The previous advocacy toward early surgery to prevent growth-related deformities, therefore, has given way to a more individualized treatment algorithm. Even with early intervention, surgery at a later stage in life is often necessary.
Regardless, there remain indications for early intervention. Numerous studies delineate the negative effect of facial deformities upon the psychosocial aspects of the child’s life. 13 , 44 , 45 , 46 , 47 , 48 Intervention may be considered at the first- or second-grade level in order to minimize these effects while capitalizing upon the presence of the 6-year molars and subsequent eruption of permanent teeth. For Pruzansky IIA mandibles, vertical distraction can be considered at this time. After distraction, the patient’s maxillary dentition is allowed to erupt downward to close the lateral open bite, thereby improving stability, possibly preventing relapse, and minimizing the secondary deformity. This early intervention may lessen extent of future operations by both lessening the deformity and generating bone stock to be used for future, definitive procedures.
The authors of this chapter agree with earlier intervention, if necessary, for the more severely affected patients. As stated, patients with type IIB or III Pruzansky mandibles may have psychosocial difficulties, and furthermore, a functional joint will be needed for later formal orthognathic surgery. In such instances, the benefits of early intervention may outweigh the risks and are actually requisite to later intervention.
Mandible
The mandibular deformity in HFM is complex with diminished structure in all planes of space. The resultant functional aberrations depend on the degree and planes of deficiency. Essentially, there are three broad treatment interventions to address the mandibular deformity. (1) For patients with retrognathia, horizontal shortening of the chinpoint, and/or clockwise mandibular rotation with resultant glossoptosis and airway obstruction, bilateral horizontal or multiplanar mandibular elongation is required with net movement of the chin point forward to open the airway. (2) For isolated vertical ramus deficiency, the hemimandible can be elongated or addressed by one of several techniques: distraction between a functional TMJ and angle/body, transport distraction to create a new TMJ and subsequent ramal lengthening, or vascularized or nonvascularized bone graft with down and forward rotation of the native mandible. (3) For patients who necessitate correction of coronal, sagittal, vertical, and transverse discrepancies, a combination of the above techniques is required, often in concert with treatment of the maxilla during definitive orthognathic surgery. Ultimately, the diagnosis is critical to make the correct decision for how and when to intervene for each of these mentioned indications.
Retrognathia and Possible Airway Obstruction
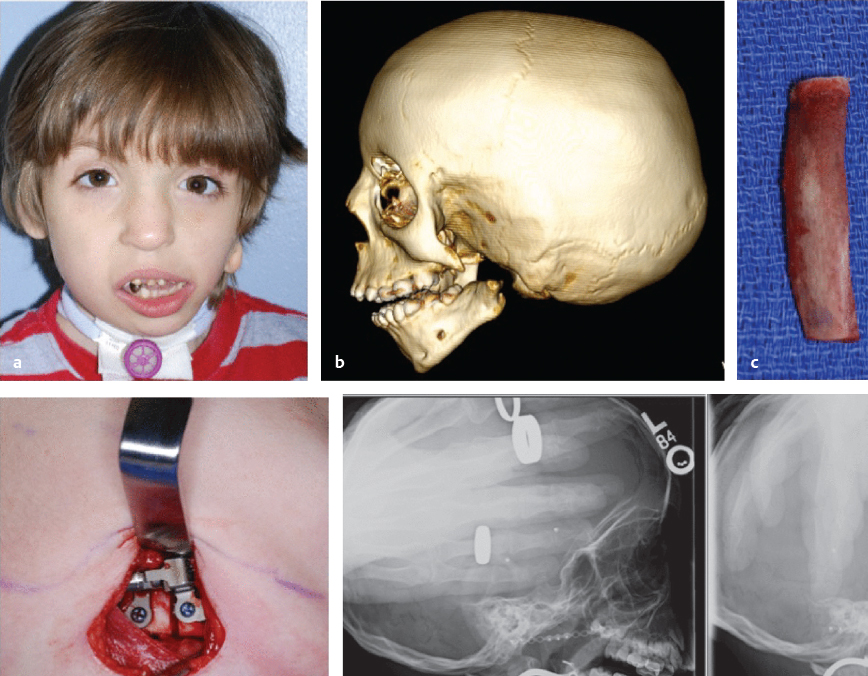
If there is airway compromise in the neonatal period, bilateral mandibular distraction osteogenesis can be used early to facilitate increases in airway volume and prevention of tracheostomy ( Fig. 71.4 ). Distraction osteogenesis offers advantages over conventional therapies, including new bone formation with concomitant expansion of the overlying soft tissues. Also, it can be used to facilitate tracheostomy decannulation in young children. In general, if there is no functional obstruction or airway compromise, the initial lengthening procedures for mandibular hypoplasia take place between 6 and 8 years old. Of note, an important consideration in determining the timing of maxillomandibular reconstruction is the patient’s TMJ anatomy. 49 , 50 , 51 Pruzansky type I mandibles may not require treatment. In mild cases in which there is no functional compromise and both the patient and the family are unconcerned with the presenting facial aesthetics, it is likely best to delay treatment until adolescence so that facial growth has time to complete. This will likely compromise reconstructive jaw surgery (BSSO ± Le Fort I ± osseus genioplasty) in addition to orthodontic treatment. 49

Vertical Ramus Deficiency6Temporomandibular Joint
The hemimandible can be elongated in a number of different ways. If the TMJ is functional and of adequate bone stock, distraction osteogenesis between the functional TMJ and the angle or body can adequately treat the deformity (see the following section for further description and Fig. 71.5 ). Transport distraction can be used to re-create a functioning TMJ, and the ramus can subsequently be lengthened. Pruzansky type IIA and type IIB deformities are often severe enough to require treatment in the mixed dentition stage due to the effect these deformities have upon the psychosocial aspects of the child’s life. 13 , 44 , 45 , 46 , 47 , 48 Early intervention, as stated previously, is controversial in patients with these specific deformities, but the goal of intervention would be to prevent the negative psychosocial effects from occurring as well as building a functional TMJ. These deformities will likely benefit from distraction lengthening during this time period, with overcorrection being the goal. If a more involved first-stage mandibular reconstructive procedure is carried out during this phase of the patient’s life (mixed dentition), then further reconstructive surgery should be anticipated—the thought that mandibular reconstruction at this stage can be done to avoid osteotomies in adulthood is unrealistic.

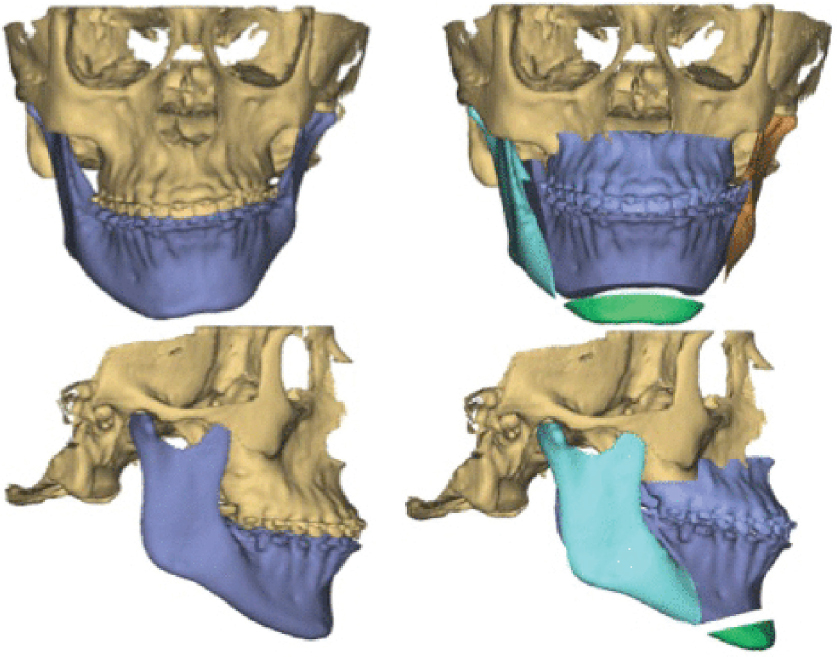
For Pruzansky type III mandibles (and some type IIB), which have severe ramal and condylar hypoplasia as well as deformed TMJ complexes, further reconstructive endeavors are often necessary. In these patients, replacement of the defective TMJ is necessary to reconstruct not only the missing mandibular condyle but also to create an articulating fossa. Most often, a costochondral graft is used to reconstruct the mandibular ramus, condyle, and TMJ ( Fig. 71.6 ). 18 , 52 , 53 With respect to future orthognathic surgery, the main requirement of the graft procedure is to buttress the most proximal portion of the vestigial ramus or condyle against the base of the skull.
The natural history of rib grafting is often unpredictable. 54 , 55 At times, rib grafts may actually overgrow, which then require setback procedures as the patient completes skeletal growth. Other times, the graft may resorb or dissolve entirely, and require regrafting to complete treatment. These problems can be at least alleviated when the procedure is carried out in a child who is late in the mixed dentition stage, when at least 2 mm of cartilage is left at the articulating surface, or when facial growth has been completed. 56 , 57 , 58 , 59 , 60
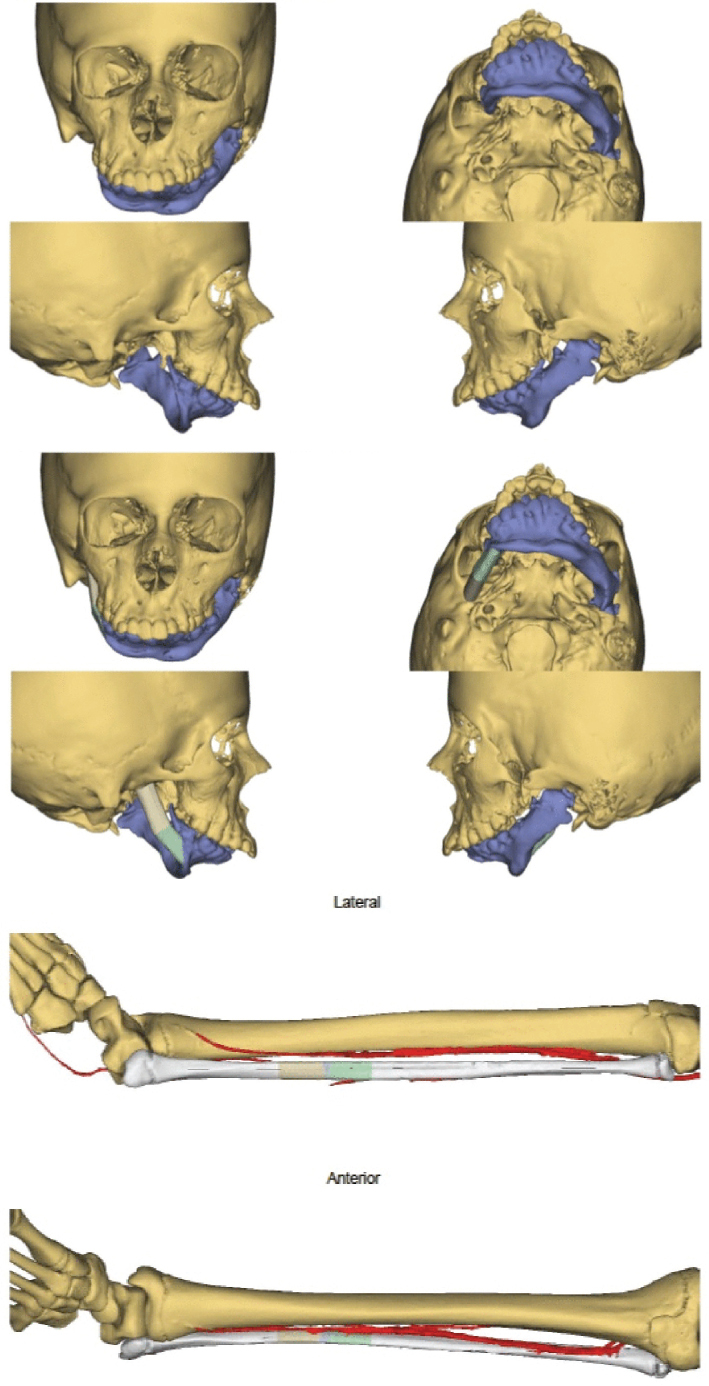
For the most severely affected patients, a vascularized free fibular flap is another viable and often more predictable option ( Fig. 71.7 ). Due to the above-mentioned concerns with the unpredictability of rib grafting and possible resorption, microsurgical mandibular reconstruction has emerged as a more stable method of treating type IIB and type III patients. Authors have demonstrated successful longterm reconstruction, including both singular ramal reconstruction as well as ramus and body reconstruction using fibular osteotomies. Furthermore, these authors have demonstrated successful distraction of the vascularized bone, with obvious greater success than that of the nonvascularized costochondral grafts. The fibular free flap is becoming the workhorse for mandibular reconstruction because of its abundant bone stock, ease of dissection, ability to facilitate simultaneous dissection of the recipient and donor sites, low donor-site morbidity, and track record for successful distraction osteogenesis. Additional benefits are the ability to perform multiple osteotomies without compromising blood supply and the use of septocutaneous perforators to obtain soft tissue to remodel facial contour. 61 , 62 , 63 , 64 , 65
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


