63 Frontal Sinus and Naso-Orbito-Ethmoid Fractures
Introduction
The frontal bone is thick and very resistant to trauma. Consequently, the majority of injuries involving the frontal sinus and nasoorbitoethmoid complex are the result of high-velocity impacts such as motor vehicle accidents, assaults, and sports injuries. While the treatment of frontal sinus and naso- orbitalethmoid fractures is distinct, the anatomical proximity of these two areas warrants a combined discussion. The initial evaluation of such high-velocity injuries should focus on airway maintenance and hemodynamic stability. Once the patient is stabilized, the brain, spine, orbits, and facial skeleton should be evaluated. This often requires a team approach involving the facial plastic surgeon, neurosurgeon, and ophthalmologist. While the anatomy and mechanism of injury have been well studied, the treatment of these injuries remains controversial. Improper management can result in aesthetic deformity, chronic sinusitis, pneumocephalus, mucopyocele, meningitis, and brain abscess—all of which generally occur years to decades after the injury. The goal of treatment is avoidance of short- and longterm complications as well as the return of normal sinus function and aesthetic facial contour. While there is a trend in the literature toward minimally invasive and endoscopic approaches, there are no prospective randomized studies comparing different treatment strategies. Surgeons must remain diligent with regard to patient education and longterm followup. A treatment algorithm for frontal sinus and nasoorbitoethmoid complex injuries will be presented.
Frontal Sinus Fractures
Embryology and Anatomy
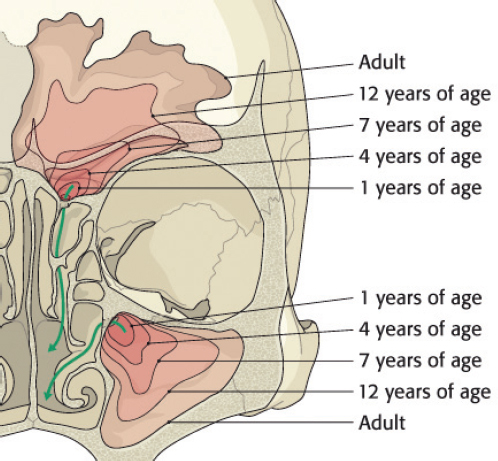
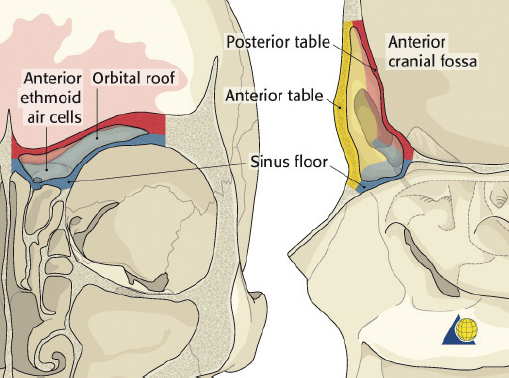
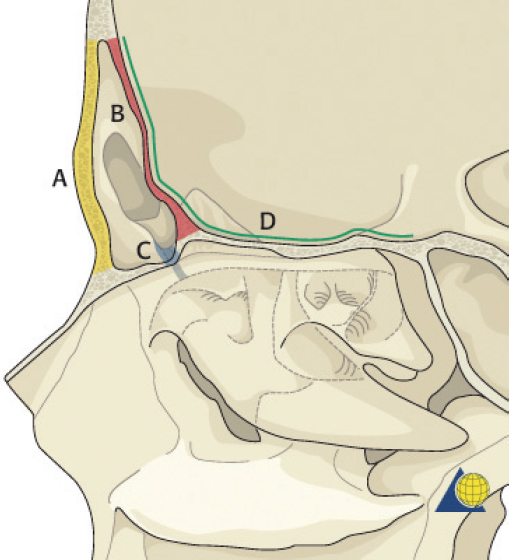
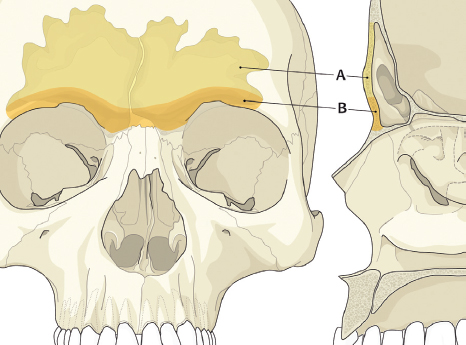
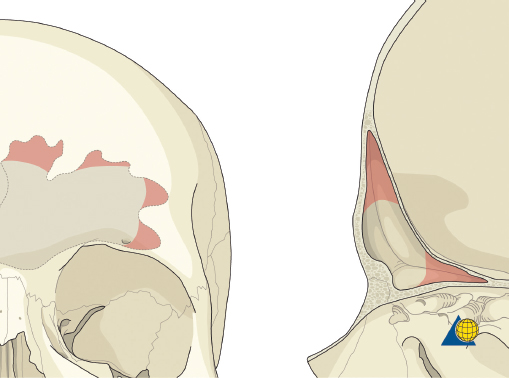
The frontal sinus is absent at birth. At approximately 1–2 years of age, the anterior ethmoid air cells invade the frontal bone to form a rudimentary cavity. By 7 years of age, the frontal sinus can be detected radiographically. The frontal sinus is adult size by approximately 15 years of age ( Fig. 63.1 ). The floor of the sinus forms the medial portion of the orbital roof. The posterior table forms a portion of the anterior cranial fossa. The anterior table forms part of the forehead, brow, and glabella ( Fig. 63.2 ). The frontal sinus is most commonly bilateral, asymmetric in shape, and divided by one or more intersinus septations. The size and shape of the adult frontal sinus are highly variable, with 10% of individuals having a unilateral sinus, 5% having a rudimentary cavity, and 4% having no sinus at all. The average dimensions are: height 30 mm, width 25 mm, depth 19 mm, and volume 10 mL. The anterior table thickness may be as great as 12 mm (average 4 mm), whereas the posterior table ranges in thickness from 0.1 to 4.8 mm. 1
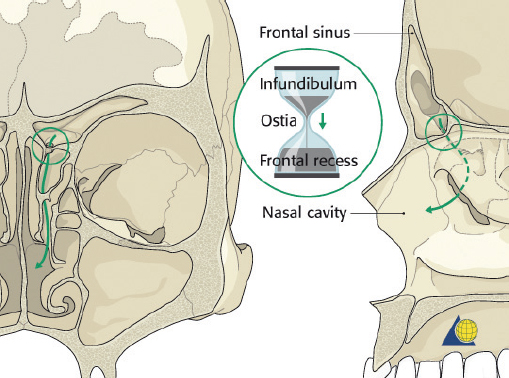
The nasofrontal recess is the sole outflow tract for the frontal sinus. The distance from the frontal sinus to the hiatus semilunaris is usually very short and is therefore most accurately described as a “recess” rather than a true duct. Each ostium is 1–3 mm in diameter and located on the posterior, inferior aspect of the sinus floor. The ostium lies anterior to the anterior ethmoid air cells, medial to the orbit, lateral to the intersinus septum, and posterior to the frontal bone. The true ostium represents the narrowest point of an hourglass configuration, with the frontal sinus infundibulum above and the nasofrontal recess below ( Fig. 63.3 ). 2 The vascular supply to the frontal sinus is from the supraorbital and supratrochlear arteries via the internal carotid system. Venous drainage occurs through three pathways: the facial vein, the ophthalmic vein (to the cavernous sinus), and the foramina of Breschet (to the subarachnoid space). 6 The ophthalmic branch of the trigeminal nerve provides sensory innervation to the frontal sinus.
Epidemiology
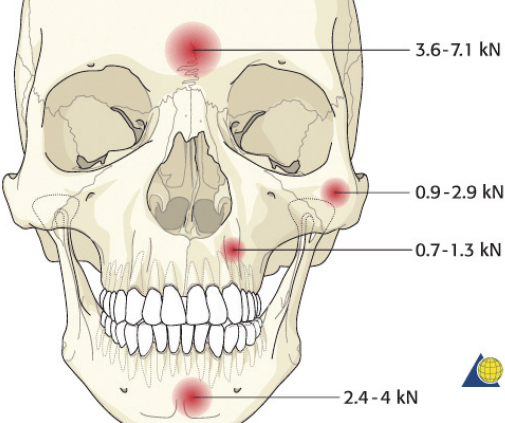
The frontal sinus is protected by thick cortical bone and is more resistant to fracture than any other facial bone ( Fig. 63.4 ). 3 Consequently, frontal sinus fractures account for only 5 to 15% of maxillofacial injuries and are most commonly associated with motor vehicles accidents, sporting events, and assaults. 4 The extreme force required to fracture the anterior table of the frontal sinus results in serious associated injuries in many patients. 5 Sixty-six percent of patients will have associated facial fractures. Isolated anterior table fractures occur 33% of the time. Combined fractures of the anterior table, posterior table, and/or the nasofrontal recess account for 67% of frontal sinus injuries. Isolated posterior table injuries occur but are very uncommon. 4
Diagnosis
The accurate diagnosis of frontal sinus fractures and nasofrontal recess injuries is crucial to appropriate treatment. After the patient has been stabilized, a thorough head and neck examination should be performed. Patients with frontal sinus fractures often complain of forehead pain and swelling. Other findings that may suggest a frontal sinus injury include supratrochlear and supraorbital paresthesias, epistaxis, forehead abrasions, lacerations, and hematoma. Through-andthrough injuries of the frontal sinus have high morbidity and prompt surgical treatment is indicated. If the patient is awake, he or she should be questioned regarding the presence of clear rhinorrhea or salty postnasal drainage. Drainage suspicious for cerebrospinal fluid (CSF) rhinorrhea can be grossly evaluated with a “halo test.” The bloody fluid is allowed to drip onto filter paper. If CSF is present, it will diffuse faster than blood and result in a clear halo around the blood. The definitive test for CSF is β-2 transferrin. The presence of β-2 transferrin is diagnostic of a skull base injury with CSF leak. The only other locations where β-2 transferrin is found are the vitreous humor of the eye and perilymph of the inner ear.
Radiological Evaluation
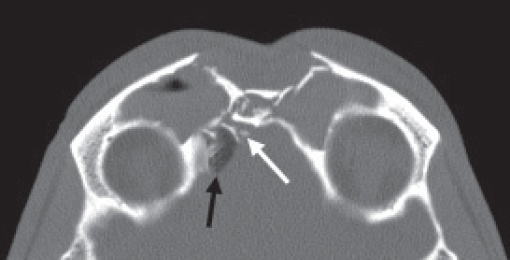
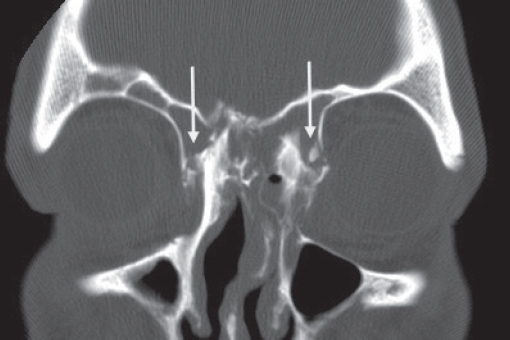
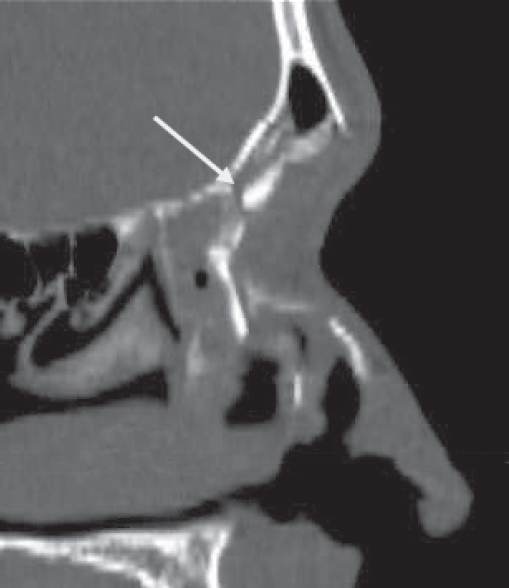
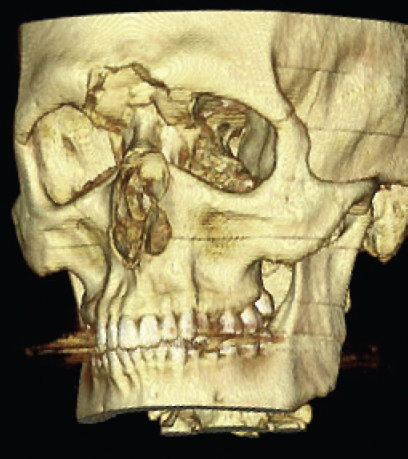
Historically, plain sinus X-rays were used to evaluate facial fractures. Thin cut (1–1.5 mm) axial computed tomography (CT) scans are now the gold standard for diagnosis of frontal sinus fractures. These images are readily reformatted into coronal, sagittal, and threedimensional (3D) reconstructions to improve the diagnostic accuracy. Axial cuts provide excellent information about the anterior and posterior table as well as pneumocephalus ( Fig. 63.5 ). Coronal reconstructions demonstrate the frontal sinus floor, orbital roof, and frontal recess ( Fig. 63.6 ). Sagittal views can assist with evaluation of frontal recess and skull base injuries ( Fig. 63.7 ). Threedimensional reconstructions can be very helpful in delineating the location of bone fragments and reducing the need for excessive dissection intraoperatively ( Fig. 63.8 ). Access to the PACS ( p icture a rchiving and c ommunication s ystem) or some type of presurgical planning software allows the surgeon to manipulate the reconstructions in space, gaining a greater understanding of depth and spatial relationships of the injury ( Video 63.1).
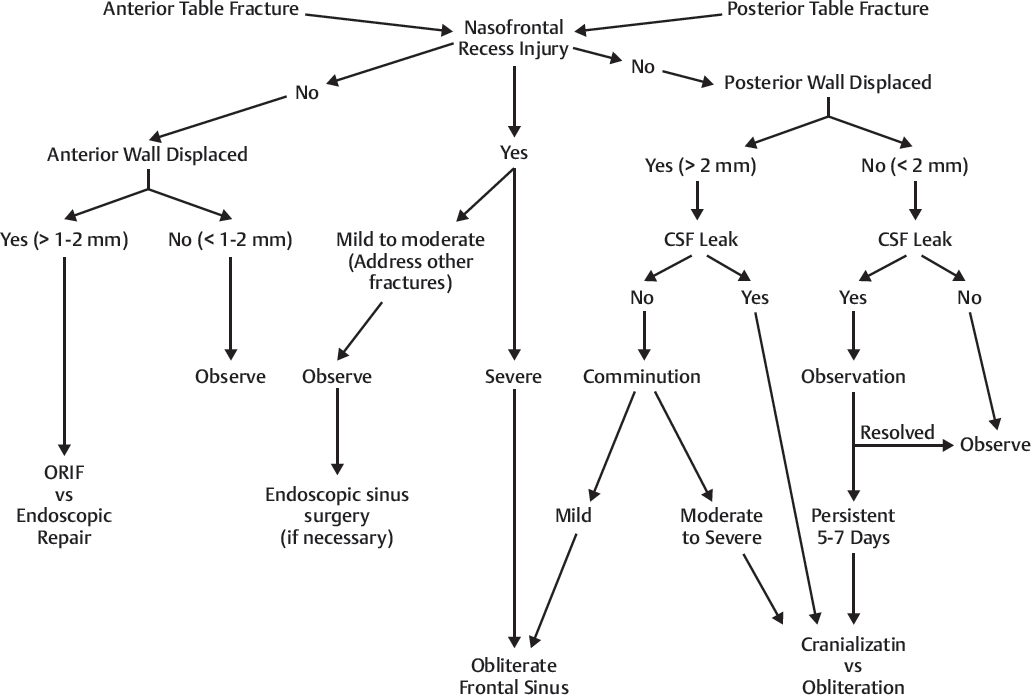
Treatment Algorithm (Fig. 63.10)
The treatment goals for frontal sinus fractures include (in decreasing order of importance) protection of intracranial contents, prevention of early and late complications, restoration of aesthetic forehead contour, and return of normal frontal sinus function. Accomplishing all of these goals is not always possible. However, reconstruction of a “safe” sinus is imperative. Once this has been accomplished, the aesthetic and functional repair can be addressed. The appropriate treatment strategy can be determined by assessing four anatomical parameters: (1) anterior table fracture, (2) posterior table fracture, (3) nasofrontal recess fracture, and (4) dural tear (CSF leak) ( Fig. 63.9 ); and applying them to the algorithm presented in Fig. 63.10 . Specific treatment options include observation, endoscopic fracture reduction or camouflage, open reduction and internal fixation, sinus obliteration, sinus exenteration (Riedel procedure), and sinus cranialization. The indications and techniques for each are discussed below.
Nasofrontal Recess Fractures (Fig. 63.10)
The compact structure of the nasofrontal recess makes accurate diagnosis of isolated fractures difficult. A thorough physical examination and a thin cut CT scan with 3D reconstructions should be critically reviewed. Radiographic findings that are most suggestive of a frontal recess injury include fractures involving the: floor of the frontal sinus, anterior ethmoid region, or gross disruption of the outflow tract. 9 , 10 , 11 In the absence of significant fracture displacement or associated frontal sinus injuries, there has been a trend toward a more conservative approach to these injuries. This would include close observation and a repeat CT scan 4 to 6 weeks after the injury. If the nasofrontal recess is found to be obstructed and the frontal sinus is opacified, surgical treatment is indicated (see below).
More recent literature has suggested that open reduction and internal fixation of frontal sinus fractures involving the frontal recess, followed by close postoperative observation, may be efficacious. 12 If outflow obstruction becomes apparent weeks to months after the injury, an endoscopic sinusotomy can be performed. The author has had some success with this technique, but there is limited longterm followup. This approach is still being investigated and should be reserved for surgeons with extensive experience with traditional open approaches to the frontal sinus as well as endoscopic frontal sinusotomy.
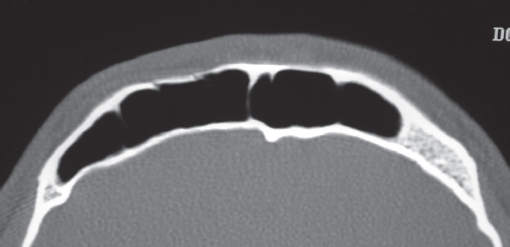
Anterior Table Fractures (Fig. 63.10)
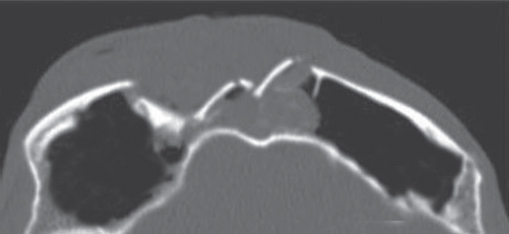
Isolated, minimally displaced (0–2 mm) fractures of the anterior table pose little risk for mucocele formation, and rarely result in aesthetic or functional deficit ( Fig. 63.11 ). The small risk of external deformity should be discussed with the patient; however, these injuries are best managed nonoperatively. Fractures with greater displacement (2–6 mm) present little risk of mucocele formation and often do well with no intervention ( Fig. 63.12 ). However the risk of aesthetic deformity likely increases as the degree of displacement increases. The decision for surgery in these patients should NOT be based on the risk of longterm functional sequelae. The decision for surgery should be carefully weighed against the risks of general anesthesia and iatrogenic sequelae (alopecia, paresthesias, facial nerve injury, etc.). Such sequelae can often be more significant than the injury itself. Minimally invasive approaches to fracture reduction have been described, accessing the frontal bone via an upper eyelid 13 , 14 or scalp incision. 15 , 16 , 17 These approaches are technically challenging and generally require significant expertise with endoscopic techniques. If an endoscopic approach is chosen, the author prefers a camouflage technique. 15 , 16 , 18 Endoscopic camouflage is performed 2–3 months after the injury when all facial swelling has resolved and the patient is able to assess if an aesthetic deformity actually exists. If the patient is seen acutely and an endoscopic camouflage repair is planned, the rational and indications for such an approach must be discussed (i.e., risk of iatrogenic injury may be greater than the traumatic deformity itself). The patient must also understand that the fracture cannot be reduced once it has healed. In the author’s experience, patients with mildly displaced fractures will often choose no further treatment for these injures because there is little if any external deformity. More complex fractures (> 6 mm displacement or with significant comminution) will require an open reduction using a coronal incision ( Fig. 63.13 ).

Posterior Table Fractures (Fig. 63.10)
Treatment of posterior table fractures is complex and controversial due to the risk of CSF leak, meningitis, brain injury, and late mucocele formation. 5 , 19 Some authors have supported exploration of nearly all posterior table fractures, while others recommend observation of even displaced posterior table injuries. This author believes the primary decision criteria for surgical intervention are the fracture severity (displacement/comminution) and the presence of a CSF leak.
Displacement ≤ 2 mm
Patient with ≤ 2 mm of displacement and no CSF leak can be observed. A repeat CT scans at 1 month and 1 year is indicated to rule out mucocele formation. The need for longterm followup should be emphasized with the patient, including the signs and symptoms of a mucocele. If a CSF leak is present upon presentation, observation is still indicated. Approximately 50% of these will resolve spontaneously. 20 If the leak persists, a sinusotomy, dural repair, and sinus obliteration are indicated.
Displacement. 2 mm
Patients with > 2 mm of displacement, no CSF leak, and minimal comminution should be considered for sinus obliteration. More severe injuries with a frank CSF leak and moderate to severe comminution will require a dural repair with removal of posterior table bone. If more than 25 to 30% of the posterior table bone is removed, a cranialization should be considered. Neurosurgical consultation should be obtained for assistance with brain debridement and dural closure.
Surgical Technique
Frontal Sinusotomy and Endoscopy
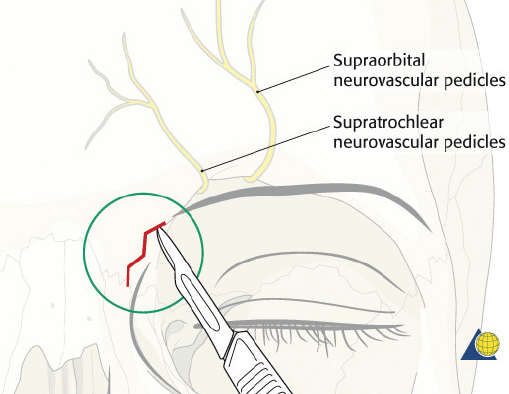
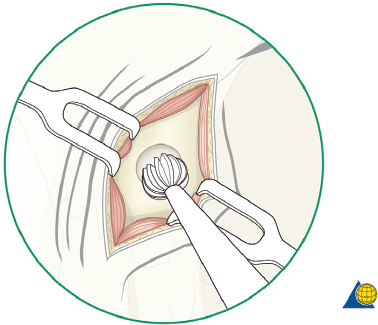
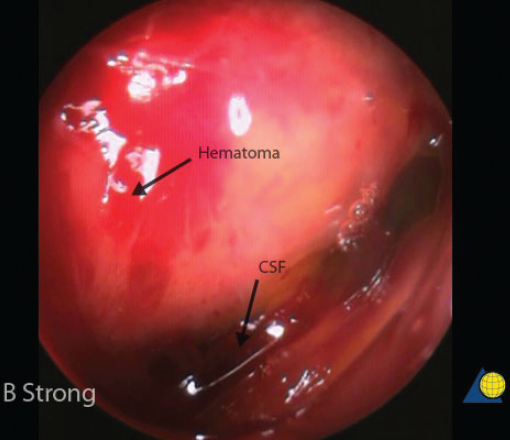
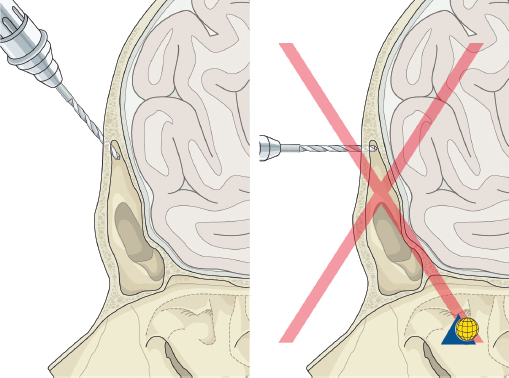
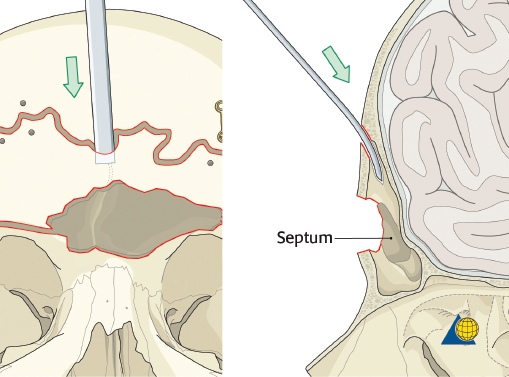
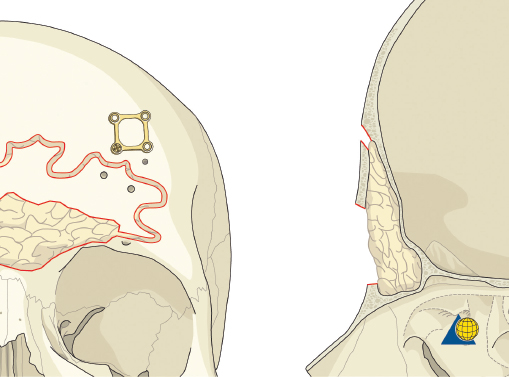
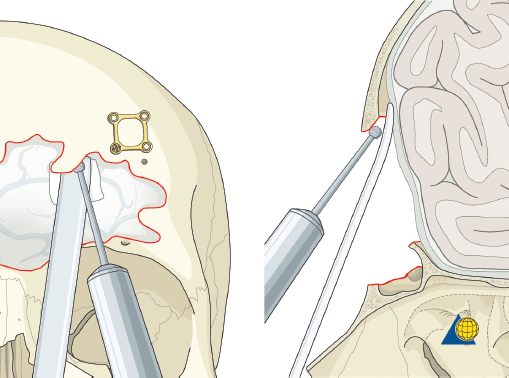
Endoscopic frontal sinusotomy can be used to visualize the posterior table and frontal recess for evidence of CSF leak. After appropriate consent is obtained for the procedure (including the risks of bleeding, infection, paresthesia, posterior table injury, and poor aesthetic result), local anesthesia is injected and a 1- to 1.5-cm skin incision is placed midway between the medial canthus and the glabella, and 1 cm inferior to the brow ( Fig. 63.14 ). The incision should not be placed within the eyebrow as this increases the risk of supratrochlear nerve injury and alopecia. The incision is best hidden by placing it medial and inferior to the curve of the brow. A scalpel is used to incise the skin, and a guarded needle point monopolar electrocautery is used to expose the periosteum. The location of the frontal sinus is confirmed on the CT scan or with intraoperative navigation. A small cutting bur is used to open a 4- to 5-mm frontal sinusotomy, 1 cm medial and inferior to the medial brow ( Fig. 63.15 ). The mucosa is incised sharply. Direct visualization of the posterior table and nasofrontal recess is performed with a 30-degree nasal endoscope ( Fig. 63.16 ). A flexible pediatric bronchoscope can be used to assess the lateral aspect of the sinus if necessary. A Valsalva maneuver can assist with the diagnosis of a CSF leak. The procedure is completed with a meticulous, layered closure. Trephination can be performed bilaterally if necessary.
Endoscopic Anterior Table Repair
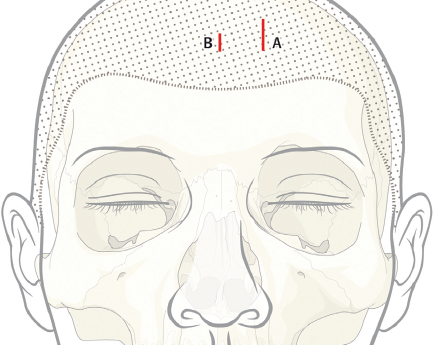
Appropriate consent should be obtained for the procedure including the risks of bleeding, infection, paresthesia, alopecia, poor aesthetic result, and possible need for open approach if an endoscopic repair cannot be performed. A 3- to 5-cm parasagittal “working” incision should be placed above the fracture, 3 cm behind the hair line ( Fig. 63.17 ). Care should be taken to minimize trauma to the hair follicles—avoiding electrocautery if possible. The incision length should be kept to a minimum, but will vary depending on the size of the fracture and implant to be inserted. A second 1- to 2-cm endoscope incision is then placed at the same height, 6 cm medial to the working incision. In patients with a prominent forehead or receding hair line, the incisions may need to be placed closer to the hairline, allowing visualization around the forehead curvature.
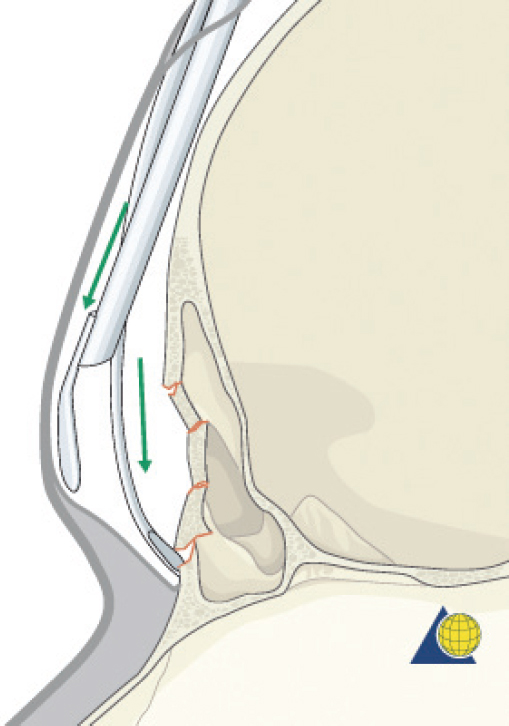
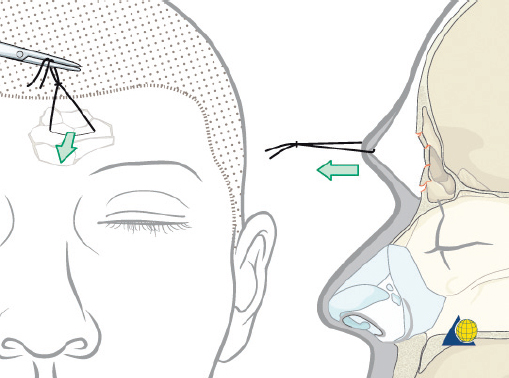
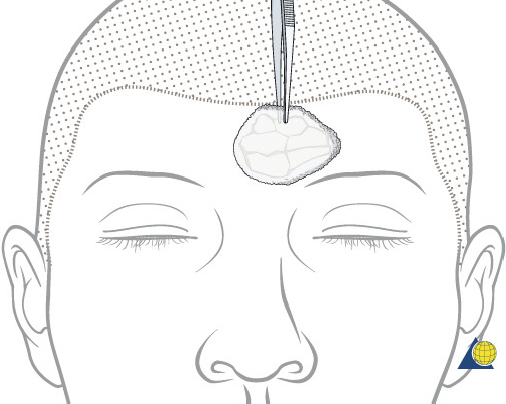
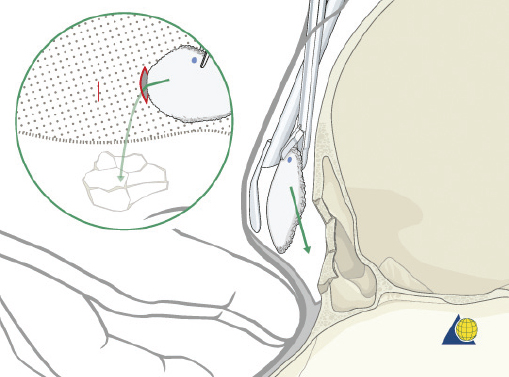
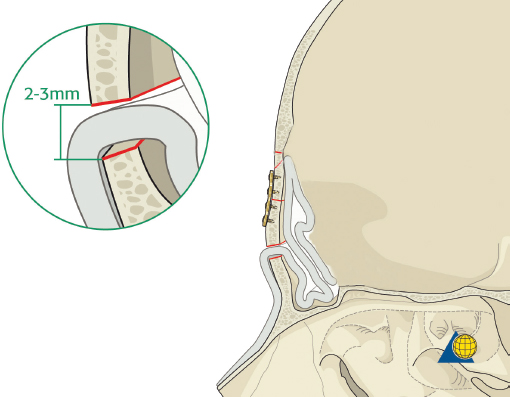
The surgical technique is similar to that of an endoscopic brow lift. 21 A “blind” subperiosteal dissection is performed down to the level of the fracture. Caution should be used to maintain the integrity of the periosteal envelope. Periosteal tears will catch the endoscope when it is inserted and make visualization more difficult. A 4-mm, 30-degree endoscope (with rigid endosheath and camera) is inserted to visualize the optical cavity. The periostoma is carefully elevated over the defect. The elevation is generally not difficult because the procedure is performed ≥ 3 months after the injury and there is a fibrous layer preventing entry into the sinus ( Fig. 63.18 ). An “0 silk” stitch can be placed full thickness through the forehead skin and used for retraction, maximizing the optical cavity ( Fig. 63.19 ). Once the entire fracture is exposed, a 0.85-mm thick porous polyethylene sheet (MEDPOR, Stryker) is trimmed to approximate the defect. The implant size can be estimated by using the forehead depression as a template ( Fig. 63.20 ). The superior edge of the implant is marked with a pen to maintain the orientation endoscopically. The implant is inserted through the working incision and manipulated over the defect ( Fig. 63.21 ). This process is repeated until the diameter of the implant is 2 to 3 mm larger than the defect. At times, the author has sutured two to three layers of MEDPOR together to more accurately fill deep defects. A 25-gauge needle is then passed through the skin over the fracture site and endoscopically visualized to determine the best site for percutaneous screw placement. A no. 11 blade is used to make a 2-mm, throughandthrough stab incision at the edge of the implant. A 1.7-mm self-drilling screw (length 4–7 mm) is passed through the stab incision, through the edge of the implant, and into the frontal bone ( Fig. 63.22 ). If the implant is not completely stable, a second screw is placed on the contralateral side. The self-drilling screw must be placed at least 0.5 to 1.0 mm away from the implant edge, or the implant may tear. The scalp incisions are then closed in layers and a head dressing is applied. Not all isolated anterior table fractures are appropriate for this technique. Injuries with severe comminution and marked mucosal injury may require open reduction or even frontal sinus obliteration. Fractures that extend over the orbital rim may be difficult or impossible to visualize endoscopically and may also require an open approach ( Fig. 63.23 ).
Open Reduction and Internal Fixation
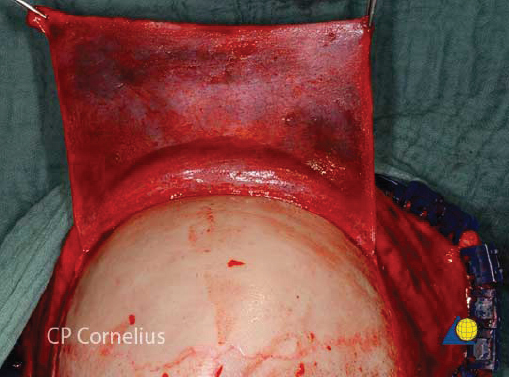
Anterior table fractures that cannot be observed or managed endoscopically will require open repair. Consent is obtained from the patient for the procedure including the risks of bleeding, infection, paraesthesia, CSF leak, meningitis, external deformity, and late mucocele formation. The coronal incision should be described, particularly in those patients with male pattern baldness. Once in the operating room, the bed is turned 180 degrees away from anesthesia. Corneal shields or tarsorrhaphies are placed. The hair need not be shaved. To be well hidden, any incision should start and end behind the ear and run across the scalp at least 3–4 cm behind the hair line. If the hair is long enough to part, a water-based lubricant is applied and the hair is banded in a zig-zag pattern ( Fig. 63.24 ). Postoperatively, gravity will pull the hair down over the transverse arms of the incision and provide some camouflage. If the patient wears their hair extremely short, the zig-zag incision has little advantage. A traditional coronal incision works equally well and is easier to perform ( Fig. 63.25 ). Brow incisions should be avoided due to the prominent scar and associated forehead anesthesia. If large forehead lacerations are already present, they should be explored and used to assist with fracture repair. However, such lacerations are often inadequate for complete fracture repair, and significant extension of forehead lacerations should generally be avoided.


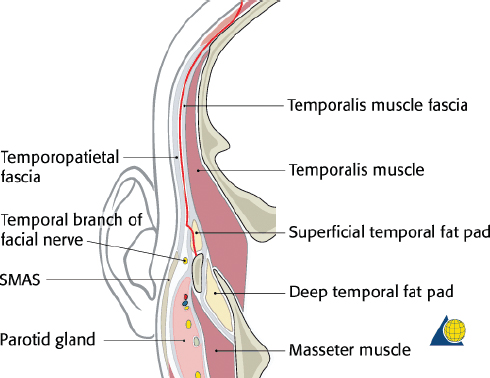
After injection of local anesthetic, the scalp is incised in thirds allowing for time to control bleeding. The central third (temporal line to temporal line) is incised down to the level of the galea aponeurosis. Larger vessels should be ligated with suture and the use of electrocautery minimized. Raney clips can be used depending on surgeon preference. If there is a need for a pericranial flap during the procedure, the pericranium is left intact on the calvaria. If no need is anticipated, the pericranium is incised and elevated with the scalp flap. Next the lateral thirds of the scalp are individually incised in a similar fashion. The lateral dissection must be meticulously performed between the temporoparietal fascia (superficial temporal fascia) and the temporalis muscle fascia (deep temporal fascia) ( Fig. 63.26 ). The temporoparietal fascia and frontal branch of the facial nerve are elevated with the flap.
If the pericranium has been elevated with the flap, the central dissection is carried forward to expose the fracture, taking care to protect the integrity of the bone fragments as much as possible. The incision can be easily extended behind the ear as necessary to facilitate rotation of the flap forward. Care is taken to avoid excessive traction or injury to the supratrochlear and supraorbital nerves. If complete exposure of the superior orbital rims is necessary, the supratrochlear neurovascular pedicle can be released using a small osteotome placed at the medial and lateral aspect of the foramina and out-fracturing the bone ( Fig. 63.27 ). This will allow for dissection along the orbital roof and greater exposure of the sinus floor.

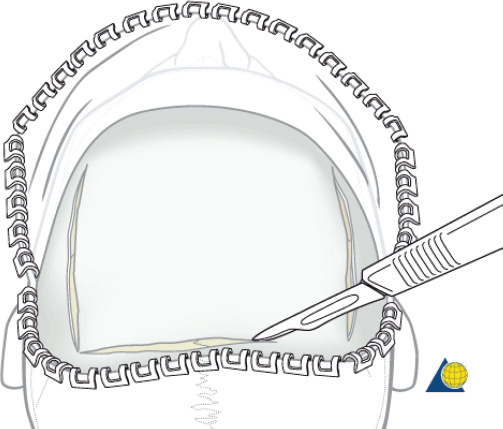
If the pericranium has been maintained on the calvaria for easier elevation and use during the procedure, the subgaleal dissection is stopped at the orbital rims. The periosteal flap is then incised at the level of the skin incision and continued laterally, 2 cm cephalad to each temporal line ( Fig. 63.28 ). As the periosteum is elevated off the bone, a careful inferior dissection over the fracture will protect the vascular supply from the supratrochlear arteries and produce a robust flap that can be used for external camouflage, sinus obliteration, or dural repairs ( Fig. 63.29 ).
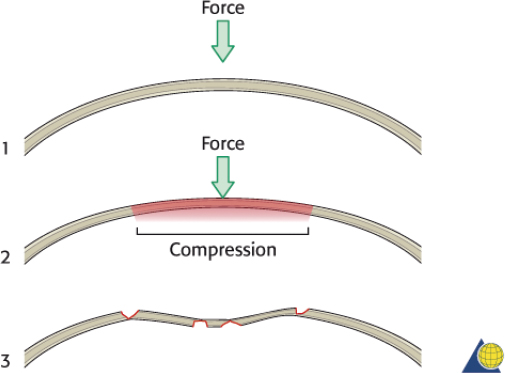
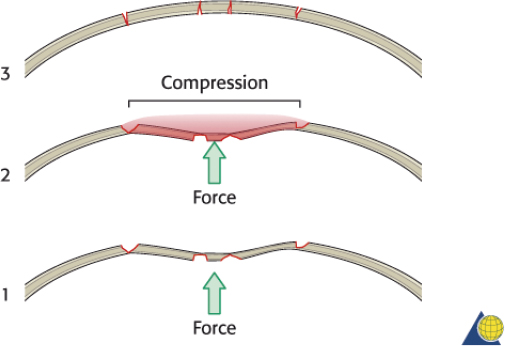
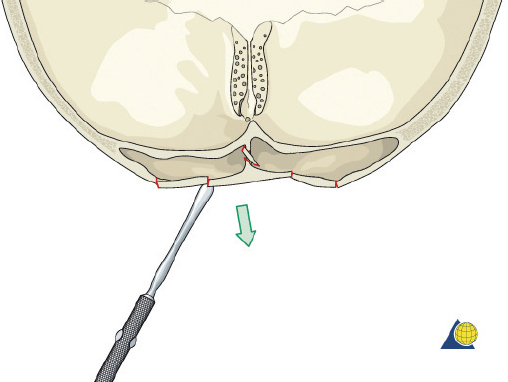
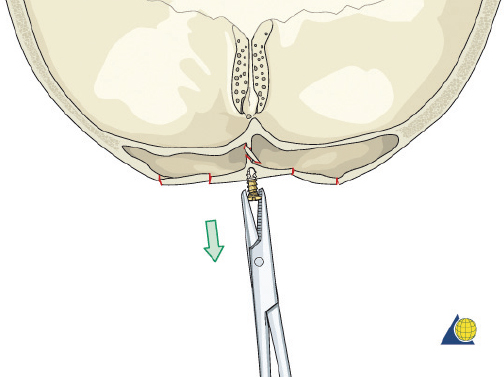
The frontal sinus contour has an intrinsic convex shape. As a perpendicular traumatic force is applied to the sinus, the convex shape is flattened. The bone is horizontally compressed until it fractures, and then it releases into a concave shape ( Fig. 63.30 ). Without significant comminution or bone displacement, fracture reduction will required enough force to pull the bone back through the compressive phase to its premorbid convex shape ( Fig. 63.31 ). While an attempt should be made to maintain the majority of fragments in situ, it may be necessary to remove a small bone fragment to release tension and allow fracture reduction. A bone hook or elevator can often be insinuated between the fragments to assist with elevation ( Fig. 63.32 ). If the bone fragments do not overlap, reduction can be accomplished by placing a 1.5- to 2-mm screw in the depressed segment, grasping the screw with a heavy hemostat, and pulling the segment anteriorly ( Fig. 63.33 ). After the bone fragments are mobilized, a 30-degree endoscope can be helpful to visualize the sinus mucosa and the nasofrontal recess. Any torn mucosa should be removed from fracture lines to avoid entrapment. The reduced fragments are then plated back in place with 1.0 to 1.3 microplates or micromesh.
While missing bone is uncommon, high-velocity injuries may result in tiny fragments that cannot be fixated. Small (4–10 mm) gaps can be reconstructed with titanium mesh. Hydroxyapatite cement should not be used as it has an unacceptably high risk of infection and extrusion. After the reconstruction is complete, the pericranium is reapproximated (if not used during the procedure), followed by the galea aponeurosis and skin. A tight galeal closure is important to obtain hemostasis and avoid hematoma. It is important to re-suspend the temporal soft tissues with 2-0 monofilament sutures, to avoid late ptosis of the forehead and upper midface ( Fig. 63.34 ). If necessary, bilateral Penrose drains are placed beneath the scalp, exiting the coronal incision above each ear, and sutured to the skin. A pressure dressing is applied. Care should be taken to ensure that the ears are not rolled forward under the pressure dressing. The Penrose drains are removed at 24 hours, the pressure dressing is discontinued at 3 days, and the skin sutures/staples are removed at 10 days.
Frontal Sinus Obliteration
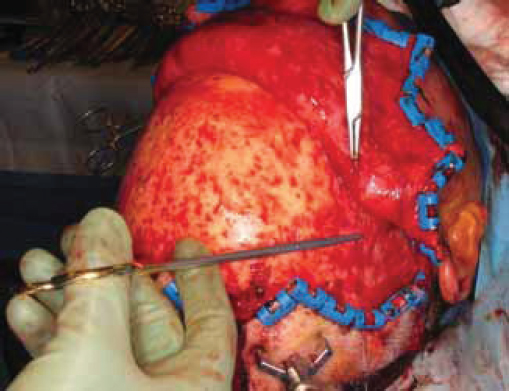
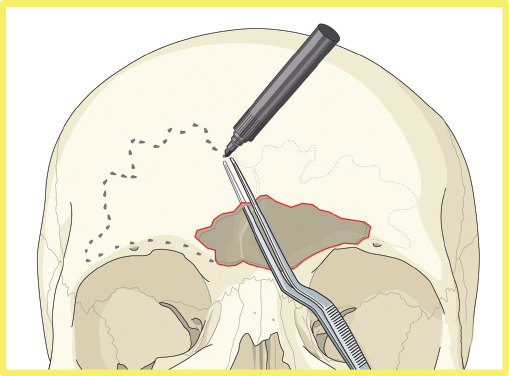
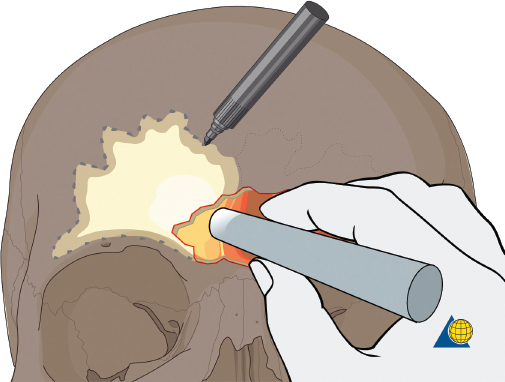
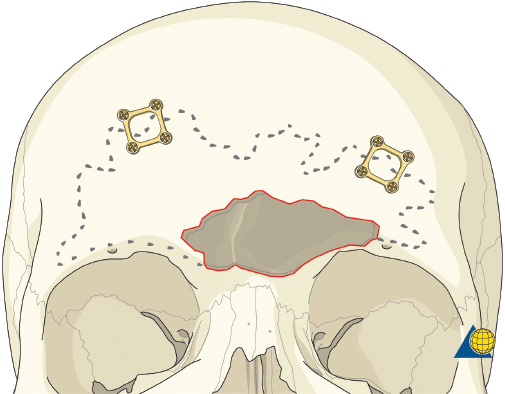
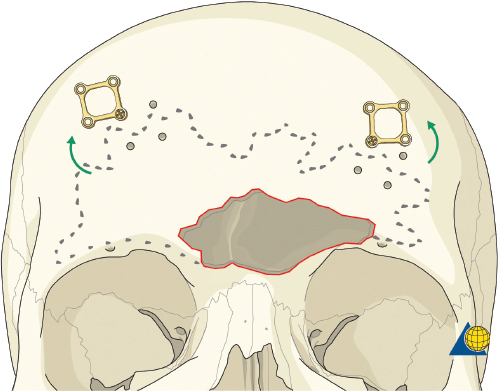
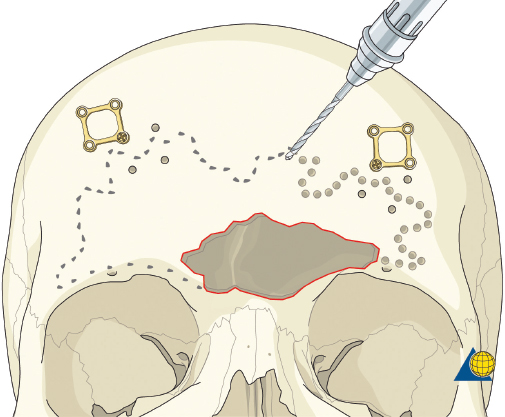
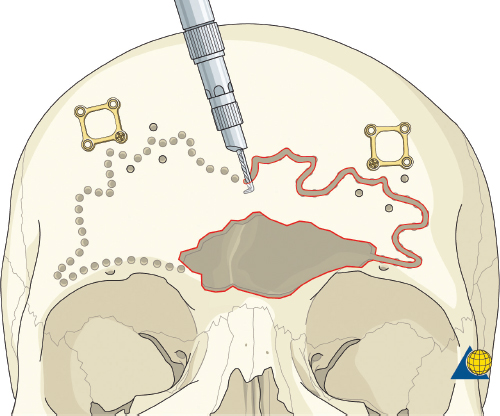
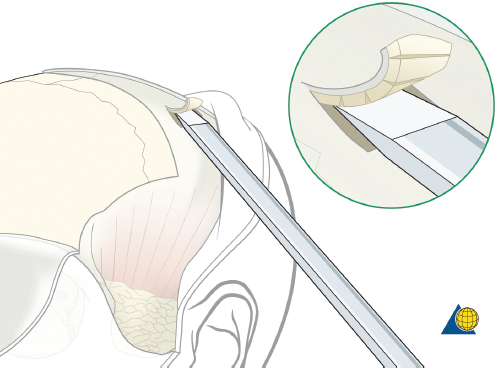
More severe injuries involving the anterior and/or posterior table(s) may require sinus obliteration. The exposure has been described above (open reduction and internal fixation). It is important to maintain a viable pericranial flap that can be used for dural repair if necessary. After complete exposure of the frontal bone (and orbital rims as necessary), all anterior table bone fragments should be carefully removed and kept moist on a side table. It is helpful to maintain the orientation of the fragments with a drawing to assist with re-orientation during the final repair ( Fig. 63.35 ). It is often necessary to complete the frontal sinusotomy, and remove any remaining anterior table bone to visualize the entire sinus. Intraoperative navigation can be useful to define the margins of the sinus. Alternatively, one tine of a bipolar cautery can be placed through a defect in the anterior table and walked around the periphery of the sinus. The outer tine is used to mark the outline of the sinus externally ( Fig. 63.36 ). Transillumination can also be used to outline the sinus. A light source is placed within the sinus, illuminating the periphery, which is then marked in a similar fashion ( Fig. 63.37 ). After the limits of the sinus have been marked, several microplates are pre-applied across the proposed osteotomy sites ( Fig. 63.38 ), maintaining the precise location of the bone flap at the completion of the procedure. The plate is rotated superiorly and the osteotomy is performed ( Fig. 63.39 ). The author prefers a high-speed Midas Rex drill (Medtronic, Inc.) and a B-1 bit. The same tool can be used to make perforations along the periphery of the sinus ( Fig. 63.40 ), and complete the osteotomy by joining the perforations with side cutting capabilities ( Fig. 63.41 ). The osteotomy line should be angled toward the sinus cavity to avoid intracranial penetration ( Fig. 63.42 ). The orbit rims and glabella can be osteotomized with either the drill or osteotomes depending on the degree of preexisting comminution; however, the surgeon must protect the supratrochlear and supraorbital neurovascular pedicles. Finally, an osteotome is inserted through the superior saw kerf and used to break down any intersinus septations, and bone flap is removed ( Fig. 63.43 ).

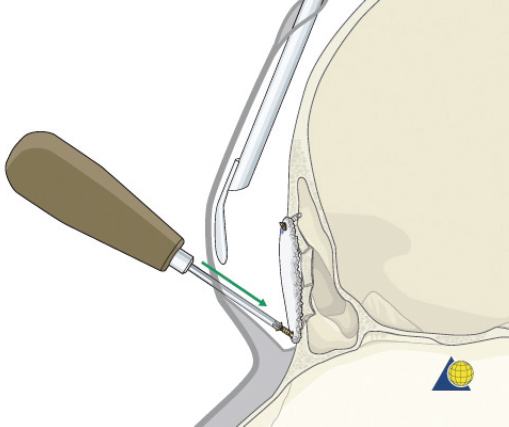
After completion of the sinusotomy, posterior table comminution is assessed and a decision is made regarding sinus obliteration or cranialization. If the sinus is to be obliterated, meticulous debridement of all mucosa is accomplished with both cutting and diamond burs. Special attention must be paid to the periphery of the sinus where complete removal of the mucosa is most challenging ( Fig. 63.44 ). The frontal sinus infundibulum mucosa is elevated inferiorly, and a temporalis muscle plug is placed to occlude each ostia. A sharp 5-mm osteotome is then used to obtain a 5 × 5 mm outer table bone graft that can be wedged into each frontal recess to secure the muscle plug ( Fig. 63.45 ).
Many different materials have been used to successfully obliterate the sinus including abdominal fat, cancellous bone, muscle, pericranium, and spontaneous osteoneogenesis with “auto-obliteration.” While different authors report the “best” success rates with specific materials, 5 , 19 , 20 the author prefers abdominal fat, and feels that success of the procedure is more likely related to the surgical technique (e.g., removal of all sinus mucosa, atraumatic technique, etc.) than the actual material. A fat graft should be obtained in a single piece without the use of electrocautery. It is used to fill the sinus and the bone flap is replaced ( Fig. 63.46 ). Alloplastic materials such as hydroxyapatite cement should be avoided due to a high risk of infection and extrusion. Finally, anterior table stabilization and closure should be completed as described above under “Open Reduction and Internal Fixation.”
Frontal Sinus Cranialization
Injuries that result in significant posterior table comminution or large dural tears should be considered for cranialization. The surgical approach is described above under “Open Reduction and Internal Fixation.” While the procedure can generally be performed through the sinus itself and a formal craniotomy is not generally required, neurosurgical consultation is recommended. It is important to maintain the integrity of the pericranial flap for dural repair and control of any CSF leak. All free bone fragments from the anterior and posterior table are removed, drilled free of any mucosa, and oriented on a side table ( Fig. 63.35 ). Posterior table fragments that are adherent to the dura are freed with a Penfield elevator. The dura is inspected for tears and then elevated behind any stable bone at the periphery of the sinus. A brain retractor ribbon is placed and Kerrison rongeurs and/or a drill are used to smooth the post table edge flush with the sinus walls, floor, and anterior cranial fossa ( Fig. 63.47 ). Simple lacerations of the dura can be repaired with interrupted 5-0 nylon sutures. More complex injuries may require neurosurgical debridement and dural closure. All fragments of the anterior and posterior table are divested of mucosa with a cutting bur.
Each frontal sinus infundibulum is drilled out and occluded as described under “Sinus Obliteration.” The pericranial flap can then be used to cover the frontal recess, fill dead space, and/or repair dural tears. When replacing the anterior table bone, a small bony defect should be fashioned in the anterior table to allow the pericranial flap to pass intracranially without cutting off the blood supply ( Fig. 63.48 ). The preserved bone fragments are then used to reconstruct the anterior table using 1.0- to 1.3-mm microplates. Micromesh can also be very helpful. Inner table frontal sinus bone fragments and outer table calvarial bone grafts can be used as necessary to supplement native bone.
Naso-orbitoethmoid Complex Fractures
Anatomy
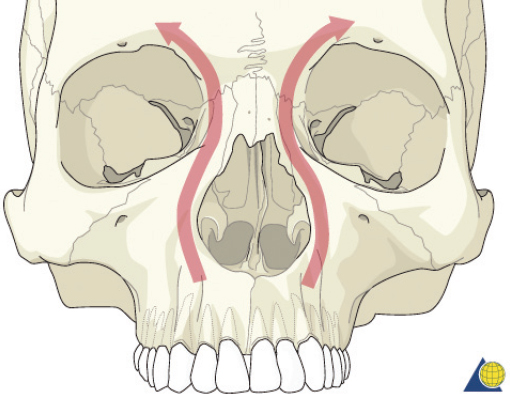
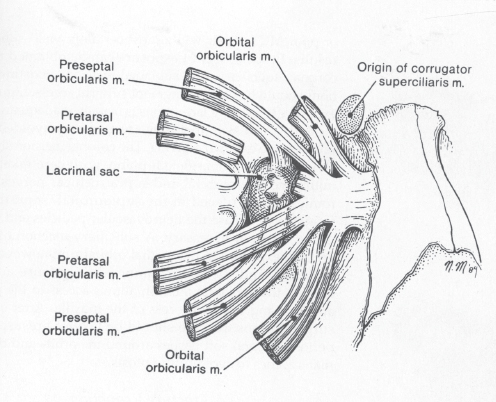
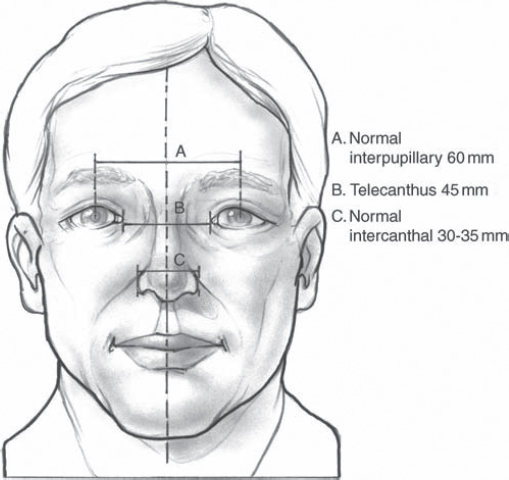
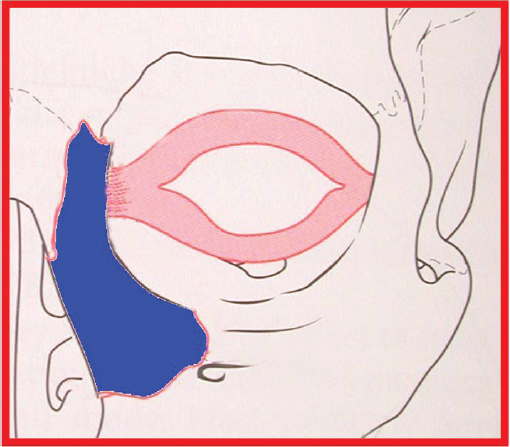
The nasoorbitoethmoid complex represents the confluence of the nasal, lacrimal, ethmoid, maxillary, and frontal bones. It constitutes the underlying support and symmetry for the central midface. The primary vertical buttress of the nasoorbitoethmoid complex is the frontal process of the maxillary bone ( Fig. 63.49 ). The primary horizontal buttresses are the superior and inferior orbital rims. Violation of these buttresses due to nasoorbitoethmoid fractures may result in longterm sequelae including nasal deformity, telecanthus, enophthalmos, midface retrusion, epiphora, CSF fistula, anosmia, sinusitis, and blindness. The medial canthal tendon arises from the anterior and posterior lacrimal crests as well as the frontal process of the maxilla. It surrounds the lacrimal sac and diverges to become the pretarsal, preseptal, and orbital orbicularis oculi muscle ( Fig. 63.50 ). The medial canthal tendon (and its bony attachment) maintains the intercanthal distance and is the focal point of nasoorbitoethmoid fracture repair. Normal intercanthal distance is 30 to 35 mm. This is equivalent to the width of the alar base and onehalf the interpupillary distance ( Fig. 63.51 ).
Diagnosis
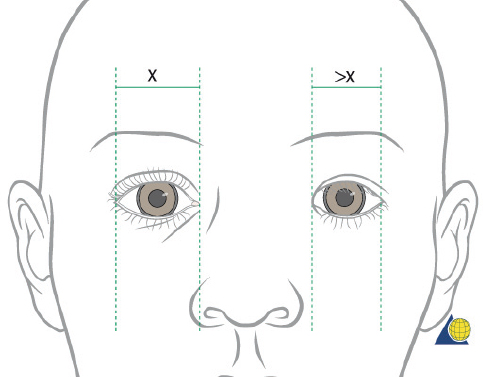
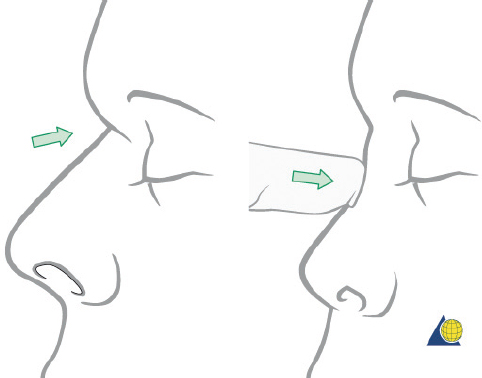
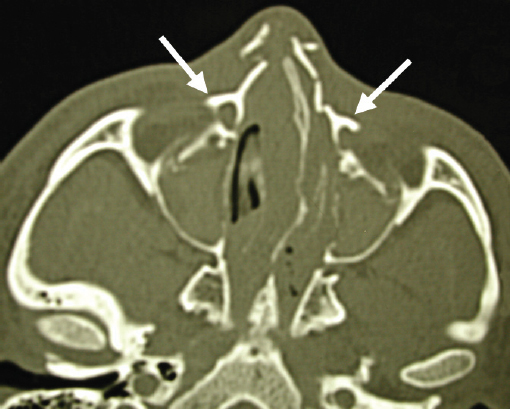
Injuries to the nasoorbitoethmoid complex can be difficult to diagnose, as they may be masked by facial edema. A complete head and neck examination should be performed including the brain, cervical spine, orbits, and presence of CSF leak. Both neurosurgery and ophthalmology consultations may be required. A high degree of suspicion must be maintained because failure to identify these injuries often results in deformities that are extremely difficult to repair secondarily. Physical findings suggestive of a nasoorbitoethmoid fracture include: (1) widening of the intercanthal distance greater than 30–35 mm; (2) blunting of the medial canthus and narrowing of the palpebral fissure width ( Fig. 63.52 ); (3) widening of the nasal dorsum; and (4) rotation, deprojection, and shortening of the nose. The integrity of the medial canthal tendon should be evaluated by carefully applying lateral tension to each lid. Normally, there will be a defined end point to the maneuver, without palpable motion at the canthal insertion ( Fig. 63.53 ). A periosteal elevator can also be inserted through the nose to apply lateral pressure in the same area. A lax medial canthal tendon, or medial orbital wall motion, is consistent with a nasoorbitoethmoid complex fracture. Telecanthus, enophthalmos, pupillary response, and extraocular muscle mobility should be assessed and documented. The degree of nasal or midface retrusion should be assessed. The surgeon should palpate the nasal dorsum at the nasion, rhinion, and tip ( Fig. 63.54 ). If there is significant lack of support along the entire nasal dorsum, an onlay calvarial bone graft will be required. Finally, thin cut (1–1.5 mm) CT scan with coronal, sagittal, and 3D reconstructions plays an important role in defining the pattern and extent of injury. The surgeon must assess the cribriform plate, frontal recess/sinus involvement, orbital integrity, degree of nasoorbitoethmoid complex comminution, and associated facial fractures. Characteristic radiologic findings include: (1) disruption and widening of the nasal dorsum in the coronal plane; (2) a “Y-sign,” occurring when the frontal process of the maxilla/lacrimal bone fractures at the insertion of the canthal ligament, resulting in a Y-shaped bone fragment ( Fig. 63.55 ); (3) depression of the nasal root; and (4) disruption of the frontal recess.

Classification
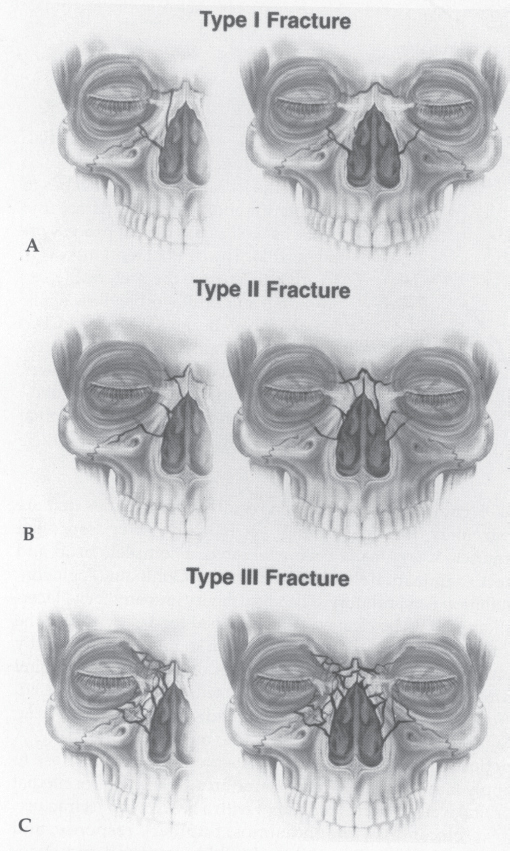
Classification of nasoorbitoethmoid fractures is generally based on the status of the bony central fragment onto which the medial canthal tendon inserts ( Fig. 63.56 ). 22 Markowitz et al devised a classification system describing the degree of bony injury ( Fig. 63.57 ). 23 Type I fractures represent a single, noncomminuted central fragment without medial canthal tendon disruption. Type II fractures involve comminution of the central fragment, but the medial canthal tendon remains firmly attached to a definable segment of bone. Type III fractures are uncommon, and result in severe central fragment comminution with disruption of the medial canthal tendon insertion. Each fracture type is subclassified as either unilateral or bilateral.
Treatment
Surgical Exposure
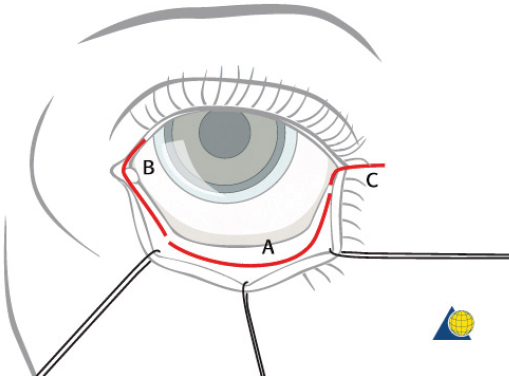
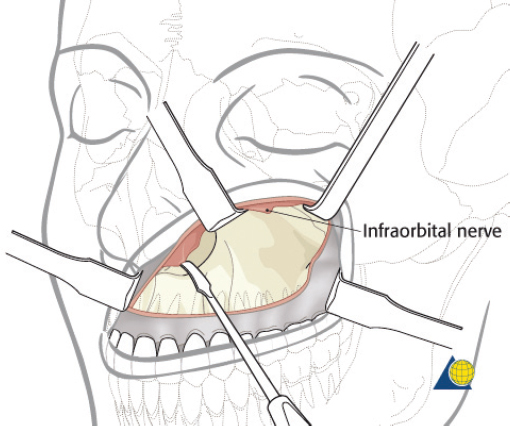
Naso-orbitoethmoid complex injuries are the most challenging of all facial fractures, and surgical repair is often complex and arduous. Inadequate exposure, imprecise fracture reduction, or poor medial canthal tendon repair will almost certainly yield suboptimal results. Some surgeons prefer a direct incision at the glabella ( Fig. 63.58 ); however, many fractures are more involved and require a combination of coronal, transconjunctival, and sublabial incisions. The current author prefers to avoid incisions directly over the medial canthus whenever possible. Existing lacerations are usually inadequate for a complete repair, but should be used to augment surgical access. Brow and “open sky” incisions are generally avoided due to unfavorable external scars and paresthesias. If a coronal incision is used, the supraorbital/supratrochlear neurovascular pedicles can be released to obtain greater exposure of the medial canthal region (described above in the section on open reduction and internal fixation of frontal sinus fractures). A transconjunctival incision offers excellent exposure to the orbital floor, rim, and medial orbital wall while minimizing the risk of postoperative lid malposition ( Fig. 63.59 ). Unfortunately, access to the frontal process of the maxilla is limited with this approach. A small (5 mm), medially based subciliary incision can be used to access this area for screw insertion. Finally, the sublabial incision allows access to the piriform aperture and frontal process of the maxilla ( Fig. 63.60 ).
Type I Fractures
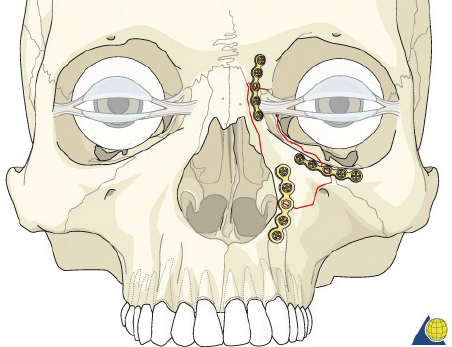
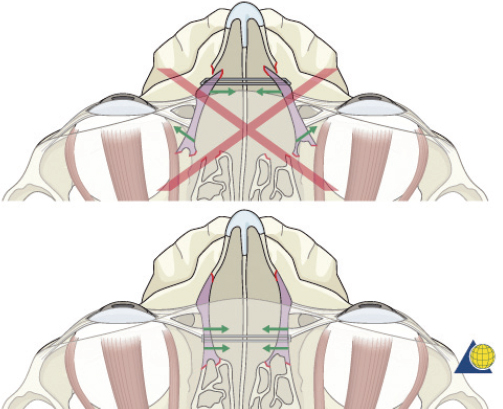
Nondisplaced type I injuries do not require surgical repair. Displaced type I fractures require direct exposure and reduction with one-, two-, or three-point fixation depending on the degree of displacement and instability ( Fig. 63.61 ). Application of a single plate from the frontal bone, across the entire fragment and onto the maxilla, should be avoided. Such placement requires greater elevation of the periosteum on the central fragment, which may disrupt the medial canthal tendon. Plates placed in this region may also widen the nasal root. An accurate reduction must be maintained until all plates are placed or the lateral pull of the medial canthal tendon may result in malreduction. If there is significant suspicion of lacrimal injury, the lacrimal system should be cannulated, with the stent left in place for approximately 6 weeks.
Type II Fractures
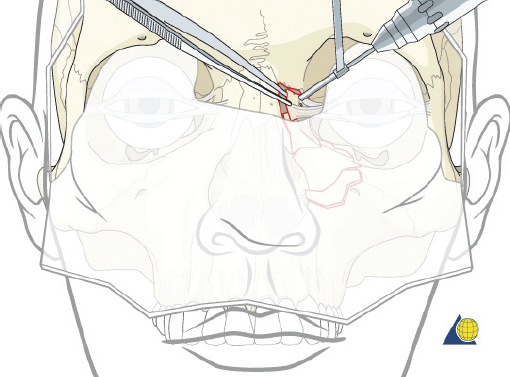
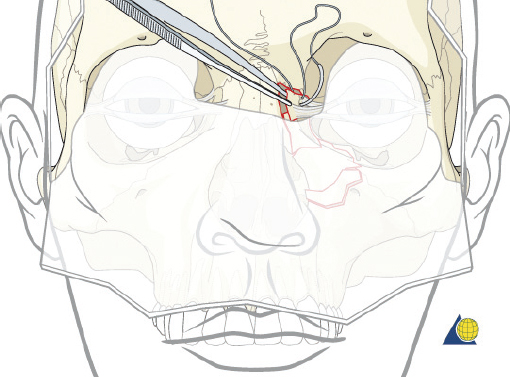
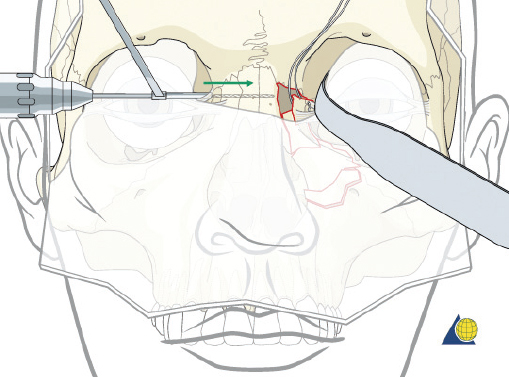
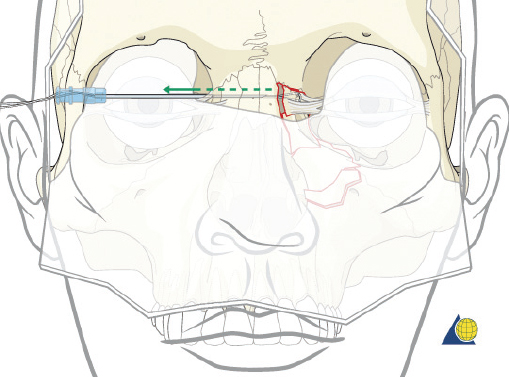
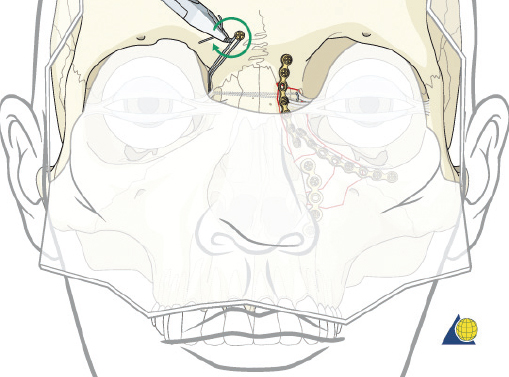
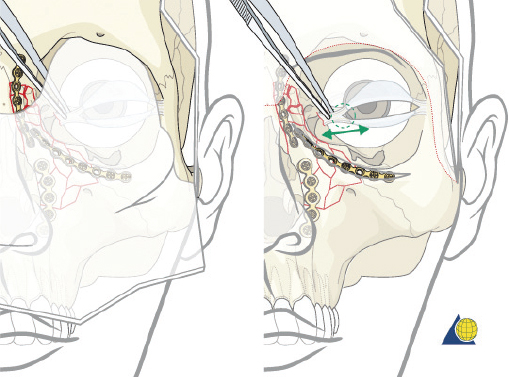
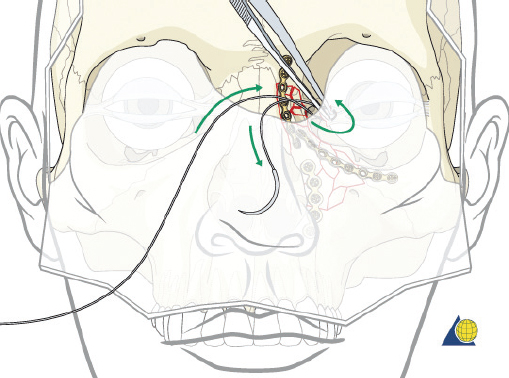
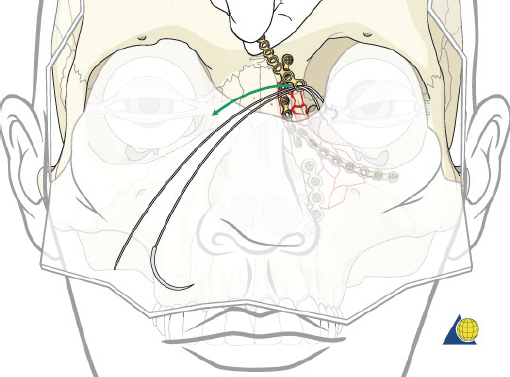
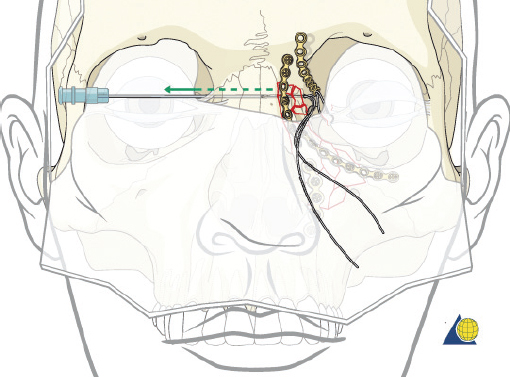
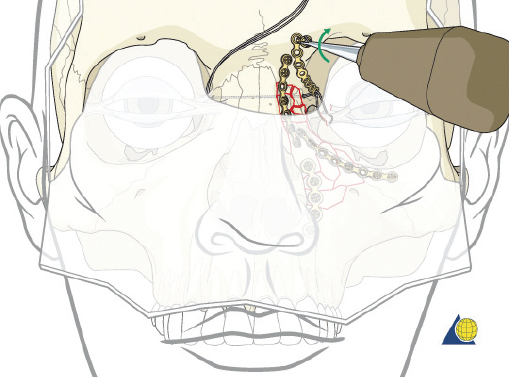
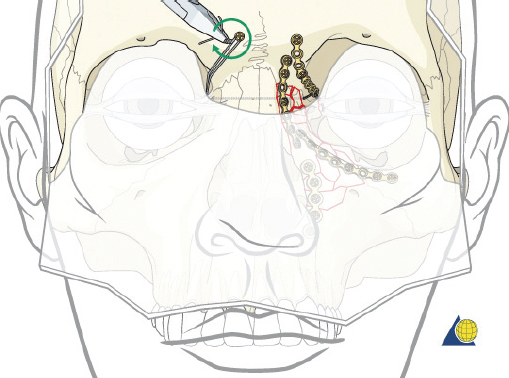
Type II fractures require more extensive surgical exposure, and generally need two- or three-point fixation. A subperiosteal dissection is used to locate, but not avulse, the medial canthal tendon. If the comminution is mild and the central fragment can be plated, the injury is treated as a type I fracture. If the central fragment is too small to be plated, transnasal wires should be used. Transnasal wires are generally easiest to place prior to any osteosynthesis of the surrounding fractures. Initially holes are drilled in the central fragment above and below the medial canthal tendon ( Fig. 63.62 ). Both ends of a 28-gauge wire (or a wire suture) are passed from lateral to medial, leaving the free ends on the medial surface of the central fragment ( Fig. 63.63 ). Once the central fragment is controlled with the wire, a drill may be used to define a transnasal path for passage of the wire ( Fig. 63.64 ). The drill must be passed posterior and superior to the lacrimal fossa, and below the frontoethmoid suture line (to avoid intracranial injury). A 14-gauge spinal needle (or angiocatheter with outer sheath removed) is then passed through the drill hole. The needle is passed in a retrograde fashion, through the ethmoid complex, from the uninjured to the injured side. A malleable retractor is placed medial to the globe on the injured side to provide protection as the spinal needle is passed. The wires are then passed transnasally through the lumen of the needle, and the needle is removed ( Fig. 63.65 ). The wire is then tightened while the central fragment is medialized with external pressure, securing the wire on a miniscrew in the frontal bone ( Fig. 63.66 ). It is critical that tension is maintained on the wire throughout fixation. Any laxity in the wire may allow the medial canthal tendon to lateralize with concomitant loss of fracture reduction. It is difficult, if not impossible, to overcorrect the reduction. Appropriate wire placement posterior and superior to the lacrimal fossa will pull the canthus medially without rotation. Transnasal wires placed anterior to the lacrimal fossa will result in lateral rotation of the central fragment and iatrogenic telecanthus ( Fig. 63.67 ).25
Type III Fractures
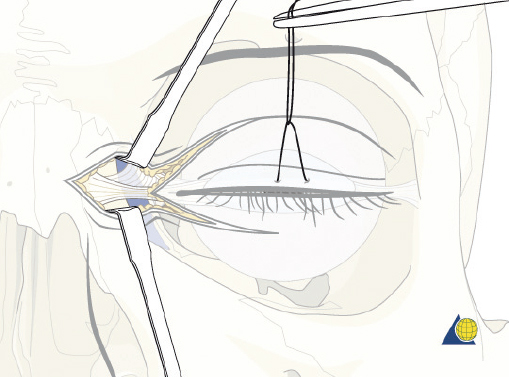
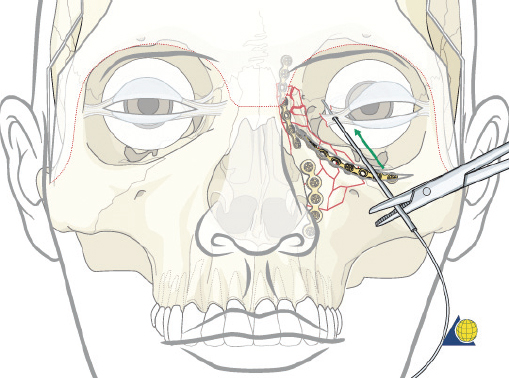
Type III fractures are the result of more severe trauma with comminution of the frontal process of the maxilla and nasal dorsum. Wide surgical exposure is obtained via coronal, transconjunctival, and sublabial incisions. The frontal process of the maxilla is generally comminuted requiring three-point fixation as previously described ( Fig. 63.61 ). It is critical that the surgeon continue to re-check each point of reduction as the plates are sequentially applied. The medial canthal tendon remnant is then identified through the coronal or limited glabellar incision. Forceps are used to pull on the deep surface of the tendon while watching for corresponding skin movement externally at the medial canthus ( Fig. 63.68 ). If the canthal tendon is accurately grasped, the surgeon will note a 1:1 relationship between the deep tissue and external skin motion. A 28-gauge wire suture is then passed through the stump of the tendon twice ( Fig. 63.69 ). While a transnasal wire can then be passed as described under type II fracture, bony disruption of the medial orbital walls often precludes accurate placement of the wire in the proper 3D position. Therefore, a cantilever technique is chosen instead.
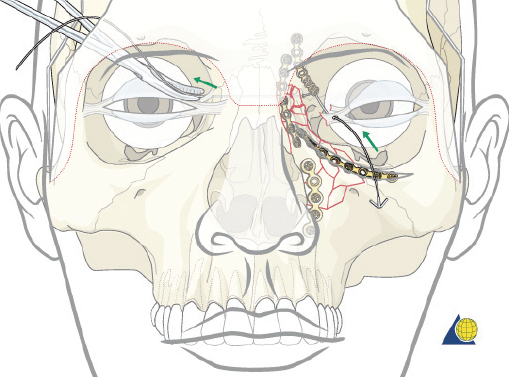
The cantilever technique involves adaption of a miniplate to run across the inferior aspect of the frontal bone and into the medial, anterior orbit in such a way that the deepest hole corresponds to the location that a transnasal wire would be passed (e.g., posterosuperior to the lacrimal fossa) ( Fig. 63.65 ). Before the plate is fixated, the wire suture attached to the avulsed medial canthal tendon is passed through the deepest hole of the plate ( Fig. 63.70 ). The wire is then passed transnasally, via a spinal needle, to the contralateral orbit ( Fig. 63.71 ). Disruption of the medial orbit often alleviates any need for drilling. A malleable retractor should be used to protect the globe while passing the spinal needle across the skull base. Screws are then placed into the frontal bone to align the distal hole of the miniplate in the correct 3D position for the canthal ligament reconstruction ( Fig. 63.72 ). Finally tension is placed on the wire while external pressure is applied to assist with medialization of the injured canthus. The final location of the canthal repair is confirmed and the transnasal wire is anchored to a screw placed on the contralateral frontal bone ( Fig. 63.73 ). An alternative technique for repair of the medial canthal tendon is the use of a canthal barb ( Fig. 63.74 ). The canthal barb is passed through a small cutaneous incision and through the medial canthal ligament, anchoring the barb within the ligament ( Figs. 63.75 and 63.76 ). The wire is then passed transnasally as described above and anchored on the contralateral frontal bone. Alternatively, the canthal barb can be placed through the miniplate and anchored on the ipsilateral. This has the advantage of avoiding transnasal wire placement, however sliding the wire through the plate becomes much more challenging due to the acute angle of placement.
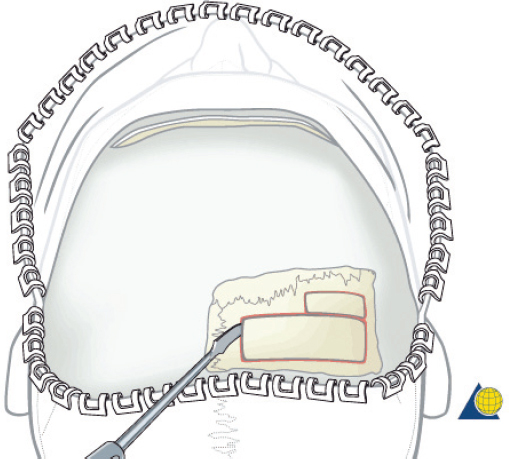
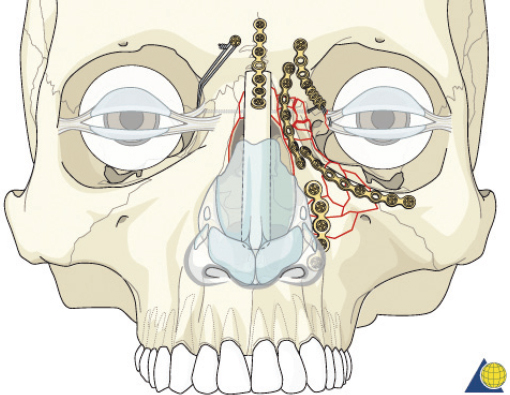
If bone grafting of the nasal dorsum is required, it is done as the final step in the reconstruction. An outer table calvarial bone graft is generally harvested from the flattest area of the parietal bone. It should be at least 6–7 cm in length ( Fig. 63.77 ). A bur should be used to thin and mold the graft to reconstruct a normal nasofrontal angle (105–120 degrees) and extend as far as is necessary to provide a normal nasal contour and tip support. An open rhinoplasty approach can be very helpful for insertion and positioning of the graft. A small trough should be drilled into the glabella to accept the superior aspect of the graft. A miniplate or two position screws are placed to cantilever the graft off the frontal bone ( Fig. 63.78 ). The inferior aspect of the graft should be inserted below the lower lateral cartilages. The septum can be suspended from the bone graft if necessary.
External bolsters are required for any procedure involving significant dissection over the central fragment (generally type II and III injuries). This will help to prevent hematoma formation and restore a normal nasal contour. Aquaplast nasal splints (Aquaplast Corp), padded with several layers of Xeroform (Invacare) gauze, are applied to the lateral nasal side wall. A 14-gauge spinal catheter (or angiocatheter with outer sheath removed) is passed transcutaneously across the nasal base at the level of the medial canthus, as well as at the inferior aspect of the nasal bones ( Fig. 63.79 ). One 26-gauge wire is passed through each needle and bolster. The wires are twisted together on each side to apply mild pressure and reduce soft tissue edema. Postoperatively, the underlying tissue should be closely observed to avoid tissue necrosis. The bolsters are removed at 7 to 10 days.

Disruption of the delicate ethmoid complex and comminution of the nasal bones can make the repair of nasoorbitoethmoid fractures extremely difficult. These injuries often test the capabilities of even the most experienced surgeons. To obtain an aesthetic surgical result, the surgeon must meticulously identify and precisely reduce/fixate the central fragment. Special attention must also be focused on the overlying soft tissue to avoid hematoma, excessive scaring, and telecanthus.
Acknowledgment
The author gratefully acknowledges the AO Foundation of Davos, Switzerland, for many of the figures included in this chapter. They are used with kind permission from the AO Surgery Reference (www.aosurgery.org), a website designed and updated by AOCMF (http://www.aocmf.org). The AOCMF is a part of the AO Foundation that serves as a voice and professional resource for craniomaxillofacial trauma and reconstruction worldwide, and includes the specialties of Otolaryngology/Facial Plastic Surgery, Oral and Maxillofacial Surgery, Plastic Surgery, Ophthalmology, and Neurosurgery. Education is the major pillar of the AOCMF, and more than 2,500 surgeons participate in over 110 AOCMF courses held worldwide each year. The AOCMF is committed to remaining in the forefront of new developments as it strives to improve education. Membership in AOCMF provides surgeons with expanded access to the Surgery Reference, as well as online access to teaching videos, scientific journals, and online discussions with other surgeons having a common interest in craniomaxillofacial trauma.
The figures credited herein as “Courtesy of the AO Foundation” are copyrighted and all such rights are in possession of the AO Foundation. Therefore these figures can only be used, reproduced, displayed and/or duplicated with the express written approval of the AO Foundation. All and any commercial use, reproduction, display, and/or duplication are subject to a respective written agreement. While the AO has allowed use of the images, the methods described do not necessarily reflect AO technique.
References
1. Anon JB, Rontal M, Zinreich SJ. Anatomy of the paranasal sinuses. New York: Thieme; 1996 2. Stammberger HR, Kennedy DW. Paranasal sinuses: anatomic terminology and nomenclature. Ann Otol Rhinol Laryngol 1995; 167:7-16 3. Nahum AM. The biomechanics of maxillofacial trauma. Clin Plast Surg 1975;2(1):59-64 4. Strong EB, Pahlavan N, Saito D. Frontal sinus fractures: a 28-year retrospective review. Otolaryngol Head Neck Surg 2006; 135(5):774-779 5. Wallis A, Donald PJ. Frontal sinus fractures: a review of 72 cases. Laryngoscope 1988;98(6 Pt 1):593-598 6. Yavuzer R, Sari A, Kelly CP, et al. Management of frontal sinus fractures. Plast Reconstr Surg 2005;115(6):79e-93e; discussion 94e-95e 7. Chen KT, Chen CT, Mardini S, Tsay PK, Chen YR. Frontal sinus fractures: a treatment algorithm and assessment of outcomes based on 78 clinical cases. Plast Reconstr Surg 2006;118(2): 457-468 8. Rohrich RJ, Hollier L. The role of the nasofrontal duct in frontal sinus fracture management. J Craniomaxillofac Trauma 1996; 2(4):31-40 9. Harris L, Marano GD, McCorkle D. Nasofrontal duct: CT in frontal sinus trauma. Radiology 1987;165(1):195-198 10. Heller EM, Jacobs JB, Holliday RA. Evaluation of the frontonasal duct in frontal sinus fractures. Head Neck 1989;11(1):46-50 11. Landsberg R, Friedman M. A computerassisted anatomical study of the nasofrontal region. Laryngoscope 2001;111(12): 2125-2130 12. Smith TL, Han JK, Loehrl TA, Rhee JS. Endoscopic management of the frontal recess in frontal sinus fractures: a shift in the paradigm? Laryngoscope 2002;112(5):784-790 13. Kim KS, Kim ES, Hwang JH, Lee SY. Transcutaneous transfrontal approach through a small peri-eyebrow incision for the reduction of closed anterior table frontal sinus fractures. J Plast Reconstr Aesthet Surg 2010;63(5):763-768 14. Chu EA, Quinones-Hinojosa A, Boahene KD. Trans-blepharoplasty orbitofrontal craniotomy for repair of lateral and posterior frontal sinus cerebrospinal fluid leak. Otolaryngol Head Neck Surg 2010;142(6):906-908 15. Strong EB, Buchalter GM, Moulthrop TH. Endoscopic repair of isolated anterior table frontal sinus fractures. Arch Facial Plast Surg 2003;5(6):514-521 16. Kim KK, Mueller R, Huang F, Strong EB. Endoscopic repair of anterior table: frontal sinus fractures with a Medpor implant. Otolaryngol Head Neck Surg 2007;136(4):568-572 17. Graham HD, 3rd, Spring P. Endoscopic repair of frontal sinus fracture: case report. J Craniomaxillofac Trauma 1996;2(4):52-55 18. Strong EB, Kellman RM. Endoscopic repair of anterior tablefrontal sinus fractures. Facial Plast Surg Clin North Am 2006; 14(1):25-29 19. Rodriguez ED, Stanwix MG, Nam AJ, et al. Twenty-six-year experience treating frontal sinus fractures: a novel algorithm based on anatomical fracture pattern and failure of conventional techniques. Plast Reconstr Surg 2008;122(6):1850-1866 20. Rohrich RJ, Hollier LH. Management of frontal sinus fractures. Changing concepts. Clin Plast Surg 1992;19(1):219-232 21. De Cordier BC, de la Torre JI, Al-Hakeem MS, et al. Endoscopic forehead lift: review of technique, cases, and complications. Plast Reconstr Surg 2002;110(6):1558-1568; discussion 1569-1570 22. Leipziger LS, Manson PN. Nasoethmoid orbital fractures. Current concepts and management principles. Clin Plast Surg 1992; 19(1):167-193 23. Markowitz BL, Manson PN, Sargent L, et al. Management of the medial canthal tendon in nasoethmoid orbital fractures: the importance of the central fragment in classification and treatment. Plast Reconstr Surg 1991;87(5):843-853
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


