66 Craniomaxillofacial Deformities
Introduction
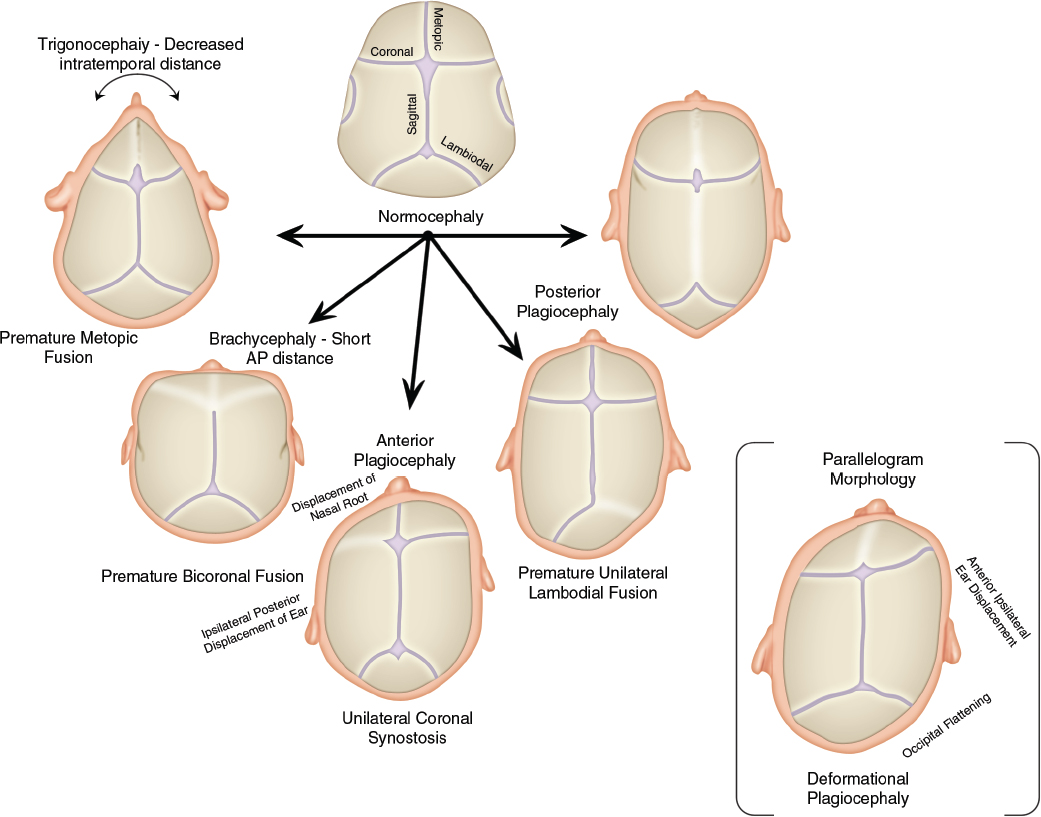
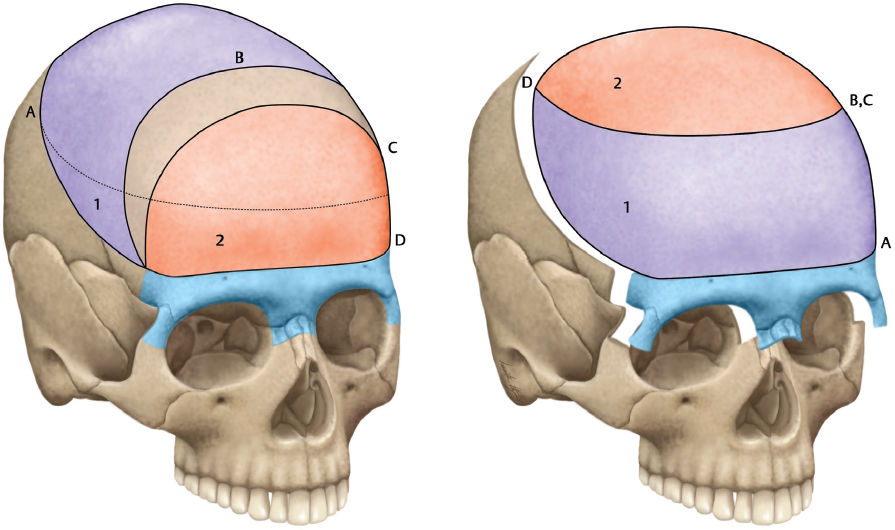
Craniomaxillofacial deformities present a range of abnormalities based on congenital conditions, trauma, and tumors. This chapter concentrates on congenital deformities, which present as a continuum from nonsynostotic deformations (posterior plagiocephaly), to single-suture synostosis, to multiple-suture craniosynostosis (craniofacial dysostosis) ( Fig. 66.1 and Table 66.1 ). Treatment of the craniosynostoses extends from conservative to multiple complex reconstructions, which may require many years; the central most basic advancement is the fronto-orbital advancement and frontal bone remodeling ( Fig. 66.2 ).
The authors advocate a team approach to the management of pediatric patients. Brain development, vision, sinuses, and airways must be considered. 1 , 2 The craniomaxillofacial team evaluates midfacial growth in childhood and adolescence, as well as occlusion and mastication in the primary mixed and permanent dentition phase. 3 , 4 A typical evaluation includes pediatric neurology, radiology, neurosurgery, anesthesiology, ophthalmology, genetics, and orthodontics. The management of patients is diverse and requires a longterm plan for followup. 5 Information about the genes and mutations underlying syndromes affecting craniofacial bones is accumulating rapidly, and surgical outcomes have been associated with specific mutations. 6 , 7 Genetics undoubtedly will play a growing role in deciding surgical strategies and family counseling. 8 , 9 In particular, coronal synostosis is frequently associated with known genetic mutations, and genetic screening will play an ever-larger role in the diagnosis of syndromic sysnostosis. The demand for outcome-based studies and evidencebased medicine has also accelerated the team management approach. Surgical procedures frequently involved extensive scalp dissection and bone osteotomies in children with low blood volumes. Advances in anesthesiology and hemostasis have significantly reduced morbidity. 10 , 11 The use of central venous catheters, arterial lines, and transthoracic Doppler have assisted in intraoperative resuscitation and decreased mortality secondary to blood loss and air embolism. In our center, we use a combination of 1:1 or 1:2 packed red blood cells with fresh frozen plasma transfused through a fluid warmer, providing colloid resuscitation matched to losses and subsequently limiting postoperative third space complications associated with crystalloid resuscitation. Nonetheless, measurement of intraoperative blood loss and resuscitation strategies remain an active area of investigation as blood loss from intracranial procedures remains the source of significant morbidity. 12
Advances in distraction osteogenesis, endoscopic surgical techniques, and the technology of absorbable plates and screws continue to change surgical options. 13 , 14 Craniomaxillofacial surgery in pediatric patients focuses on syndromic and nonsyndromic craniosynostosis, craniofacial tumors, trauma, and aesthetics. 15 , 16 , 17 The present chapter discusses indications, methods, and outcomes for craniosynostosis surgery.
Overview of Craniosynostosis
Craniosynostosis or premature fusion of the coronal, sagittal, metopic, or lambdoidal sutures ( Fig. 66.1 ) may be primary or secondary to known teratogens, metabolic disorders, hematologic disorders, or malformations such as microcephaly. 18 Craniosynostosis can also be found when patients are overshunted and sutures subsequently override and fuse. 19 , 20 The condition may be “isolated,” involving a single suture, or “complex,” involving multiple sutures. 17 , 21 Approximately 100 different forms have been described. Pathophysiology may be heterogeneous because phenotypes do not always associate with specific mutations. 21 , 22 Phenotypes have been classified as nonsyndromic and syndromic; the latter have been linked to several chromosomes. 18 , 23 For patients to carry a diagnosis of syndromic craniosynostosis, they must present with additional anomalies that exist in an embryologically distinct location from the craniofacial skeleton.
Most cases of craniosynostosis are single suture nonsyndromic patients. The developing calvarial ossifies in an intramembranous pattern whereby bone develops directly from mesenchymal precursor cells in a perpendicular direction from the cranial sutures. A complex interplay exists between the developing brain, dura, and pericranium that coordinates ossification. The dura maintains a strong osteogenic potential until early childhood. 24 Diagnosis of cranial suture synostosis is based on the knowledge of perpendicular growth from the suture. Once a suture is fused, growth will be restricted around the suture in a perpendicular fashion with compensatory changes along the open sutures; this results in welldefined cranial morphologies ( Fig. 66.1 ).
The common syndromic synostoses involve fibroblast growth factor receptor (FGFR) and transforming growth factor receptor activities. 25 , 26 , 27 , 28 Deletions in the TWIST gene have been detected in Saethre-Chotzen patients. 29 Because the same receptor can be involved in different “named” syndromes (e.g., Crouzon or Pfeiffer syndrome), it seems likely that syndrome eponyms will be replaced by designating the specific gene mutation. 30 Additionally, the degree of penetrance in these disorders is variable. No genetic difference may be seen between two syndromic patients with widely differing degrees of severity of craniofacial dysmorphology. 31
The most commonly encountered syndromic cases involving FGFR signaling are Aperts, Crouzon, Muenke, and Pfeiffer syndromes. Most often, they will present with bicoronal sysnostosis and midfacial retrusion. These mutations are most commonly gain-of-function mutations and are inherited in an autosomal dominant pattern. 32 Normal cranial ossification develops through intramembranous ossification; FGFR-1, -2, and -3 signaling modulate osteoblast activity in both enchondral and intramembranous bone ossification. 33 These receptors contain three major immunoglobulin-like regions with variable binding affinity for 22 known fibroblast growth factor ligands. 32 Activation and homodimerization of receptors facilitates downstream signaling via the MAP/ERK and PI3K/AKT signaling cascades. 33 Mutations in FGFR genes account for Apert, Crouzon, Pfeiffer, and Muenke syndromes, among others. 34 In these patients, the oversignaling of the fibroblast growth factor pathway is thought to result in premature fusion of the coronal suture; however, the mechanism is still poorly understood.
Two other significant protein mutations that also result in syndromic synostosis cases are MSX and TWIST. The MSX mutation is gain-of-function mutation in the muscle segment homobox 2 (MSX2) that accounts for Boston-type craniosynostosis, 35 which has been identified in one cohort in the Boston, Massachusetts, area. 32 Expression and suture involvement is variable (much like Pfeiffer syndrome), accounting for variable phenotypes, from fronto-orbital recession to cloverleaf skull deformities. 36 The TWIST1 mutation is notable for being the only known lossof-function mutation in syndromic synostosis cases. Currently there are 100 known mutations of the helix-loop-helix transcription factor TWIST1 (missense, nonsense, deletions, and duplications), accounting for Sathere-Chotzen syndrome. 33
Morphologic studies are beginning to unravel the complex relations between intracranial pressure (ICP), skull shape, and skull volume. It has been postulated that a cranial base malformation was the primary anomaly. More recent studies lend support to the idea that the proximal cause is the premature closure of the cranial sutures; however, the underlying dura also plays a significant role. 37 , 38 The brain-dural interaction with ossification of the developing calvarium is an important area of emerging research in the pathophysiology of suture synostosis. Computer-assisted morphologic analyses have advanced the understanding of normal and abnormal growth. There are questions about intracranial volumes in patients with metopic craniosynostosis. 39 , 40 Many authors have concluded that intracranial volumes are normal in most forms of craniosynostosis and may be larger than normal in Apert syndrome. 41
M. Michael Cohen has reviewed the epidemiology and pathophysiology of the craniosynostoses. 18 Briefly, incidence data are difficult to measure because the conditions are not often lethal and are not always recognized in newborns, or recorded in adults. Investigators have estimated 0.2 to 0.5 cases per 1,000 births. 42 , 43 Such studies noted that rates appeared to be increasing, and suggested that the increase was due to enhanced awareness of the condition and improved diagnostic imaging technology. In the 1980s, a subset of the craniosynostoses, unilambdoidal synostosis, attracted particular interest because reports indicated a significant increase in the incidence, which generally had been considered to be about 1% of the craniosynostoses cases. Pediatric neurosurgeons observed that lambdoidal craniosynostosis and positional plagiocephaly (sometimes referred to as “occipital plagiocephaly” and “functional plagiocephaly”) had similar morphologic characteristics. 44 The suspected increase in lambdoidal synostosis was, in fact, an increase in positional plagiocephaly, an increase related to the American Academy of Pediatrics recommendation (in 1992) that healthy infants avoid the prone sleeping position. Asymmetric skull flattening tends to be perpetuated or accentuated by supine positioning of the infant; the head will turn to the flatter side by forces of gravity when any degree of torticollis exists. The majority of single suture nonsyndromic cases present as sagittal suture synostosis.
It is important to differentiate positional plagiocephaly from craniosynostosis. The majority of infants may be diagnosed by careful exam and do not require imaging studies for the diagnosis. Positional plagiocephaly has been dramatically on the rise since recommendations issued by the American Academy of Pediatrics for infants to be placed on their backs to sleep. 45 Infants with positional plagiocephaly present with a “parallelogram” configuration from the vertex view. The occiput is flat from sleeping chronically on one side with anterior displacement of the ipsilateral ear. Often the contralateral forehead is retruded and the ipsilateral forehead is anteriorly displaced giving the parallelogram shape. Positional plagiocephaly may be treated by conservative measures including change of sleeping position and in more severe cases helmet therapy. Ideally children are treated with helmet therapy before 32 weeks of age but improvement in shape has been documented in infants up to 12 months of age. 46
Diagnosis
Pediatricians and family practitioners often request neurosurgical consultation for infants with abnormal head circumference in relation to standard growth curves, yet who are otherwise normal in growth and development. Prenatal diagnosis has relied on the family’s genetic information and fetal deoxyribonucleic acid analyses. Prenatal ultrasound measurements may play a role in confirming suspected cases. 47 Anomalies are frequently noted at birth; parents report a progressive worsening of the deformity and routinely express a concern about potential developmental problems. 48 The infants are usually seen by the age of 6 months. Preterm birth, which is associated with reduction in brain volume and poor cognitive outcomes, would signal a more frequent monitoring program. 49
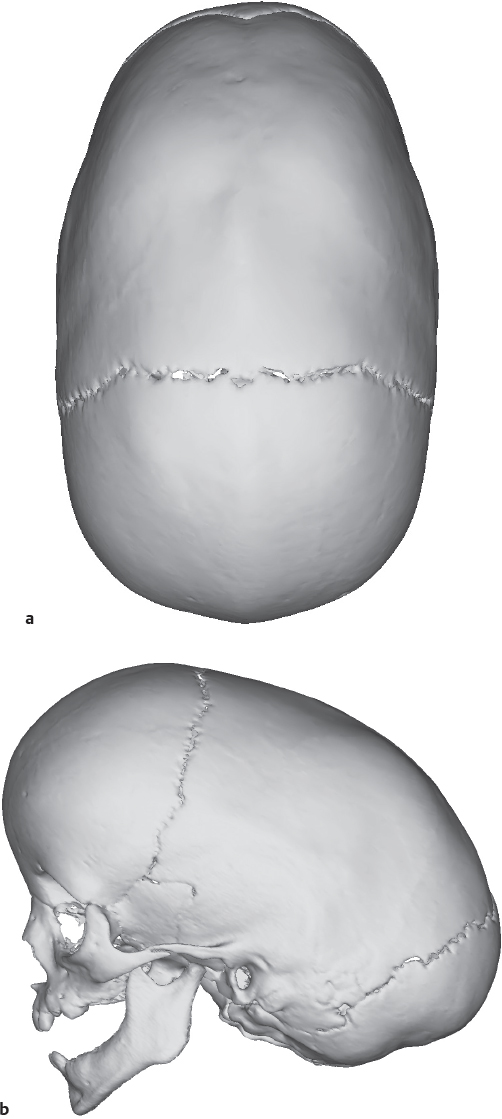
The evaluation of full-term infants with potentially misshapen heads is straightforward. 50 A long, narrow, boat-shaped head termed scaphocephaly indicates sagittal synostosis ( Fig. 66.3 ). The cephalic index is a common measure of the degree of severity in scaphocephaly. The normal cephalic index is ∼80, as measured by the cranial width over the cranial length multiplied by 100. Indexes under 71 are indicative of scaphocephaly. A top view of the typical distortion of sagittal synostosis is shown in Fig. 66.5a .
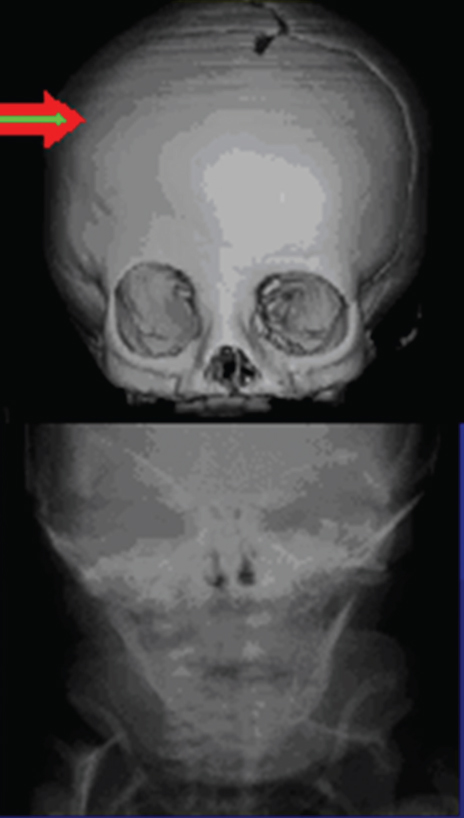
Unilateral and bilateral coronal synostoses are recognized by their forehead deformities ( Fig. 66.4 ). These are termed the anterior plagiocephalies. Bilateral coronal sysnostosis cases present with a symmetric short and tall skull termed turribrachycephaly. Cranial index in these patients will be elevated >82 to 85; patients with an index greater than 85 have severe brachycephaly. Unilateral coronal sysnostosis cases are often the most difficult to treat and present with varying degrees of frontofacial dysmorphology including an ipsilateral retruded brow and raised eyebrow. Growth arrest along the squamosal suture line resulting in the characteristic radiograph finding of a harlequin deformity is diagnostic. Often the contralateral forehead will be significantly bossed, accentuating the frontofacial asymmetry.
Metopic synostosis presents with the characteristic trigonocephaly shaped forehead. Examination reveals a prominent metopic suture with narrowing and elongation of the skull in the posterior direction. The forehead may be noted to be “keel” shaped, and the bitemporal distance in these patients is decreased; in severe cases, the patient may be hypoteloric ( Fig. 66.6 ).
Lambdoidal suture synostosis comprises the lowest frequency of synostosis cases. These are termed posterior plagiocephaly and are notable for occipital flatness along the effected suture with a mastoid bulge in addition to a posterior and inferiorly displaced ipsilateral ear. The ear position helps to differentiate posterior plagiocephaly from deformational or positional plagiocephaly.
The large majority of misshapen heads seen in primary care relate to positional plagiocephaly. These anomalies are usually mild and noticed at birth or soon thereafter. Anatomically, the occipital region in positional plagiocephaly is flattened with anterior compensatory changes and asymmetry in the ear position. Contralateral anterior flattening and unilateral anterior bossing are generally mild. Unilateral cases have compensatory growth in the contralateral parieto-occipital region manifested by bossing and vertex elongation. This elongation is more prominent in bilateral deformities, which also have lateral parietal widening, occipital flattening with anterior narrowing, and increased frontal projection. Infants may sleep on their backs and have slight flattening of the occipital region. These problems generally correct themselves as the infant grows and begins to roll over. Sometimes assistive devices are useful. 51 Differential diagnoses include torticollis, positional molding, and craniosynostosis. Positional molding may have a clinical manifestation similar to an actual craniosynostosis, but the sutures appear open on plain X-rays and computed tomographic (CT) scans in the functional case. Torticollis involves a shortened sternocleidomastoid muscle, which can result in flattening of the temporal and occipital region. The anterior deformity is typically greater than the posterior deformity and is on the side of the abnormality. The usually mild deformity improves with neck exercises and physical therapy. The muscle rarely needs to be divided or lengthened. Similar shaping can be seen in newborns with substantial developmental delays and in infants with torticollis, as well as with hypotonic infants who do not move their head. Table 66.2 briefly outlines the differential diagnosis between lambdoidal synostosis and patients with posterior plagiocephaly.
Radiologic Studies
Radiologic studies are seldom needed for initial diagnosis of cranial deformities, 52 , 53 although imaging technology plays a key role in treatment decisions and preoperative planning. CT imaging and threedimensional reconstruction provide detailed information about the cranial anatomy and sutures that cannot be obtained with routine radiographs. Preoperative modeling based off of CT imaging will play an ever-increasing role in the treatment of congenital craniofacial anomalies. Computerguided planning has the potential for reduced operative times and more precise reconstructions based off of cephalometric norms. Plain films have little role in the treatment and diagnosis of children with craniosynostosis. Also, CT imaging is not without its own risks; while protocols are still being perfected to reduce radiation exposure, every effort should be made to limit the number of imaging studies. Frequently, a single threedimensional CT within a month of a reconstructive operation is recommended. If imaging studies are preformed too early during this period of significant calvarial growth, the imaging study will lose its utility as a preoperative guide. Less invasive interventions, such as endoscopic craniectomies and suturectomies, may be performed without preoperative CT scans.
The CT evaluation reveals the amount of asymmetry of the skull and the compensatory changes that have occurred; in addition, it allows for identification of the venous sinuses. 54 , 55 The largest risk factor in these operations is blood loss and a clear knowledge of the position of the torcula helps prevent inadvertent injury in low posterior remodeling procedures. The CT scan in occipital deformities may also indicate abnormalities of the brain and the bone. Infants with severe deformities typically show diminished posterior subarachnoid fluid similar to the changes seen with increased ICP, but on a more localized basis. This appears to extend into the ventricular system, resulting in ventricular effacement. Generalized subarachnoid space dilation per se anteriorly does not indicate neurologic impairment, for it frequently is found in posterior plagiocephaly with normal neurologic status. With severe compression, sometimes the ipsilateral perimesencephalic cistern is effaced also. The finding usually correlates with an irregular, patchy, diminished thickness of the occipital bone. The patchiness is greatest in bilateral cases and appears to be similar to the copper-beaten or thumbprinting appearance seen on plain radiographs. “Copper beating” may not be a good marker for raised ICP because it occurs late and is an inconsistent finding. 56
Indications for Treatment
Several management protocols have been proposed. However, it is important to recognize that protocols cannot be viewed as absolute. For example, the decision not to operate can change rapidly with new information. Several protocols have focused on radiologic descriptors of the skull. We believe that it is more important to focus on the brain and indications of its normal development than on the bone that surrounds it. When plagiocephaly is severe enough to produce marked cerebral compression as demonstrated by clinical signs and the condition is progressive or nonrelenting, it is unwise to base all decisions on whether sutures appear to be fused. Open sutures on CT do not guarantee normal sutures or normal function. Our experience suggests that children can have abnormal-appearing sutures with normal neurologic status and normal-appearing sutures with neurologic deficits or marked cerebral compression. In cases of plagiocephaly with only mild cerebral compression, we would not advocate surgical correction, whereas in other cases, where the suture abnormality is less clear but the brain is severely compressed, we would advocate surgical correction after failure of conservative management.
The majority of patients with posterior plagiocephaly can be managed conservatively. Parents are instructed to change the child’s position slightly during naps and sleeping. Many therapists know how to carve out a pillow of foam rubber, which redistributes the weight of the head and is comfortable for the child. The costs are minor and the results appear to be excellent. 51 Severe cases can be treated with helmeting.
Indications for treatment need to be considered by the craniomaxillofacial team for each case based on clinical signs, syndromic and genetic information, radiologic indicators, and whether the child is stable or developing symptoms. Term newborns with mild localized bone deformities may develop normally despite their misshapen bones and appearance. Absent complications, one may take a wait-and-see attitude. Any benefits of routine imaging must be balanced against the considerable time and resources associated with CT investigations, especially in children.
Hydrocephalus is not usually found in single-suture, mild, nonsyndromic craniosynostosis. 57 , 58 The latter is thought by some to be an aesthetic problem with infrequent consequences for brain function and development. Mental development, measured by intelligence quotient tests, in infants with nonsyndromic, single-suture craniosynostosis appears to be normal in the absence of increased ICP and other pathologies. 59 However, clinical impressions have associated appearance with the adolescent’s ability to socialize, school performance, and adult behavioral problems. 60 , 61 Postoperative developmental attainment scales improved in a group of 28 infants (mean age of 8 months) with sagittal synostosis who had significantly poorer gross locomotor function compared with normal controls. 62 Yet most available testing methodologies have detected little significant evidence associating surgical intervention in single-suture isolated craniosynostosis and ultimate intellectual outcome. 63 , 64 In this regard, it is of interest to note the anthropologic studies of the many civilizations that practiced cranial deformation for appearance and political gains. 65 , 66 Such practices imply that an abnormal skull shape does not interfere with normal intelligence, although one cannot conclude that the physiologic results of congenital and cosmetic deformations are the same.
Apparently well-tolerated craniosynostosis can abruptly worsen either spontaneously or following head injury. Craniosynostosis by definition may result in progressive deformities due to limitations of the growth of the skull perpendicular to the involved suture. 67 Multiple suture synostosis and syndromic synostoses frequently associate with increased ICP, hydrocephalus, and visual impairment. 57 , 68 , 69 Multifactorial mechanisms underlie elevated ICP, including skull morphology and venous outflow obstruction. 70 , 71 The effects of craniosynostosis on the brain are not localized to structures immediately adjacent to the suture or to the endocranial surface of the skull. Visual loss can develop suddenly without other symptoms of ICP. 72 The actual size or changes in the size of the ventricles are not reliable predictors of ICP or changes in ICP. 73 Finally, severe cosmetic factors are in their own right a valid indication for surgery, especially as the intraoperative risks decrease with improved techniques and the increasing availability of biodegradable surgical tools.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


