68 Evaluation and Management of Cleft Lip and Palate Disorders
Introduction
Of all facial plastic surgery procedures, few are as rewarding as repairing orofacial cleft deformities. Patients with cleft lip and/or palate and associated nasal deformities experience difficulty with feeding and effective speech production, in addition to overwhelming social stigmata accompanying the obvious alterations in appearance and facial growth. The treatment of such patients is a challenging task, requiring a multidisciplinary team of providers to manage the myriad aesthetic, dental, psychosocial, speech, and otologic needs of these individuals. 1 This chapter reviews the embryology, anatomy, and classification of both unilateral and bilateral cleft malformations. Treatment philosophy, including the timing and technique of various cleft repairs, is also described.
Embryology of the Lip and Palate
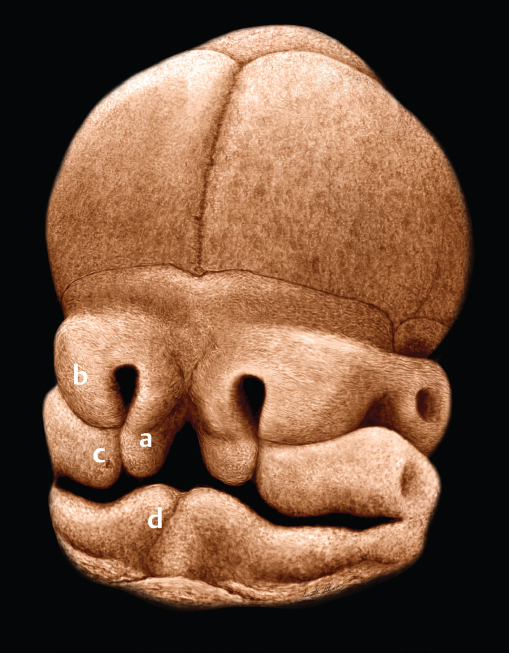
Normal development of the lip and palate occurs during the embryonic period, in the first 12 weeks of intrauterine life. The midportion of the face develops anterior to the forebrain by differentiation of the broad midline frontonasal prominence. The primary palate forms at 4 to 6 weeks and forms the initial separation between the oral and nasal cavities. The primary palate, or median palatine process, is formed by the fusion of the paired medial nasal prominences, and is that portion of the hard palate anterior to the incisive foramen. Fusion of the paired medial nasal prominences during the sixth week gives rise to the philtrum, the premaxilla, the columella, the nasal tip, and the central and lateral incisors ( Fig. 68.1 ). 2 , 3 Development of the primary palate is embryologically distinct from the formation of the palate posterior to the incisive foramen (the secondary palate). The lateral elements of the upper lip (lateral to the philtral columns) are derived from the paired maxillary processes. The cheek, maxilla, zygoma, and secondary palate are also formed by the maxillary processes. The upper lip, therefore, is formed by both the medial nasal and maxillary processes in concert. 4
The secondary palate begins developing at roughly 8 weeks of gestation, after development of the primary palate is complete ( Fig. 68.2 ). Formation of the secondary palate occurs by superomedial growth and migration of the palatal shelves (the medial projections of the posterior maxillary processes). As the palatal shelves migrate, the developing nasal cavities expand laterally and inferiorly.
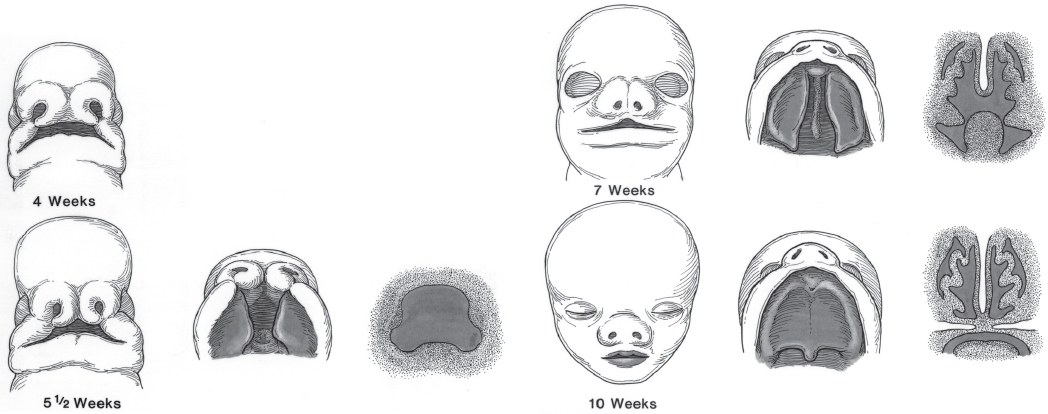
The palatal shelves are initially separated by the developing tongue. Growth of the mandible is associated with inferior displacement of the tongue, which allows the palatal shelves to migrate superiorly and assume a horizontal orientation. The “shelf elevating force” that causes the upward motion of the shelves is believed to be mediated by a process involving mesenchymal proliferation and growth factor–induced changes in local extracellular matrix, including hydration of hyaluronic acid in the tips of the shelves. 5 , 6 If fetal development and mandibular growth do not proceed normally, the tongue does not descend and the palatal shelves cannot migrate superiorly and medially, despite the shelf elevating force. The resulting malformation can result in the Pierre Robin sequence (micrognathia, relative macroglossia, and U-shaped cleft palate) ( Fig. 68.3 ). 7
Normal palatal formation begins when the palatal shelves and nasal septum contact each other and fuse in an anteriorto-posterior direction. Fusion is explained by cell signaling interactions between the epithelium of the palatal shelves and its deeper mesenchyme. 8 Palatal closure first occurs at the incisive foramen at roughly 8 weeks of gestation and is usually completed through the uvula by 12 weeks. The degree of clefting of the secondary palate is related to many factors, including when in fetal development the fusion process is interrupted. Therefore, a spectrum of palatal abnormality exists that can involve varying degrees of soft and hard palate clefting. 9
Cleft Classification
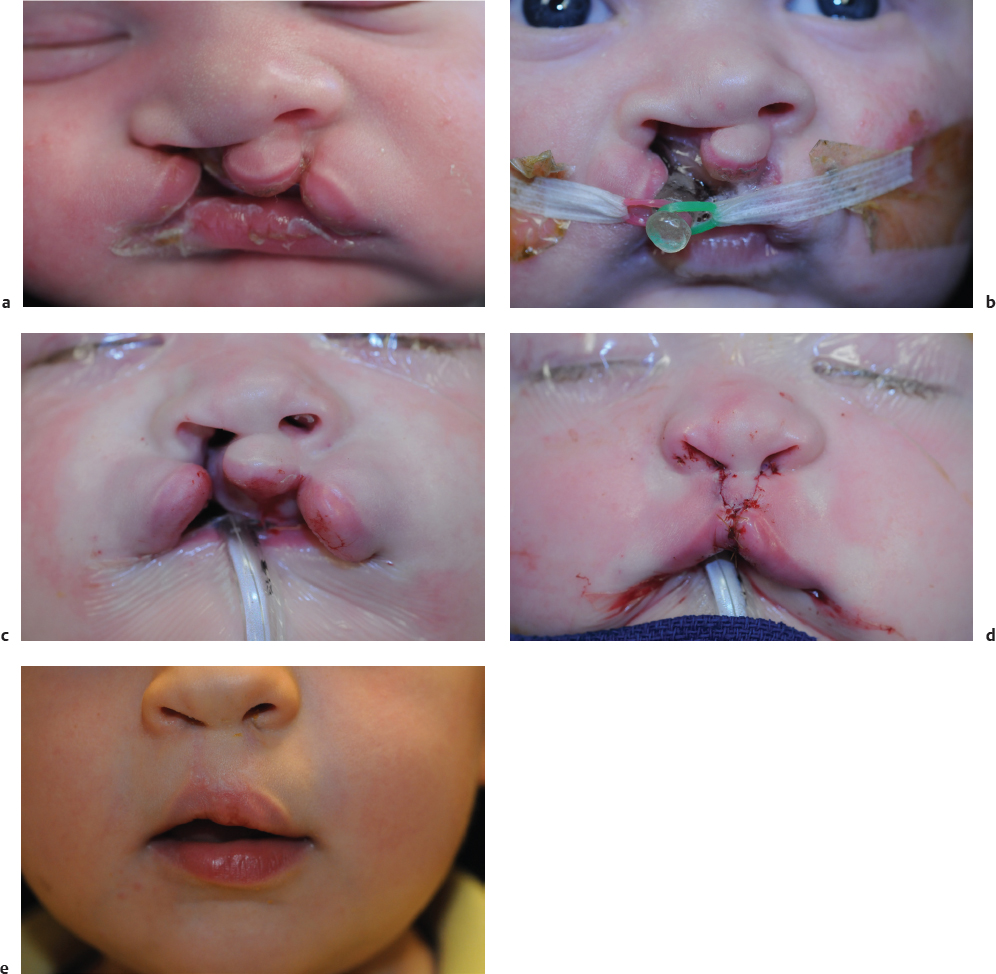
The embryologic development of the lip and palate serves as a natural framework to classify congenital clefts. The primary palate and lip develop between weeks 4 and 8. Interruption of this development will cause clefts of the lip and central alveolus (primary palate). Clefts of the lip may be unilateral or bilateral, complete or incomplete. They may be isolated in an otherwise normal child or associated with clefts of the palate or other malformations (syndromic clefts). Human cleft lip, with or without associated cleft palate, is caused by failure of the medial nasal prominences to make contact with the lateral nasal prominences and maxillary processes during embryogenesis. Interruption of this embryonic process creates malformation of some or all of the upper lip, central alveolus, and primary palate. A minor malformation of normal development may cause diastasis of the central orbicularis oris muscle fibers, with no overt clefting of the epidermis of the upper lip. This condition is known as a microform cleft lip deformity ( Fig. 68.4 ). An incomplete unilateral cleft lip involves a fullthickness deficit of skin, muscle, and mucosa, but does not extend superiorly through the entire lip height ( Fig. 68.5 ). A complete unilateral cleft lip occurs when a fullthickness cleft extends through the entire height of the lip and floor of the nose ( Fig. 68.6 ). A cleft of the alveolus is almost always associated with complete clefting of the lip.



The degree of clefting of the upper lip depends on the timing and degree of interruption of normal lip development. If disruption occurs on both sides of lip development, a bilateral cleft lip results. In the incomplete bilateral cleft lip, there is skeletal continuity and little or no protrusion of the premaxilla ( Fig. 68.7 ). In the complete bilateral cleft lip, the premaxilla is totally detached from each maxilla ( Fig. 68.8 ).


Either the unilateral or bilateral cleft lip deformity may be isolated or associated with clefts of the alveolus or palate. Because a more substantial interruption of lip development is required to create a bilateral cleft lip, this deformity is more likely to be associated with clefting of the secondary palate than is the unilateral cleft lip.
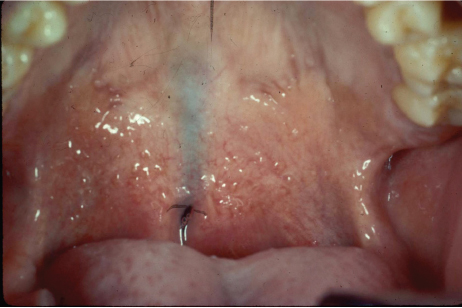
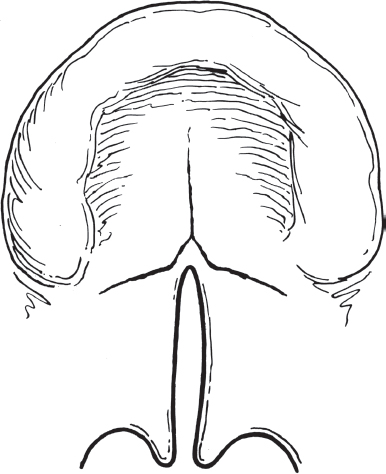
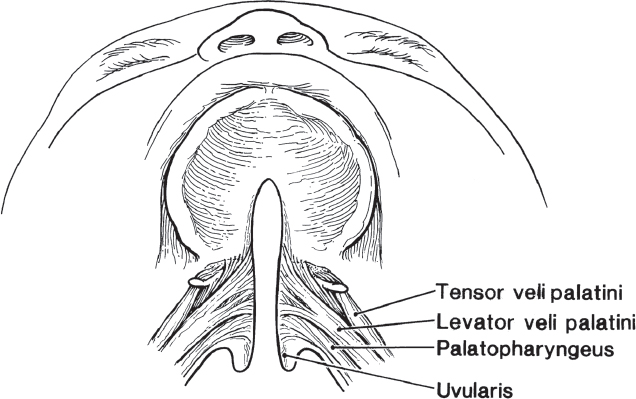
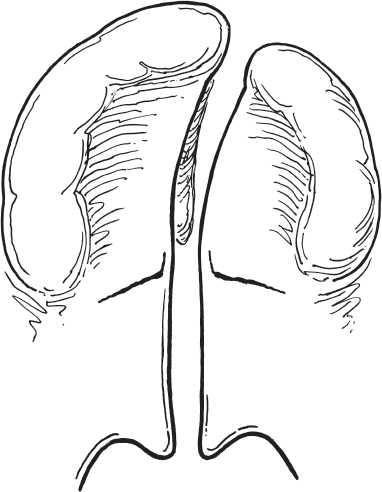
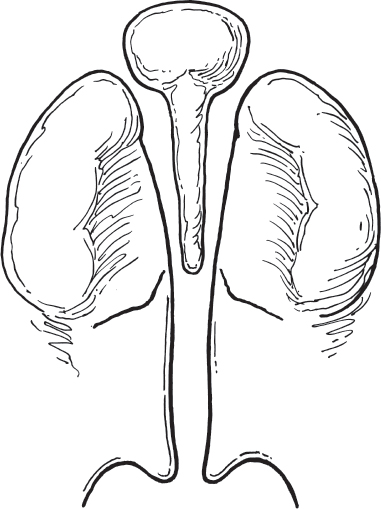
As with cleft lip, clefts of the secondary palate display variable expression. A bifid uvula is the mildest expression of soft palate clefting. This common deformity occurs when there is a lack of normal uvular fusion. A submucous cleft palate occurs when there is diastasis of the soft palatal musculature ( Fig. 68.9 ). In this condition, the palatal mucosa is intact, but speech therapy and/or surgical repair are often required because of intrinsic muscle dysfunction caused by the diastasis. Detection of submucous cleft palate can commonly be delayed into childhood, manifesting when speech dysfunction and/or chronic otitis media becomes noted. 10 , 11 Fullthickness clefting of the soft palate (incomplete cleft of the secondary palate) may also occur ( Fig. 68.10 ). Finally, complete clefting of the secondary palate may result from total interruption of the normal formation of the palate posterior to the incisive foramen ( Fig. 68.11 ). 12
Clefts of the secondary palate may be associated with complete cleft lips and are designated as complete clefts of the lip and palate. Complete cleft lip and palate may be unilateral or bilateral. The complete unilateral cleft lip and palate usually involves attachment of the vomer to the maxillary palatal shelf of the noncleft side ( Fig. 68.12 ), whereas complete bilateral cleft of the lip and palate usually exhibits vomerine and premaxillary detachment from the two lateral palatal shelves ( Fig. 68.13 ). In all cases, clefting of the upper lip and palate is variable in expression and typically follows known embryologic patterns.
Timing of Surgery and Philosophy of Cleft Repair
The decision when to repair a cleft lip or palate is based on a variety of factors, including patient growth and development, safety to undergo anesthesia, speech development, facial growth, and psychosocial impact. As always, the risks, alternatives, and benefits of repair need to be fully discussed with the parents or guardians prior to any procedure. The timing of cleft repairs is outlined in Table 68.1 . 13
In patients with cleft palate, tympanostomy tube insertion can be performed at age 3 to 6 months to overcome Eustachian tube dysfunction, treat chronic otitis media with effusion, aerate the middle ear space, decrease conductive hearing loss, and minimize the likelihood of chronic ear disease. Because the literature increasingly supports early intervention in children with hearing loss and given that tympanostomy tube placement is associated with few complications, the benefits outweigh the risks of this additional procedure. 14 , 15 , 16 In patients with cleft lip and palate, the lip repair and tympanostomy tube placement are commonly performed together, at roughly 3 months of age, unless the use of nasoalveolar molding is employed, necessitating later repair. Cleft palate repair is typically performed at 9 to 18 months, in the timeframe prior to the initial development of speech to minimize the possibility of velopharyngeal dysfunction (VPD). Greater defect widths and/or the presence of sleepdisordered breathing will often be the reasons for later repairs. Short duration tympanostomy tubes (e.g., Paparella I tubes) can be exchanged for long duration tympanostomy tubes (e.g. modified Goode t-tubes) at the time of palatoplasty.
After cleft palate repair, patients are monitored carefully for speech development, usually beginning at age 2 years. If VPD is identified, a VPD workup including nasopharyngoscopy and videofluoroscopy is performed. If the degree of VPD is significant and recalcitrant to speech therapy, additional surgical treatment can be performed between 5 and 7 years of age.
Other surgical treatments for cleft deformities include alveolar bone grafting after deciduous teeth have exfoliated at roughly 9 to 11 years of age, cleft rhinoplasty at 12 to 16 years of age, and orthognathic surgery after age 16 years, when growth of the facial skeleton is complete. The need for these interventions is related to the initial deformity as well as the growth and development of the patient.
Presurgical Nasoalveolar Molding
Presurgical nasoalveolar molding (PNAM) is a treatment used to improve the outcomes of surgical repair for cleft lip and palate. Different forms of maxillary orthopedics have been employed for centuries, with descriptions of taping, molding, using straps, and wiring patients to reduce the size of the cleft. 17 McNeil described modern use of this presurgical infant maxillary orthopedics technique in the 1950s. His technique focused on ways to manipulate the alveolar cleft or premaxilla. 18 Grayson, Cutting, and Wood introduced a molding technique that went beyond previous descriptions, addressing the alveolus, the lip, and the nose. 19 This is the foundation for current nasoalveolar molding.
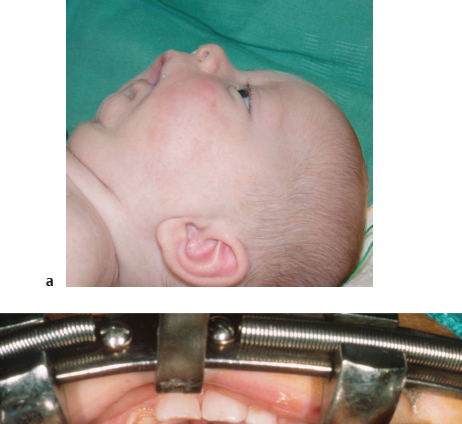
A heavy-bodied silicone material is used to make the first impression as soon after birth as possible. The impression is then used to make a dental stone model, from which an acrylic mold is created ( Fig. 68.14 ). The acrylic mold is fashioned with a retention arm, placed at a 40-degree angle to prevent unseating of the mold and allow for proper movement, or activation, of lip and alveolus ( Fig. 68.15 ). This device is secured in place to the cheeks bilaterally with surgical tape and elastic bands ( Fig. 68.16 ). The mold is kept in place nearly all the time, with the exception of daily cleaning and possible alterations needed for feeding early on in the use of PNAM. The mold is adjusted weekly to reduce the size of the alveolar cleft and improve positioning of the upper lip. As the cleft is reduced, a nasal stent is added to help lengthen the columella and reshape nasal cartilages ( Fig. 68.17 ).




The central goal of PNAM is to achieve better surgical outcomes in patients with cleft lip and palate. This is accomplished by a decreased size of the alveolar cleft, allowing for reduced tension on lip and palate repair, improved position of the nasal cartilages, and increased length of the columella ( Figs. 68.18 and 68.19 ). Today, most surgeons that employ this technique use this for wide, complete unilateral clefts of the lip and palate; wide, bilateral clefts of the lip and palate; bilateral clefts with significant asymmetry; and bilateral clefts with “locked-out” premaxillary segments. Larger studies looking at objective outcome data of PNAM are still needed to establish indications and show the longterm effects.

Cleft Lip
Anatomy of the Lip
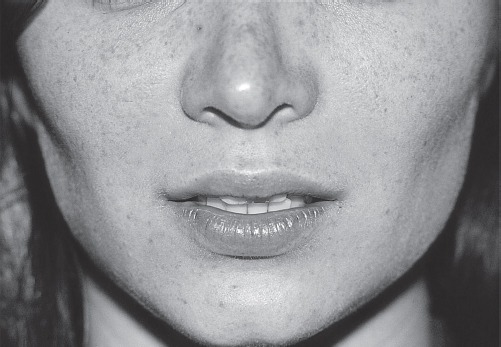
The upper lip can be divided into red (mucous membrane) and white (cutaneous) components. The vermilion (Latin vermiculus, “small worm”) is the dry portion of the lip’s red mucous membrane. It is a modified mucosal membrane lacking pilosebaceous units, salivary glands, or eccrine glands, bordered superiorly by the vermilion-cutaneous junction (i.e., the vermilion border). This mucocutaneous junction serves as an important aesthetic element separating the convex red lip from the concave white lip. A round roll of epithelium is present just superior to the vermilion border, called the white roll. 20 The white roll spans the entire upper lip, reflecting ambient light ( Fig. 68.19 ). Precise reconstruction of the mucocutaneous junction and white roll of the upper lip is essential in reestablishing normal upper lip aesthetics.
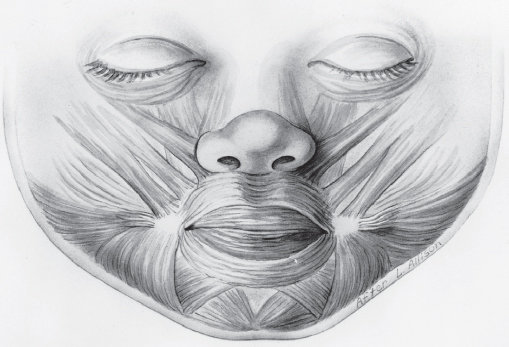
The muscles of the upper and lower lips play an important role in the appearance and function of the lips. Careful attention is therefore required when recreating muscle continuity in repair of any congenital or traumatic deformity. The principal muscle of the lips is the orbicularis oris ( Fig. 68.20 ). This muscle encircles the oral orifice, forming a sphincter within the substance of the lips. 21 The superficial layer of this muscle arises from the dermis and passes obliquely to insert into the mucous membrane lining the inner surface of the lips. The fibers of the deep layer arise from the maxilla above and the mandible below. 22 The orbicularis oris is innervated by the buccal and marginal mandibular divisions of the facial nerve.
Unilateral Cleft Lip
The unilateral cleft lip deformity may involve any combination of skin, muscle, and underlying mucosa. As previously discussed, microform cleft lip involves clefting of the upper lip musculature. Incomplete cleft lip involves skin, muscle, and mucosa but often spares the nasal sill and underlying skeletal structures. Complete unilateral cleft lip deformities involve all tissue layers.
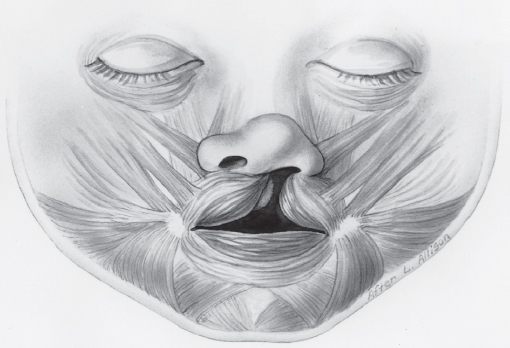
The orbicularis oris muscles associated with the unilateral cleft lip deformity are hypoplastic and incompletely developed when compared with their noncleft counterparts. In addition, the upper lip muscles are prevented from attaching to their normal insertions, finding unnatural insertions instead ( Fig. 68.21 ). Although it is obvious that no muscle crosses the cleft in complete clefts, the skin bridge in incomplete clefts has also been found to contain no functional musculature. Muscle dissections by Fara et al on stillborn babies with incomplete clefts confirmed that the muscles in unilateral cleft lips are more hypoplastic on the medial side of the cleft than the lateral side. 23 Additionally, these dissections revealed that the upper lip muscles in incomplete clefts did not cross the cleft gap unless the skin bridge was at least one-third the height of the lip. Even if the orbicularis oris muscle is present in the skin bridge of an incomplete cleft; however, the orientation of the fibers is abnormal.
The major vascular supply to the lips and nose arises from the facial artery, the fourth branch of the external carotid artery. The facial artery gives rise to the superior and inferior labial arteries at each oral commissure. The paired superior labial arteries anastomose in the midline of the upper lip, and the two inferior labial arteries behave similarly in the lower lip. In the unilateral cleft lip, the aberrant vascular supply parallels the findings of the unilateral cleft lip musculature ( Fig. 68.22 ). As with the orbicularis oris, the blood supply on the lateral aspect of the cleft is better developed than the vasculature on the medial side. The superior labial artery courses along the margin of the cleft, anastomosing with either the angular artery or the lateral nasal artery at the base of the nose. In incomplete clefts, a thin, terminal branch of the superior labial artery commonly crosses the skin bridge.
Surgical Repair
Many techniques have been described over the years for repair of the unilateral cleft lip. Early descriptions of cleft lip repair utilized variations of straight-line closures. The main disadvantage of straight-line closure is the tendency for vertical scar contracture across the mucocutaneous junction, resulting in notching of the lip. Wide complete unilateral cleft lips are also difficult to repair by the straight-line method.
In the mid-20th century, various geometric closures were proposed for repairing the unilateral cleft lip. Geometrical techniques, such as modified Z-plasties, quadrangular flaps, and triangular flaps, were designed to decrease the amount of lip shortening that occurred with cleft lip repair and to improve orbicularis oris realignment and function. 24 , 25 , 26 , 27 LeMesurier described the quadrangular flap and Tennison described the triangular flap as reliable methods for decreasing vertical lip contracture in unilateral cleft lip repair. 24 , 28
The primary advantage of geometric repair techniques for cleft lip is that they provide a reproducible method of lip repair. Exact measurements can be taken with calipers to assure a tensionfree closure of the lip. The basic disadvantage of these methods is that the incisions always violate the philtral column on the noncleft side, thereby creating a scar that does not respect boundaries of known anatomical subunits. In addition, geometric repairs require exacting presurgical measurement and often lack flexibility during surgical application.
In 1957, Ralph Millard incorporated aspects of multiple previously described repairs, and developed the rotation advancement flap for repair of the unilateral cleft lip. 29 This method maximized surgical flexibility while facilitating elimination of a minimal amount of normal lip tissue. This method is now the most commonly utilized technique for repair of the unilateral cleft lip. The advantages and disadvantages of the Millard rotationadvancement flap technique are shown in Table 68.2 .
Advantages | Disadvantages |
Flexible | Requires experienced surgeon |
Minimal tissue discarded | Possible excessive tension |
Good nasal access | Extensive undermining required |
Camouflaged suture line | Vertical scar contracture |
| Tendency to small nostril |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


